Percutaneous Coronary Intervention for Coronary Artery Disease
정 명 호
전남의대 전남대병원 순환기내과 광주 동구 학동 8번지 Myung Ho Jeong, M.D.
Department of Cardiovascular Medicine
Chonnam National University Medical School & Hospital E-mail : [email protected]
R
ecently the incidence of coronary artery disease has been increasing in Korea. Percutaneous coronary intervention (PCI) has been established as one of the most effective therapeutic methods in addition to medical therapies, especially for patients with acute coronary syndrome (ACS). ACS refers to unstable angina (UA), non-ST segment elevation myocardial infarction (NSTEMI), and ST segment elevation myocardial infarction (STEMI). UA`/`NSTEMI is a common but heterogeneous disorder with patients exhibiting a wide variety of risks. In patients with UA`/`NSTEMI, early risk stratification is at the center of the manage- ment program and can be achieved by using clinical criteria, electrocardiographic changes and biomarkers, or both. Platelet glyco- protein (GP) IIb/IIIa receptor blockers are indicated in high-risk patients who are likely to undergo PCI, but are not indicated in the management of lower risk patients who do not undergo PCI. There is a hard evidence to support the substitution of the low-molecular weight heparin for unfractionated heparin. Many recent trials have demonstrated the benefit of an early invasive strate- gy with coronary angiography followed by PCI in patients at high and intermediate risk. Prompt reperfusion of ischemic myocardi- um is the major focus of acute treatment of patients with STEMI. Two reperfusion strategies have been developed: thrombolytic therapy and primary PCI. Although these two strategies have traditionally been considered distinct and at times competing options, it is likely that the care of patients with STEMI will be improved in the future if they are viewed as a single integrated effort for reperfusion. However, PCI has been shown to be superior to thrombolysis in the treatment of STEMI admitted to highly experienced PCI centers. A meta-analysis of many randomized trials found significantly lower mortality rate, and lower rate of nonfatal reinfarction and intracerebral hemorrhage with primary PCI compared with thrombolysis. Currently, a primary PCI strate- gy may begin with the initiation of a platelet GP IIb/IIIa receptor blocker in the emergency center, together with aspirin and heparin (especially low molecular weight heparin), followed by rapid application of coronary angioplasty with stenting. Primary PCI is feasi- ble in community hospitals without surgical capability, however, due to the concerns about timing and safety margin, this approach is not yet advocated in the current guidelines.
Keywords : Angina; Myocardial infarction; Percutaneous coronary intervention; Thrombolysis 핵 심 용 어 : 협심증 ; 심근경색증 ; 관상동맥 중재술; 혈전용해
Abstract
서 론
최
근 관상동맥질환이 국내에서도 급증하고 있으며, 협심증 및 심근경색증 환자에서 약물요법과 더불 어 경피적 관상동맥 중재술(percutaneous coronary intervention, PCI)의 시술이 늘어나고 있다. 특히 최근 에 불안정형 협심증(unstable angina, UA)과 비ST 분 절 상승/ST 분절 상승 심근경색증(non-ST segment elevation/ST segment elevation myocardial infarc- tion, NSTEMI, STEMI)과 같은 급성 관상동맥 증후군 (acute coronary syndrome, ACS) 환자에 대한 치료가 관심을 끌고 있다.ACS는 UA와 NSTEMI 및 STEMI 등을 일컬으며 UA나 NSTEMI의 기본적인 병리생태학적 기전은 동일 하다. 대부분의 ACS는 비폐쇄성 혈전 생성에 의해 야기 된다. ACS의 치료는 관상동맥의 죽상반(atherosclerotic plaque)의 균열, 파열로부터 심근허혈, 심근괴사에 이 르는 여러 단계의 병태생리학적 과정을 목표로 하는 다 양한 치료방법으로 이루어지고 있다. STEMI의 경우는 신속하게 재관류를 시키는 것이 가장 중요하고 UA/
NSTEMI의 경우는 죽상반을 안정화(stabilization), 수 동화(passivation)하여 병의 진행을 억제하고 혈전의 재발이나 혈관의 수축을 예방하는 것이 필요하다. 심근 의 산소 요구/공급의 균형은 심박 수, 후부하, 수축력, 전부하를 조절함으로써 이루어지는데, 나이트레이트, 베타차단제, 칼슘 길항제 등이 이런 목적으로 사용되어 지고 있다.
경피적 관상동맥 풍선확장술(percutaneous translu- minal coronary angioplasty, PTCA)은 1977년 Grunt- zig에 의해 처음으로 시행되었다. 1990년대에 이르러 관 상동맥 중재술의 기술과 약물의 발달로 인하여 PTCA는
다혈관 질환, 완전폐쇄병변, 불안정형 협심증, 급성 심근 경색증과 같은 대부분의 관동맥 질환 분야에 도입되게 되 었다. 최근에 풍선확장술인 PTCA 뿐만 아니라 스텐트 시술, 죽상종 절제술 등을 모두 포함하여 PCI로 일컬어 지고 있다. PCI 시술의 간편성, 국소마취만의 필요, 짧은 재원기간, 시술의 짧은 회복시간 등과 같은 PCI의 장점 은 PCI의 보편화를 이끌었고 매년 전 세계적으로 약 150 만건의 PCI가 시술되고 있다. 본 교실에서도 1990년대 전반기에는 연간 200여건, 후반기에는 1,000여건, 2000 년대 초반에는 1,500여건을 시술하고 있으며, 2003년도 에는 2,384건을 시술하여 그 시술 건수가 급증하고 있다.
관상동맥질환 치료의 목표는 환자의 증상을 없애고 사 망이나 심근경색증의 위험을 감소시키는 데 있다. 관상동 맥 풍선 확장술이나 스텐트 시술과 같은 PCI는 대부분의 환자의 증상을 경감시키고 사망이나 심근경색증과 같은 심각한 합병증을 감소시키지만, 스텐트의 급성 혈전성 폐 쇄나 재협착과 같은 문제점이 남아있다.
관상동맥 중재술의 기전 및 기술적 측면
PCI는 fluoroscopy를 이용하여 경피적으로 관상동맥 병변을 치료한다. 국소 마취를 통하여 대개 대퇴동맥이나 요골동맥을 hollow-bore needle로 천자하고 대개 5~8F 크기의 sheath를 삽입한다. 이후 특별한 모양의 guiding catheter를 유도 철선을 따라 대동맥을 통해 관 상동맥의 개구부까지 진행시킨다. 현재까지 수 많은 guiding catheter의 개발로 인해 PCI technique의 눈부 신 발전을 이루었다. Diagnostic catheter에 비해 guid- ing catheter는 더 stiff한 shaft를 가지며 내경이 더 넓 고 더 짧고 각진 tip(110°vs 90°)과 re-enforced con- struction을 가진다. Guiding catheter는 aortic root의
넓이, coronary ostial origin(high, anterior), ostial orientation(superior, horizontal, inferior) 등에 기초 하여 선택할 수 있다. 이 guiding catheter를 통해 조영 제를 주사하여 관상동맥을 조영하고 병변이 있는 관상동 맥으로 약 0.014 inch의 guidewire를 삽입한다.
Guidewire는 central core 혹은 shaft(대개 stainless steel이나 nitinol), distal flexible spring coil(대개 platinum 혹은 tungsten), lubricous coating(silicone, PTFE, 혹은 다른 hydrophilic coating) 등 3가지 기본 구성요소를 갖추고 있다. Whisper 혹은 ChoicePT wire 는 simple-to-complex PTCA에 이용되며 심하게 tor- tuous하거나 tight lesion을 cross 할 수 있다. Shinobi wire는 uncrossable lesion에 유용하며 ATW wire는 simple-to-complex lesion에 이용되며 stent delivery 에 유용하다. CrosswireNT는 chronic total occlusion 에 유용하며 그 이외에 BMW wire, Cross-IT 200XT, Cross-IT 300XT wire 등이 임상에 이용되고 있다. 이 guidewire를 통해 inflatable balloon, stent, 그리고 atherectomy catheter를 병변 segment로 삽입한 후 병
변 부위를 치료하게 된다(그림 1).
Balloon catheter(그림 2)는 대개 두 개의 내강으로 이루어져 있다. 하나의 내강으로는 guidewire가 통과하 고 하나의 내강은 식염수와 조영제의 혼합물이 원위부 catheter tip에 위치한 풍선을 부풀리는 데 이용된다.
Fluoroscopy 투시 하에서 balloon을 병변의 중심부에 위 치시킨 후 3~20기압으로 부풀려서 혈관을 확장시킴으로 써 좁아진 내강을 넓히게 된다. PTCA에 흔히 이용되는 balloon에는 ART balloon, Maverick balloon, cutting balloon, Hayate balloon, Arashi balloon, Stormer balloon, Rx balloon, U-pass balloon 등이 있다. 관상 동맥 스텐트는 대개 316 L stainless steel이나 nitinol 등의 금속물질로서 deflated balloon catheter 위에 쪼그 라진 채로 부착되어 있다. Balloon inflation 중에 이 쪼 그라진 스텐트는 팽창되어 혈관 내강을 지지하게 된다.
Balloon은 좁아진 혈관을 적절하게 부풀리기는 하지만 좁아진 병변 혈관에 거친 통로를 개통시키는 데 그치는 반면 스텐트는 원래 혈관 내강만큼으로 충분히 넓힐 수 있고 혈관 내막박리를 치료할 수 있으며 elastic recoil을 줄인다. Coronary atherectomy device에는 directional 그림 1. 관상동맥 중재술 시술방법. 유도 도자(guiding ca-
theter, A)를 관상동맥 개구부에 위치시킨 후 풍선 도자(balloon catheter, B)를 가느다란 유도 철선 (guide wire, C)을 따라서 병변에 위치시키고 확장 시킴.
그림 2. 풍선 도자. 풍선 도자는 두개의 내강을 가지고 있으 며, 하나는 유도 철선을 통과시키고 하나는 풍선을 부풀리는 데 사용함.
A
B
C
coronary atherectomy(DCA), transluminal extrac- tion catheter(TEC), high-speed rotational atherec- tomy(rotablator), pullback atherectomy catheter (PAC), rotary atherectomy system(X-Sizer) 등이 있다. DCA는 일차적으로는 atherosclerotic tissue를 잘 라서 제거함으로써 이차적으로는 Dottering effect를 통 해 좁아진 관동맥 내경을 넓힌다. 현재 DCA는 내경 3 mm 이상의 de novo lesion, bifurcation lesion, ostial lesion, 그리고 스텐트 내 재협착 병변 등의 치료에 사용 된다. Rotational atherectomy(RA)는 140,000~
200,000 rpm으로 고속 회전하면서 관상동맥 내의 athe- rosclerotic tissue를 제거하는 기술이다. RA는 관상동맥 내의 병적인 석회화 조직은 제거하고 병이 없는 혈관 조
직은 남기는 differential cutting이 그 원리이다. RA를 통해 혈관 내 atherosclerotic tissue는 적혈구의 크기보 다 작은 2`~5 μm 크기로 절개되어 미세 순환을 통해 이 동되어 reticuloendothelial system에 의해 제거된다.
RA가 적응될 수 있는 병변으로는 American College of Cardiolog/American Association (ACC/AHA) type B2 이상의 complex lesion, long lesion, ostial lesion, chronic total occlusion, restenotic lesion, angulated lesion, stent restenosis 등의 치료에 이용될 수 있다.
성공적으로 PCI를 마친 이후에 모든 catheter를 제거 하고 동맥 천자 부위를 직접 압박하거나 여러 device를 사용하여 지혈한다. 특별한 합병증이 없으면 환자는 시술 3~6시간에 움직일 수 있으며 동맥 천자 부위에 이상이 Suspected ischemia on ECG
Very low risk (<1%)
Low risk (approximately
4%)
Intermediate risk (approximately
8%)
High risk (>16%)
No Yes
No
Suspected myocardial infarction on ECG
Yes
Two or more risk factors No risk
factors
One risk factor
Zero or one risk factor
Two or more risk factors
그림 3. 흉통을 주소로 내원한 환자 중 심근경색증이 의심되는 환자를 72시간 내에 주요 심장 사건이 발생할 확률에 따라 4군 으로 분류함.
없고 심전도나 심근 효소치가 안정되어 있으면 시술 다음 날 아침에 퇴원할 수 있다.
불안정형 협심증/비ST 분절 상승 심근경색증
1. ACS의 위험도 분석
ACS이 의심되는 환자에서 진단을 내리는 것 뿐만 아 니라 적극적인 치료를 요하는 합병증이 발생할 위험도를 평가하는 것이 중요하다(그림 3)(1). 저위험도군에서는 아스피린과 베타 차단제를 처방하여 외래에서 치료하는 것이 가능하다. 중등도 위험도나 고위험군에서는 심장 중
환자실에 입원하여 다양한 약물을 투여하고 관상동맥 조영술을 시행하 여 필요한 경우 관상동맥 중재술을 시행하여야 한다. ACS의 위험도는 표 1과 같다. 20분 이상 지속되는 흉 통이 있고 심전도에서 적어도 1 mm 이상의 ST 분절의 변화가 있거나 심 각한 좌심실 기능 부전을 보이는 경 우는 고위험군으로 분류하며 안정 시에 흉통이 없거나 65세 미만, 정상 심전도, 심근경색증의 과거력이 없는 경우는 저위험군으로 분류된다. 적절 한 약물치료에도 불구하고 지속되는 흉통과 심전도에서 ST 분절의 변화 가 있으면 심근경색증으로 진행할 가 능성이 높으므로 즉각적인 관상동맥 조영술을 통해 관상동맥 중재술을 시 행하여야 한다(그림 4, 5)(2, 3).
혈중 트로포닌의 측정은 ACS 환 자의 위험도를 평가하는 데 유용한 지표로 이용될 수 있다. 트로포닌 복합체는 심근의 칼 슘-매개성 수축 과정을 조절하는 3가지 아형으로 구성 된다. 여기에는 칼슘과 결합하는 트로포닌 C, 액틴과 결 합하여 액틴-마이오신 상호작용을 억제하는 심근 특이 적인 트로포닌 I(cardiac specific troponin I, cTnI)와 트로포마이오신과 결합하여 트로포닌 복합체와 부착하는 심근 특이적인 트로포닌 T(cardiac specific troponin T, cTnT)로 구성된다. cTnT의 대부분은 트로포닌 복합체에 부착되어 존재하나 6% 정도는 세포질에 용해된 상태로 존재하며 cTnI는 약 2~3%가 세포질에 존재한다.
Troponin은 심근과 skeletal muscle에 존재하지만 이들 표 1. 급성 관상동맥 증후군 환자에서 사망 혹은 심근경색증 발생 위험도 분류
High risk
At least one of following features must be present : Prolonged, ongoing (>20min) rest pain
Pulmonary edema
Angina with new or worsening mitral regurgitation murmurs Rest angina with dynamic ST changes of at least 1 mm Angina with S3 or rales
Angina with hypotension Intermediate risk
No high-risk features but must have any of the following :
Rest angina now resolved but not low likelihood of coronary disease Rest angina (>20 min or relieved with rest or nitroglycerin)
Angina with dynamic T-wave changes Nocturnal angina
New-onset Canadian Cardiovascular Society class III or IV angina in past 2 weeks but not low likelihood of coronary disease Q waves or ST depression of at least 1mm in multiple leads Age > 65 years
Low risk
No high-risk or intermediate-risk feature but may have any of the following : Increased angina frequency, severity, or duration
Angina provoked at a lower threshold
New-onset angina within 2 weeks to 2 months Normal or unchanged ECG
은 각각 다른 유전자에 의해 encode되어 아미노산 서열 이 다르다(4). 이러한 사실은 심근에서 유리되는 cTnT와
cTnI에 특이적인 항체를 생산하게 만들었고 enzyme-linked assay를 통한 심근 특이적인 정량적인 측정 법을 개발하게 되어 Food and Drug Administration(FDA)의 승 인을 받게 되었다(5). cTnI나 cTnT 는 정상인의 혈중에서는 발견되지 않는다. 이러한 트로포닌은 심근 세 포가 여러가지 상황에 의해 손상을 받을 때 혈중으로 유리되어 나온다.
심근 손상시 세포질에 존재하는 트 로포닌이 먼저 혈중으로 유리되고, 이어서 심근섬유에 부착되어 있는 트로포닌이 서서히 혈중으로 유리된 다(6).
UA 환자에 있어서 트로포닌의 상 승은 환자의 불량한 예후와 관련이 있 다. Antman 등(7)은 내원시 cTnI가 0.4 ng/mL 이상인 경우에 0.4 ng/
mL 미만인 경우보다 내원 6주 이내 사망할 확률이 높다고 하였고(3.7%
vs. 1.0%), 혈중 cTnI 수치가 증가 할수록 사망률은 증가한다고 하였 다. cTnI의 상승은 여러가지 다른 인 자를 보정한 이후에도 독립적인 예 후인자로 작용한다고 하였다. 본 교 실의 연구(8)에서는 UA로 내원한 230명의 환자를 트로포닌 양성 유무 와 심전도상 ST 분절 하강 유무에 따라 분류하였을 때 트로포닌 양성인 경우에 심한 관상동 맥 협착을 보였고 다혈관 질환이 많았고 보고 1년간 추적 High/Intermediate Risk
MANAGEMENT OF UA / NSTEMI
Cor. Arteriography
LMCD, 3VD+LV Dys., or Diab. Mell.
CABG
1 or 2VD, suitable
for PCI Normal
Clopidogrel, llb/llla inhib.
Consider Alternative Diagnosis
PCI
Discharge on ASA, Clopidogrel, Statin, ACE-1
MANAGEMENT OF UA / NSTEMI Lower Risk
Stress Test
+High Risk +Not High Risk Negative
Coronary Arteriography
Clopidogrel, Statin, ACEI, Outpatient Rx
Consider Alternative Diagnosis
High-Risk Strategy
그림 4. UA/NSTEMI 환자 중 고위험군 및 중등도 위험군 환자의 치료(위편) 및 저위험도 환자군 치료(아래편)
LMCD : 좌주간지 병변 VD : 혈관 질환
LV Dys : 좌심실부전증 ASA : 아스피린
ACE-I : 안지오텐진 전환효소억제제
관찰하였을 때 무사고 생존율이 낮았다고 하였다. 이와 같이 협심증 환자에서 트로포닌의 상승은 그 진단적 의미 뿐 아니라 예후를 결정하는 데도 중요한 역할을 한다.
ACS의 위험도를 평가하는 데 이용되는 또 다른 중요 한 요소는 Thrombolysis In Myocardial Infarction
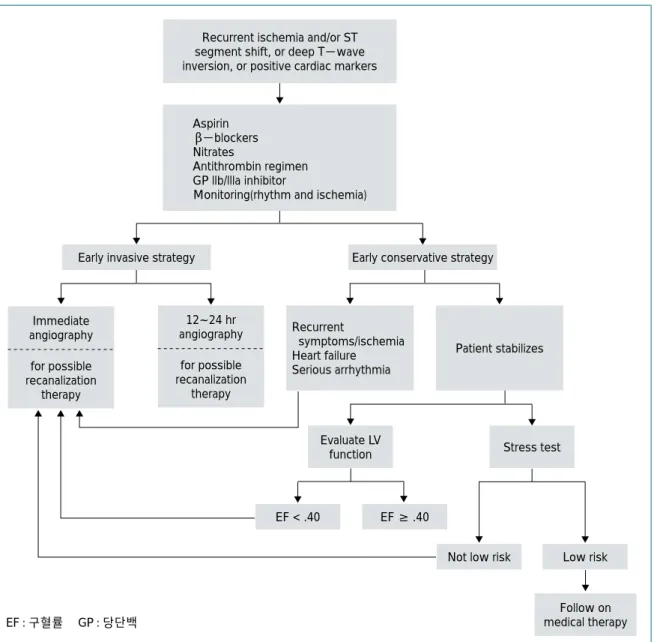
(TIMI) risk score로서 여기에는 7가지 인자가 있는데 이에는 65세 이상의 고령, 3가지 이상의 관상동맥질환의 위험인자의 존재, 50% 이상의 관상동맥 협착의 과거력, 심전도에서 ST 분절의 변화, 이전 24시간 이내에 2번 이 상의 흉통, 최근 1주 이내에 아스피린 사용력, 심근 효소 Recurrent ischemia and/or ST
segment shift, or deep T-wave inversion, or positive cardiac markers
Aspirin β-blockers Nitrates
Antithrombin regimen GP llb/llla inhibitor
Monitoring(rhythm and ischemia)
Early invasive strategy Early conservative strategy
Immediate angiography for possible recanalization
therapy
12~24 hr angiography
for possible recanalization
therapy
Recurrent
symptoms/ischemia Heart failure Serious arrhythmia
Patient stabilizes
Evaluate LV
function Stress test
EF < .40 EF ≥ .40
Not low risk Low risk
Follow on medical therapy
그림 5. 고위험군 환자 치료방법 EF : 구혈률 GP : 당단백
치의 상승이 포함된다. TIMI risk score가 낮을수록 event rate가 낮 고, TIMI risk score가 높을수록 event rate이 높다.
2. 관상동맥 중재술
처음부터 특별한 적응증이 없는 한 내과적 치료와 비관혈적인 검사 를 우선 실시하여 고위험군에서 관 상동맥 조영술이나 중재술을 실시하 는 early conservative strategy와 특별한 금기가 없는한 처음부터 관 상동맥 조영술을 실시하여 관상동맥 재개통술을 적극적으로 권장하는 early invasive strategy가 있으며 각각의 방침에는 합리적인 근거를 가지고 있다.
1999년 ACC/AHA guideline의 early invasive strategy의 적응증 은 강력한 항허혈 치료에도 불구하 고 안정시 또는 경한 활동에도 협심 증상이나 심근허혈이 반복되는 경 우, 반복되는 협심증상이나 허혈이 있으면서 심부전 증상, 제 3심음, 폐 수종, 승모판막 폐쇄부전증이 새로 생기거나 악화된 경우, 비관혈적 검 사에서 고위험 소견이 있을 때, 비관 혈적 검사에서 좌심실 기능이 저하 된 경우(구혈률 < 40%), 혈역학적 으로 불안정하며 흉통이 있을 때, 저 혈압을 동반하는 경우, 지속적인 심
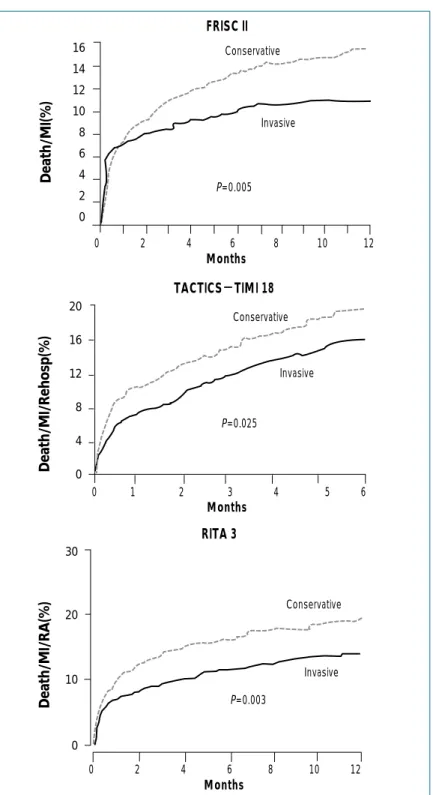
16 14 12 10 8 6 4 2 0
0 2 4 6 8 10 12 Conservative
Conservative
Conservative FRISC II
TACTICS--TIMI 18
RITA 3
Months Months Months
Invasive
Invasive
Invasive P=0.005
P=0.025
P=0.003 20
16
12
8
4
0
0 1 2 3 4 5 6
0 2 4 6 8 10 12 30
20
10
0
Death/MI(%)Death/MI/Rehosp(%)Death/MI/RA(%)
그림 6. FRISC II, TACTICS-TIMI 18 및 RITA 3 연구에서 사망/심근경색증/
재관류 요법/재입원율의 조기 관혈적 방법 및 보존적 방법의 비교
실성 빈맥, 최근 6개월 이내에 PCI를 시행받은 경우, 과 거에 관상동맥 우회술을 받은 경우이다.
그러나 진행중인 허혈이나 고위험 소견이 없더라도 ACS가 재발하는 경우와 65세 이상 환자 또는 혈관 재개 통술에 금기가 없으면서 ST절 하강이 있거나 심근 손상 의 지표가 양성인 환자에서도 early invasive strategy를 선택할 수 있다.
TIMI ⅢB 연구(9)에서 1,473명의 불안정형 협심증 (unstable angina, UA), 비Q파 심근 경색증(Non-Q wave myocardial infarction, NQMI) 환자를, VAN- QWISH 연구(10)에서 920명의 NQMI 환자를 대상으로 invasive strategy와 conservative strategy를 무작위 비교하였을 때 유사한 결과를 보였다. 그러나 최근의 FRISC Ⅱ연구(11)에서는 3,048명의 ACS 환자를 대상 으로 dalteparin으로 5~7일간 치료하고, 이 중 2,457명 의 위험성이 아주 높지 않는 환자들을 대상으로 daltepa- rin vs. placebo , invasive vs. non-invasive treat- ment 로 무작위 비교하였을 때 6개월 후의 임상결과를 보면 delteparin의 계속 사용 유무에 따른 차이는 없었으 나 사망, 심근경색증의 발생률이 invasive군이 9.4%, non-invasive군이 12.1%(P=0.031), 1년 내 사망률은 invasive군 2.2%, non-invasive군 3.9%(p=0.016)로 서 invasive군이 유의하게 좋았다. 또한 TACTICS-
TIMI 18 연구(12)는 2,220명의 ACS 환자(UA, NSTE- MI)를 대상으로 conservative strategy와 invasive strategy를 무작위로 비교하였을 때 30일의 사망이나 심 근경색증의 빈도는 invasive arm이 4.7%, conservative arm이 7.0%였고 6개월간 사망, 심근경색증, 재입원의 빈도를 invasive arm이 conservative arm에 비하여 22% 감소시켰다. RITA 3 연구(13)도 conservative treatment에 비해 invasive treatment의 우월성을 증명
하였다(그림 6).
따라서 UA/NSTEMI 환자에서 invasive treatment 가 환자의 임상적 경과를 향상시키는 데 중요한 역할을 하며, 본 교실에서도 고위험군 ACS 환자에서 조기에 관 혈적인 치료를 시행하고 있다.
3. 저분자량 헤파린
저분자량 헤파린(low molecular weight heparin, LMWH)은 기존의 heparin에 비해서 비교적 예측이 가 능한 항응고효과를 나타내고 aPTT monitoring이 필요 없으며 피하주사로 쉽게 투여할 수 있다는 장점이 있어서 점차 기존의 미분획 heparin을 대체해 나가고 있다.
FRISC 연구(14)에서는 아스피린을 복용한 ACS 환자에 서 dalteparin에 대한 효과를 비교하였는데, 위약에 비하 여 사망과 심근경색증의 발병률을 40일까지 유의하게 줄 일 수 있었으나 초기 6일째와 45일까지의 사망, 심근경 색, 재관류의 시행 및 재발성 협심증 등의 발생을 줄이지 는 못하였다. 그러나 본 교실의 연구에서는 dalteparin의 사용이 PCI를 시술받은 UA 환자에서 장기간 임상경과 를 개선시켰다(15).
FRAXIS 연구(16)에서는 불안정형 협심증과 ST 분절 상승이 없는 심근경색증 환자에서 nadroparin을 투여하 여 사망, 심근경색증 및 난치성 또는 재발성 협심증의 발 생을 줄이지 못하였고 출혈성 합병증이 보다 많이 발생하 였다.
Enoxaparin에 대한 연구로는 ESSENCE(17)와 TIMI 11B(18)가 있는데, ESSENCE 연구에서는 3,171예의 불안정형 협심증과 ST 분절 상승이 없는 심근경색증 환 자를 대상으로 unfractionated heparin을 정맥 주사한 군과 enoxaparin을 매일 2회 피하 주사한 군을 비교하여 enoxaparin 투여군에서 사망, 심근경색증, 재발성 협심
증 등의 발생이 14일째 유의하게 적었으며(16.6% vs.
unfractionated heparin 투여군 19.8%, P=0.02), 이 는 30일째(19.8% vs. 13.3%, P=0.02)와 1년 후 (31.9% vs. 35.7%, P=0.02)에도 계속 유지됨을 보고하 였다. TIMI 11B 연구에서도 8일째 사망, 재발성 심근경 색증, 긴급 재관류 요법의 필요성 등이 enoxaparin 투여 군 12.4%, unfractionated heparin 투여군 14.5%로 enoxaparin 투여군에서 유의하게 낮음을 보고하였다.
본 교실의 연구에서도 PCI를 시술받은 ST절 비상승 심근경색증 환자에서 tirofiban과 저분자량 헤파린인 dalteparin의 병합요법은 장기간 임상 효과를 개선시켰 다(19).
4. 혈소판 당단백 IIb/IIIa 수용체 차단제
혈소판 응집의 최종 단계에 관여하는 platelet glyco- protein(GP) Ⅱb/Ⅲa 수용체를 차단하는 약제로 현재 사용되는 것들은 chimeric monoclonal antibody인 abciximab과 eptifibatide(synthetic peptide), tiro- fiban(non-peptide) 등이 있다. 관상동맥 중재술에서 GP Ⅱb/Ⅲa 억제제의 효과는 대규모의 비교 임상연구에 서 정립되었다. Abciximab은 EPILOG(20), EPIS- TENT(21) 연구에서 0.25 mg/kg를 bolus injection한 후 12시간 동안 0.123 ㎍/kg/min의 속도로 점적하는 것 이고, heparin은 70 U/kg를 bolus로 투여하고 ACT를 200초 이상 유지하도록 하는 저용량의 heparin을 정주하 되 PCI 후에는 heparin을 중단하는 방법이 가장 효과적 이고 안전한 표준 투여방법으로 사용되고 있다. Epti- fibatide의 경우 PURSUIT 연구(22)에서와 같은 180 ㎍/
kg bolus 투여 후 2.0 ㎍/kg/min로 정주하는 것이 적합 한 용량으로 권장되고 있다. 이 약제들은 UA/NSTEMI 환자의 PCI시에 사용함으로써 사망률, 심근경색증, 재시
술의 필요성을 감소시킬 수 있음은 많은 연구들에서 입증 되었다(20~26). 또한 UA/NSTEMI 환자의 초기 내과 적 치료시에도 GP Ⅱb/Ⅲa의 사용은 사망과 심근경색증 을 감소시킬 수 있었다(24, 27). 즉 Abciximab을 이용한 EPIC, EPILOG, EPISTENT, CAPTURE 연구들에서 는 약제 사용군에서 30일의 MACE를 4.5~6.5% 정도로 감소시켰고, tirofiban을 이용한 RESTORE 연구(28)에 서는 2.5%, eptifibatide를 이용한 IMPACTⅡ 연구에서 는 1.5% 감소시켰다. 또한 장기적인 효과는 EPIC, EPICOG, EPISTENT의 1년 이상 추적 연구에서 관찰 되어 있다. TACTICS-TIMI 18 연구(25)에서는 아스피 린, 헤파린과 함께 tirofiban을 투여하고 조기 중재시술 과 보존적 치료를 비교하였는데, 조기 중재시술군에서 심 근경색의 발생이 33% 감소하였다. 현재까지 연구 결과 들을 종합해 보면 GP Ⅱb/Ⅲa 억제제들은 UA/NSTE- MI 환자에서 조기 PCI 치료전략의 선택시에 그 효과가 탁월하고 특히 고위험군에서 유용한 것으로 생각된다.
5. Drug-eluting stent 1) Sirolimus-coated stent
Sousa 등(29, 30)이 진행한 소규모 연구에서 신생내막 증식 억제에 양호한 결과를 보인 이후로 두 개의 세계적 인 대규모 연구결과가 발표되었다. RAVEL study(31) 는 238명의 native 관상동맥 병변(vessel 직경 2.5~3.5 mm)에 대하여 18 mm 길이의 sirolimus 부착 스텐트와 bare 스텐트를 비교한 연구로서 sirolimus 부착 스텐트 는 무사고 생존율 96.5%, 재협착률 0%라는 경이적인 결 과를 보여주었다. 스텐트 혈전증은 한 예에서도 없었다.
이러한 효과는 sirolimus 부착 스텐트 시술 초기 환자들 의 2년간의 subgroup 분석에서도 신생내막형성의 억제 효과가 그대로 유지됨을 보여 주었다(32). SIRIUS 연구
(33)는 미국 내에서 1,100명의 de-novo 관상동맥 병변 환자를 대상으로 시행된 연구로서 비교적 복잡병변에 대 해 시행된 연구이다. 연구 결과 일차 종결점인 target vessel failure(TVF)는 59% 감소(21% with control vs 8.6% sirolinus), target lesion revascularization(TLR) 은 75% 감소(16.6% with control vs 4.1% with siroli- mus), 재협착률은 in-stent 3.2%(control 35.4%), in-
segment 8.9%(control 36.3%)로서 RAVEL에서 보여 주었던 것과 동일한 결과를 보여 주었다. 이것은 대단히 인상적이며 경이롭다고까지 할 수 있다. 뿐만 아니라 심 한 복잡 재협착 병변에 시술한 sirolimus 부착도 신생 내 막 형성과 4개월 관상동맥 조영술에서 반복적인 재협착 을 억제하는 결과를 보여 주었다(34). Holmes 등(35)은 sirolimus-eluting stent 시술 환자 533예와 대조 bare 표 2. ReoProⓇ stent 및 대조 스텐트 시술 환자의 관상동맥 내 초음파 소견
EEM : 외탄력막 (external elastic membrane), CSA : 단면적 (cross sectional area), P & M : 죽상종 및 중막 (plaque and media), NIH : 신생내막증식 (neointiam hyperplasia)
ReoProⓇstent (n=43)
Control stent
(n=42) p value
Preintervention
Proximal reference EEM CSA(mm2) 14.2±3.1 13.7±2.8 0.232
Lesion site EEM CSA(mm2) 13.8±3.6 12.7±3.9 0.204
Lesion site lumen CSA(mm2) 4.1±1.0 4.0±0.8 0.777
Lesion site P&M CSA(mm2) 9.7±3.2 8.7±3.6 0.280
Lesion site plaque burden (%) 70.3±6.3 66.5±8.5 0.119
Distal reference EEM CSA(mm2) 12.7±3.2 12.4±2.8 0.604
Postintervention
Stent CSA(mm2) 7.8±2.2 7.7±1.4 0.898
lumen CSA(mm2) 7.8±2.2 7.7±1.4 0.898
NIH area(mm2) 0.0±0.0 0.0±0.0 1.000
Follow--up
Proximal reference EEM CSA(mm2) 14.1±3.5 13.5±3.0 0.211
Stent CSA(mm2) 7.7±2.0 7.6±1.5 0.178
Intrastent lumen area(mm2) 5.7±1.6 4.2±0.8 0.001
Intrastent NIH area(mm2) 2.0±1.6 3.4±1.7 0.001
Distal reference EEM CSA(mm2) 12.4±2.8 12.1±2.4 0.587
Serial (after intervention to follow--up) comparison
Proximal reference EEM CSA(mm2) -0.1±0.7 -0.2±1.0 0.821
Stent CSA(mm2) -0.1±1.1 -0.1±1.2 0.978
Intrastent lumen area(mm2) -2.1±1.6 -3.5±1.8 0.001
Intrastent NIH area(mm2) -2.0±1.6 -3.4±1.7 0.001
Distal reference EEM CSA(mm2) -0.3±1.2 -0.3±1.4 0.967
stent 시술 환자 525예 등 1,058예의 환자에서 9개월에 표적 병변 재개통술은 각각 4.1%, 16.6%(P`<`0.001), 12개월에 각각 4.9%, 20%로서 sirolimus-eluting stent 시술 환자군에서 유의하게 낮았다고 보고하였다 (P`<`0.001). Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital(RESEARCH) re- gistry(36)는 sirolimus-eluting stent군 508예와 bare stent군 450예에서 1년 표적 병변 재개통술은 각각 3.7%와 10.9%(HR, 0.35 [95% CI, 0.21 to 0.57]; P`<
0.001)였고, 1년간 사망, 심근경색증, 표적병변 재개통술 과 같은 주요 심장 사고는 각각 9.7%와 14.8%(hazard ratio [HR], 0.62 [95% CI, 0.44 to 0.89] ; P=0.008) 로서 sirolimus-eluting stent군에서 유의하게 낮았다 고 보고하였다.
2) Paclitaxel-coated Stent
최근 시행된 paclitaxel-coated 스텐트 연구들을 보면 다음과 같다. 아시아에서 진행된 ASPECT trial, 유럽에 서 진행된 ELUTES trial, 미국에서 진행된 PATENCY trial, Taxol derivate인 Quanam QP2 stent를 이용한 SCORE trial, 그리고 DELIVER, TAXUS trial 등이 있다. ASPECT trial은 우리나라를 비롯한 아시아권에서 이루어진 연구로서 IVUS가 가능하였던 81명의 환자를 대상으로 스텐트 재협착에 유의한 억제효과가 있음을 발 표하였다(신생내막 증식 정도 31±22 mm3in control, 18±15 mm3 in low dose, and 13±14 mm3 in high dose, P`<`0.001)(37).
또한 paclitaxel을 이용한 TAXUS I 연구의 6개월, 12 개월 결과에서도 주요 심장사고 3% with paclitaxel 10% with control, 재협착 0%, 10% with control이라 는 우수한 결과를 보였다(38). TAXUS-IV 연구(39)는
1,314명의 환자를 대상으로 하였고 TAXUS 스텐트군에 서 대조 스텐트군에 비해 12개월 target lesion revascu- larization율을 73%(4.4% versus 15.1%, P`<`0.0001), TLR을 62%(7.1% versus 17.1%, P`<`0.0001), TVF를 52%(10.0% versus 19.4%, P`<`0.0001), 주요 심장 사 고를 49%(10.8% versus 20.0%, P`<`0.0001) 감소시 켰다.
3) Estradiol-coated stent
최근 30명의 환자를 대상으로 17-beta estradiol coated BiodivYsio stent의 재협착 억제효과를 본 EASTER 연구(40)에서 late loss 0.54±0.44 mm, 재협 착률 6.6%, TLR 3.3%의 양호한 결과를 보여 estradiol 의 항증식 작용에 대해 대규모 연구를 기다리고 있다. 본 교실에서도 17-beta estradiol을 Dispatch catheter를 이용하여 국소전달한 후 스텐트를 시술하였을 때 돼지 관 상동맥 재협착 모형에서 신생내막의 증식을 유의하게 감 소시켰음을 보고한 바 있다(41).
4) ReoProⓇ-coated stent
Abciximab은 중재시술 초기 24~48시간 동안 증가되 는 염증 표지자인 C-reactive protein, interleukin-6, tumor necrosis factor-a가 감소시키는 항염증 효과 (42)와 중성구나 단핵구의 표면에 존재하는 수용체로 세 포의 접합(adhesion)과 백혈구와 혈소판의 상호작용 및 혈관손상에 대한 염증반응에 주요한 역할을 하는 CD 11b/18(macro-phage-1 receptor) receptor와 ab-
ciximab이 교차반응을 함으로써 세포와 세포외기질의 관 계를 방해하고 세포 사이의 접착력을 차단하는 작용을 갖 고 있다(43).
본 교실에서는 보건복지부의 연구비 지원을 받아
ReoProⓇ부착 스텐트를 동물심도자 실에서 개발하여 안정성과 그 효과 를 입증한 후 2001년 8월부터 2002 년 10월까지 본 교실에서 PCI를 시 술받았던 환자 99예(ReoProⓇ 부착 스텐트 시술 48예, 대조 스텐트 시술 51예)를 대상으로 시행한 전향적인 임상연구에서 추적 관상동맥 조영 술의 재협착률은 14.6%, 29.4%로 서 ReoProⓇ부착 스텐트 시술군에서 더 낮았고, late loss는 각각 0.33±
0.28 mm, 0.88±0.41 mm로서 Reo- ProⓇ부착 스텐트 시술군에서 유의 하게 적었다(44). 이 환자 중 추적 관상동맥 초음파가 가능했던 85예 (ReoProⓇ 부착 스텐트 시술 43예, 대조 스텐트 시술 42예)의 결과는 표 2와 같아서 ReoProⓇ부착 스텐트는 대조 스텐트에 비해 유의하게 신생 내막 증식을 억제하였다(45).
급성 심근경색증
1. 응급실에서 치료
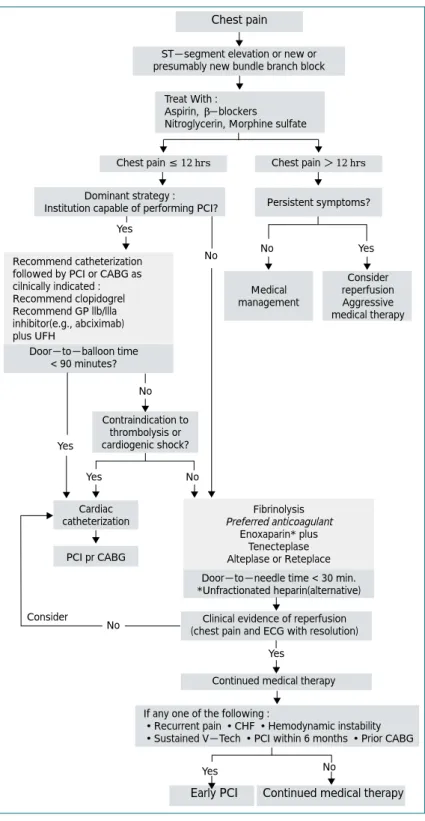
AMI가 의심되는 환자가 응급실에 도착하면 신속히 초기 평가를 시행 하고 조기에 재관류 치료를 시행하 는 것을 지체해서는 안된다. 응급실 에 AMI 환자가 내원했을 때의 치료 방침은 그림 7과 같다.
응급실에서 치료의 목표는 급성
Yes No Recommend catheterization
followed by PCI or CABG as cilnically indicated : Recommend clopidogrel Recommend GP llb/llla inhibitor(e.g., abciximab) plus UFH
Door-to-balloon time
< 90 minutes?
Medical management
Contraindication to thrombolysis or cardiogenic shock?
PCI pr CABG
Fibrinolysis Preferred anticoagulant
Enoxaparin* plus Tenecteplase Alteplase or Reteplace Door-to-needle time < 30 min.
*Unfractionated heparin(alternative)
Clinical evidence of reperfusion (chest pain and ECG with resolution)
Continued medical therapy
Early PCI Continued medical therapy Consider reperfusion Aggressive medical therapy No Yes
Yes
No
Yes
Cardiac catheterization
No Yes
If any one of the following :
•Recurrent pain •CHF •Hemodynamic instability
•Sustained V-Tech •PCI within 6 months •Prior CABG Yes No
Consider
No
Dominant strategy :
Institution capable of performing PCI? Persistent symptoms?
Chest pain ≤ 12 hrs Chest pain > 12 hrs Chest pain
ST-segment elevation or new or presumably new bundle branch block
Treat With : Aspirin, β-blockers
Nitroglycerin, Morphine sulfate
그림 7. 급성 ST 분절 상승 심근경색증 환자에서 근거에 의한 효과적인 치료방법
흉통을 보이는 다른 질환과 AMI 환자를 즉시 감별하여 즉각적인 치료에 돌입하는 것이다. 지속적인 심전도 모니 터링을 시행하고 정맥 내 수액을 주입하며 혈액을 채취하 여 심근 효소를 비롯한 여러 혈액 검사를 실시한다. 그리 고 즉시 재관류요법 중 혈전용해 치료를 할 것인지(응급 실 도착 이후 20~30분 이내), 아니면 primary PCI를 시행할 것인지(관상동맥 조영술까지 60분 이내, PCI까지 60~90분 이내)를 빨리 결정하여야 한다. 아스피린은 금 기가 아닌 모든 환자에게 투여하여야 하며 대부분의 환자 에서 헤파린의 투여가 필요하다. 흉통이 있는 환자에게는 니트로글리세린 설하정을 투여하고 심한 통증에는 몰핀 을 사용한다. 베타차단제는 특히 고혈압, 빈맥, 지속되는 흉통이 있는 경우 효과적이다. 저산소증을 막기 위해 산 소를 공급하고 혈압은 100~140 mmHg 사이로 유지한 다. 고혈압 환자에서 니트로글리세린, 베타차단제 등을 사 용한다. 저혈압 동반시에는 위의 약제를 중지하고 수액 공 급을 실시하며, 혈역학적인 상태에 따른 치료를 시행한다.
증상이 있는 서맥이나 미주신경 항진에 의한 저혈압에 는 아트로핀을 사용하고 가능한 빨리 심혈관계 중환자실 이나 심도자실로 환자를 이동한다.
2. 재관류 치료
심근에 대한 조기 재관류가 AMI 환자의 일차 치료 목표 이다. 관상동맥의 재관류는 혈전용해제 치료나 primary PCI를 통해 이루어질 수 있다. 이러한 관상동맥 재관류요 법을 통해 지난 30년간 AMI 환자의 30일 사망률은 20~30%에서 5~10%로 감소하였다. 여기에서는 AMI 환 자의 관상동맥 중재술 요법에 대해서만 언급하고자 한다.
1) Primary PCI
Primary PCI는 AMI 환자의 생명을 구제할 수 있는
가장 확실한 방법으로 선호되는 관상동맥 재개통 방법이 다. 지금까지 수 많은 연구에서 AMI 환자에서 혈전용해 요법에 비해 PCI가 더 좋은 효과를 가지는 것으로 보고 되 었다(46, 47). AMI 환자의 1차 선상의 치료는 primary PCI이어야 한다는 의견이 지배적이다(48). 최근의 National Registry of Myocardial Infarction 연구(49) 도 AMI 환자에서 primary PCI의 사망률 감소에 대한 효과를 보여 주었다.
PCI를 시행할 것인지, 아니면 혈전 용해요법을 시행할 것인지는 여러가지 인자에 의해 좌우되지만 일반적으로 경험이 많은 병원(>`200 PCIs/yr/center ; 관상동맥 우 회술 가능 ; >`75 PCIs/yr/operator ; frequent primary PCI)에서는 primary PCI가 일반적으로 선호된다(50).
PCI는 심인성 쇼크와 같이 사망할 가능성이 높은 경우, 증상 발현 이후 4시간 이상 경과된 경우, 뇌출혈의 위험 이 높은 경우(70세 이상, 여성, 항고혈압 치료를 받는 경 우 등)에 특히 선호되는 관상동맥 재개통 방법이다. Pri- mary PCI 시작 전에 아스피린, clopidogrel, 헤파린, 혈 소판 당단백 IIb/IIIa 수용체 차단제 등을 미리 사용하는 것이 안전하다.
Wharton 등(51)은 고위험군의 AMI 환자에서 관상동 맥 우회술의 뒷받침이 되지 않는 병원에서 primary PCI 를 바로 시행하는 경우와 관상동맥 우회술의 뒷받침이 되 는 병원으로 환자를 이송해서 primary PCI를 시행하는 경우에 대해 비교하였는데 관상동맥 우회술의 뒷받침이 되는 병원으로 환자를 이송해서 primary PCI를 시행하 는 경우에 비해 바로 primary PCI를 시행한 경우에 30 일 사망률, 재경색증, 뇌졸중이 더 낮은 경향을 보였고 1 년 사망률이 낮은 경향을 보임을 보고하여 고위험군 AMI 환자에서 primary PCI의 안전성과 유효성을 증명 하였다.
Primary PCI의 혈전용해요법과 비교한 장단점은 표 3 과 같다.
DANish trial in Acute Myocardial Infarction (DANAMI-2)(52)와 PRimary Angioplasty in acute myocardial infarction patients for General commu- nity hospitals transported to percutaneous translu- minal coronary angioplasty Units versus Emergency thrombolysis(PRAGUE-2) 연구(53)에서는 PCI를 시 행할 수 없는 병원에 AMI 환자가 내원했을 때 적절한 관 상동맥 재개통 방법이 무엇인가를 연구하였다. DANA- MI-2에서는 alteplase, PRAGUE-2에서는 strep- tokinse를 사용하여 혈전용해요법을 시행했던 경우와 PCI가 가능한 병원으로 환자를 이송하는 경우를 비교하 였는데 이 두 연구 모두에서 PCI가 가능한 병원으로 환 자를 이송하는 경우가 30일 사망률이 유의하게 낮음을 보고하였다. DANAMI-2 연구에서는 24개의 referral hospital에 enroll된 1,129명의 AMI 환자와 5개의 inva- sive-treatment center에 enroll된 443명의 AMI 환자 등 총 1,572명의 AMI 환자에서 관찰한 주요 심장 사고가 referral hospital에서는 primary PCI군에서 8.5%, alteplase군에서 14.2%였고(P=0.002), invasive-
treatment center에서는 primary PCI군에서 6.7%,
alteplase군에서 12.3% (P=0.05) 로 referral hospital과 invasive-
treatment center 모두에서 pri- mary PCI군이 alteplase 사용군 보다 양호한 예후를 보였다. 또한 PRAGUE-2 연구에서도 주요 심 장 사고가 PCI군에서 8.4%, strep- tokinase 사용군에서 15.2%로 PCI 군에서 유의하게 주요 심장 사고가 낮았다. 따라서 referral hospital의 경우에도 혈전용해요 법을 시행하는 것보다 PCI가 가능한 병원으로 환자를 이 송하는 것이 환자의 사망률을 줄이는 것으로 생각된다.
2) Facilitated PCI
현재까지 여러 연구에서 primary PCI가 혈전용해요법 에 비해 좋은 효과를 보여 주었으나 PCI가 가능한 병원 으로 환자를 이송하는 데 오랜 시간이 걸리는 병원에서는 아무런 처치 없이 환자를 이송하는 것은 도의적인 문제를 유발시킬 수 있다. Pharmacoinvasive approach , 즉 facilitated PCI는 PCI 이전에 혈전 용해제 단독요법이 나 혈전 용해제와 혈소판 당단백 IIb/IIIa 수용체 차단제 와의 병합요법으로 경색 동맥을 재개통시킴으로써 관상 동맥 조영술 및 임상경과에서 양호한 예후를 보일 수 있 다는 가설에 근거하는 것이다. GRupo de Analisis de la Cardiopatia Isquemica Aguda(GRACIA-2) 연구 (54)는 abciximab을 사용하면서 primary PCI를 시행한 군과 tenecteplase와 enoxaparin을 사용한 이후에 조 기 PCI를 시행한 군(facilitated group)을 비교하였는데 6시간에 ST 분절 정상화는 facilitated group에서 높았 으나, 6주 후에 경색 범위와 좌심실 기능과 주요 출혈성 합병증에 있어서는 차이가 없었다. Bavarian Reperfusion 표 3. ASTEMI 환자에서 Thrombolysis와 Primary PCI의 장단점 비교
Thrombolysis Primary PCI
•손쉽게 투요할 수 있음
•빠른 시간 내에 투여할 수 있음
•의료진에 따른 차이가 거의 없음
•치료비가 비교적 적음
•효과적인 혈류 개선을 얻을 수 있음
•재발률이 낮음
•뇌출혈을 비롯한 합병증이 적음
•관상동맥 병변을 정확하게 파악할 수 있음
•혈전용해제 금기증에서도 시행 가능함
•심도자실 및 인력이 준비되어야 함
•경험이 많은 관상동맥 중재술 시술의사가
•있어야 함
AlternatiVes Evaluation(BRAVE) 연구(55)는 절반 용량의 reteplase와 abciximab 병합요법 후 즉시 PCI를 시행한 경우와 abciximab만 사용 후 즉시 PCI를 시행한 경우를 비교하였는데 TIMI 3 flow가 병합요법군에서는 높았으나, 경색 범위에 있어서 차이가 없었고 출혈성 합 병증은 오히려 병합요법군에서 높다고 하였다. 따라서 빠 른 시간 내에 PCI를 시행할 수 있는 경우 pharmacoin- vasive approach는 primary PCI에 비해 장점이 없다고 결론내릴 수 있다. 하지만 PCI를 시행하기까지 3시간 이 상이 소요되는 경우라면 facilitated approach를 고려하 여야 한다. 현재 reteplase와 abciximab의 병합요법 후 PCI를 시행하는 경우, abciximab 단독요법 후 PCI를 시 행하는 경우 등 두 가지 facilitated PCI와 abciximab 사 용 후 primary PCI를 시행하는 경우를 비교하는 Faci- litated Intervention with Enhanced Reperfusion Speed to Stop Events(FINESSE) 연구(56)가 진행중이다.
3) Rescue PCI
다양한 종류의 혈전 용해제 투여로 치료받은 AMI 환 자의 약 46%에서 조기 재관류에 실패한다고 알려져 있 다(57~59). AMI 환자에서 혈전 용해제 투여로 재관류 에 실패한 경우에 시행되는 구제적 관상동맥 중재술(res- cue PCI)은 심근 구제에 의해 경색의 크기를 줄이고, 좌 심실 기능을 보존하며, 단기 및 장기 예후를 향상시킨다.
본 교실의 연구(60)에서 1997년부터 1999년까지 rescue PCI를 시행받은 환자와 primary PCI를 시행받은 환자 를 비교하였을 때 1개월 생존율이 각각 93.5%, 94.5%, 6개월 생존율은 93.5%, 93.7%, 12개월 생존율은 90.3%, 91%로 양 군간에 유의한 차이는 없어서 AMI 환 자에서 rescue PCI는 primary PCI와 비교하여 대등한 예후를 보임을 보고한 바 있다. Tadros 등(71)은 AMI에
대한 혈전용해요법 실패 이후 rescue stenting을 시행한 환자와 rescue PTCA를 시행한 환자를 비교하였는데 6 개월 추적 관찰에서 사망률, 심근경색증, 재입원 등의 주 요 심장 사고에 있어서 양 군에 차이가 없었으나(60%
vs. 27%, P=0.06), 재발성 흉통은 스텐트군에서 유의하 게 낮아 rescue PTCA보다 rescue stent 시술을 권고하 였다.
4) Drug-eluting stent
Saia 등(62)은 89명의 ST 분절 상승 AMI 환자에게 sirolimus-eluting stent(SES)를 시술하였을 때 병원 내 사망률은 6.2%였고 조기 혹은 후기 스텐트 혈전은 발 생하지 않았으며 재협착은 없었다고 보고하였다. Lemos 등(63)은 AMI 환자에서 SES를 시술한 186명과 bare metal stent를 시술한 183명을 비교하였을 때 300일째 반복적인 PCI율이 각각 1.1%와 8.2%(P=0.01), 주요 심장 사고는 각각 9.4%와 17%로 SES군에서 유의하게 낮음을 보고하였다(P=0.02). 본 교실의 연구(64)에서 AMI 환자에서 ReoProⓇ부착 스텐트를 시술한 32명과 대조 스텐트를 시술한 31명을 비교하였을 때 재경색이 각각 0%, 6.5%, 반복적인 PCI율은 12.9%, 29% 등 1년 간 주요 심장 사고는 각각 12.9%, 35.5%로서 ReoProⓇ 부착 스텐트 군에서 유의하게 낮음을 보고하였다.
5) Optimal preprocedural therapy in catheteriza- tion laboratory
심도자실에서 PCI 이전에 가장 적절한 preprocedural therapy에 대해서는 아직 논란이 많다. 혈소판 혈전은 관상동맥 중재술 시술중이나 직후에 일어나는 관상동맥 의 급성 폐쇄와 같은 합병증을 일으키는 데 중요한 역할 을 한다. 혈소판 당단백 Ⅱb/Ⅲa 수용체 차단제의 하나인
abciximab은 혈소판 응집의 최종 단계를 차단하는 강력 한 혈소판 응집억제제로서 당뇨병이나 고위험군 PCI의 결과를 향상시키고 단기 및 장기간 사망률 감소 등 주요 심장 사고 감소에 효과적으로 알려져 있다.
본 교실의 연구(65)에서 고위험군 AMI 환자 중 abciximab을 사용하면서 관상동맥 중재술을 시술받았던 환자 68명의 6개월 추적 관찰에서 사망은 4.4%, AMI 1.5%, 반복적인 PCI 25%, 관상동맥 우회술 3%, 주요 출혈성 합병증은 0%로 AMI 환자의 중재시술시 abcixi- mab은 심각한 출혈성 합병증 없이 효과적으로 사용될 수 있음을 보고한 바 있다. Antoniucci 등(66)은 PCI를 시 행한 환자에서 abciximab을 사용하였을 때 사망, 심근경 색증, 관상동맥 재개통술률, 뇌졸중 등의 30일 주요 심장 사고가 감소함을 보고하였다. 또한 Antoniucci 등(67)은 경색 동맥 스텐트 시술시에 abciximab을 사용한 경우가 사용하지 않은 경우보다 1년 생존율이 높았고(95% vs.
88%, P=0.017), 재경색률이 낮음을 보고하였다(1% vs.
6%). 그러나 Controlled Abciximab and Device Investigation to Lower Late Angioplasty Compli- cations(CADILLAC) 연구(68)에서는 abciximab 사용 군에서 약간의 이득이 있을 뿐이었다. 따라서 PCI시에 abciximab의 효과는 좀 더 규명되어야 할 필요가 있다.
결 론
최근 협심증 환자에서 PCI가 가장 확실한 치료법으로 자리매김하였다. 특히 여러 약물 부착 스텐트의 개발은 기존의 스텐트가 안고 있던 가장 큰 단점인 스텐트 재협 착을 획기적으로 줄임으로써 협심증 환자의 치료에 한 획 을 긋는 역할을 하였다. 협심증 환자에서 고위험군을 속 히 발견하고 빠른 시간 내에 PCI를 시행하는 것이 환자
의 생명을 구하고 심근경색증과 같은 심각한 합병증을 막 는 길이다.
AMI 환자가 내원한 경우 금기가 없는 모든 환자에서 아스피린, clopidogrel, 헤파린, 베타 차단제, 안지오텐신 전환효소 차단제를 사용하여야 하며 혈전용해요법을 시 행할 것인지, 아니면 primary PCI를 시행할 것인지는 각 center의 특성에 따라 결정될 수 있다.
급성 심근경색증 환자의 치료에 있어서 혈전용해제보 다 primary PCI가 더욱 효과적이며, 합병증도 적음이 알 려지고 있어서 향후 PCI 시술이 더욱 활발히 전개되리라 생각된다(69, 70).
참 고 문 헌
11. Lee TH, Goldman L. Evaluation of the patient with acute chest
pain. N Engl J Med 2000 ; 342 : 1187 - 95
12. Braunwald E. Application of current guidelines to the manage-
ment of unstable angina and non-ST-elevation myocardial infarction. Circulation 2003 ; 108 : III-28-III-37
13. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin
MD, Smith Jr SC, et al. ACC/AHA guidelines for the manage- ment of patients with unstable angina and non-ST-seg- ment elevation myocardial infarction : A report of the American College of Cardiology/American Heart Association task force on practice guidelines(committee on the management of pa- tients with unstable angina). J Am Coll Cardiol 2000 ; 36 : 970 - 1062
14. Hamm CW. New serum markers for acute myocardial infarc-
tion. N Engl J Med 1994 ; 331 : 607 - 8
15. Wu AH, Apple FS, Gibler WB. National Academy of Clinical
Biochemistry Standards of Laboratory Practice : Recommen- dations for the use of cardiac markers in coronary artery dis- eases. Clin Chem 1999 ; 45 : 1104 - 21
16. Davidson NE, Helzlsouer KJ. Decision making with cardiac tro-
ponin tests. N Engl J Med 2002 ; 346 : 2079 - 82
17. Antman EM, Tanasijevic MJ, Thompson B. Cardiac-specific
troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med 1996 ; 335 : 1342 - 9
18. Lee SH, Jeong MH, Park JS, Kim W, Kim KH, Kang JC, et al.
The long-term clinical significance of troponin and electrocar- diogram in patients with unstable angina. Korean J Med 2001 ; 61 : 506 - 17
19. Anderson HV, Cannon CP, Stone PH, Williams DO, McCabe
CH, Braunwald E, et al. One-year results of the Thrombolysis in Myocardial Infarction(TIMI) IIIB clinical trial. A randomized comparison of tissue-type plasminogen activator versus placebo and early invasive versus early conservative strategies in unstable angina and non-Q wave myocardial infarction. J Am Coll Cardiol 1995 ; 26 : 1643 - 50
10. Boden WE, O'Rourke RA, Crawford MH, Blaustein AS, Deedwania PC, Lavori PW, et al. Outcomes in patients with acute non-Q-wave myocardial infarction randomly assigned to an invasive as compared with a conservative management strategy. Veterans Affairs Non-Q-Wave Infarction Strate- gies in Hospital(VANQWISH) Trial Investigators. N Engl J Med 1998 ; 338 : 1785 - 92
11. Lagerqvist B, Safstrom K, Stahle E, Wallentin L, Swahn E.
FRISC II Study Group Investigators. Is early invasive treatment of unstable coronary artery disease equally effective for both women and men? FRISC II Study Group Investigators. J Am Coll Cardiol 2001 ; 38 : 41 - 8
12. Cannon CP, Weintraub WS, Demopoulos LA, Vicari R, Frey MJ, Braunwald E, et al. for the TACTICS Thrombolysis in Myo- cardial Infarction 18 Investigators. Comparison of early inva- sive and conservative strategies in patients with unstable co- ronary syndromes treated with the glycoprotein IIb/IIIa inhi- bitor tirofiban. N Engl J Med 2001 ; 344 : 1879 - 87
13. Fox KA, Poole-Wilson PA, Hendersen RA, Clayton TC, Chamberlain DA, Pocock SJ, et al. Randomized Intervention Trial of Unstable Angina Investigators. Interventional versus conservative treatment for patients with unstable angina or non-ST elevation myocardial infarction ; the British Heart Foundation RITA 3 randomized trial. Randomized Intervention Trial of Unstable Angina. Lancet 2002 ; 360 : 743 - 51 14. FRISC study group. Low-molecular-weight heparin during
instability in coronary artery disease. Lancet 1996 ; 347 : 561 - 8
15. Hong YJ, Jeong MH, Lee SH, Park OY, Kim JH, Kang JC, et al. The use of low molecular weight heparin in to predict clini- cal outcome in patients with unstable angina that had under- gone percutaneous coronary intervention. Kor J Int Med 2003 ; 16 : 167 - 73
16. Leizorovicz A. The FRAXIS study. XXth Congress of the Euro- pean Society of Cardiology, Vienna, Austria, August 1998 ; 25 17. Cohen M, Bigonzi F, Le louer V, Gosset F, Fromell GS,
Goodman S. One year follow-up of the ESSENCE trial(enoxa- parin versus heparin in unstable angina and non-Q-wave myocardial infarction). J Am Coll Cardiol 1998 ; 31 : 79A 18. Antman EM, McCabe CH, Gurfinkel EP, Turpie AG, Bernink
PJ, Braunwald E, et al. Enoxaparin Prevents Death and Cardiac Ischemic Events in Unstable Angina/Non Q-Wave Myocardial Infarction : Results of the Thrombolysis In Myo- cardial Infarction(TIMI) 11B Trial. Circulation 1999 ; 100 : 1593 - 601
19. Lim SY, Bae EH, Jeong MH, Lee SH, Kim HG, Kang JC, et al.
The clinical effect of Tirofiban with low molecular weight heparin in patients with acute Non-ST segment elevation myocardial infarction. Korean J Med 2003 ; 65 : 527 - 34 20. EPILOG Study. Platelet glycoprotein IIb/IIIa receptor blockade
and low-dose heparin during percutaneous coronary revas- cularization. N Engl J Med 1997 ; 336 : 1989 - 96
21. The EPISTENT Investigators. Randomised placebo-con-
trolled and balloon-angioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein IIb/IIIa blockade. Lancet 1998 ; 352 : 87 - 92
22. The PURSUIT Trial Investigators. Inhibition of platelet glyco- protein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. Platelet Glycoprotein IIb/IIIa in Unstable Angina : Receptor Suppression Using Integrilin Therapy. N Engl J Med 1998 ; 339 : 436 - 43
23. The EPIC Investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty. N Engl J Med 1994 ; 330 : 956 - 61 24. The CAPTURE Investigators. Randomised placebo-con-
trolled trial of Abciximab before and during coronary interven- tion in refractory unstable angina : the CAPTURE Study. Lancet 1997 ; 349 : 1429 - 35
25. Cannon CP, Weintraub WS, Demopoulos LA. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med 2001 ; 344 : 1879 - 87 26. The ESPRIT Investigators. Novel dosing regimen of eptifi-
batide in planned coronary stent implantation(ESPRIT) : a ran- domized, placebo-controlled trial. Lancet 2000 ; 356 : 2037 - 44
27. Platelet Receptor Inhibition in Ischemic Syndrome Manage- ment in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non-Q-wave myocardial infarction. N Engl J Med 1998 ; 338 : 1488 - 97
28. King SB, Willerson JT, Ross AM. for the RESTORE Investi- gators. Time course of reduction in adverse cardiac events fol- lowing angioplasty using a IIb/IIIa receptor blocker, Tirofiban : the RESTORE Trial. Circulation 1996 ; 94 : I - 199
29. Sousa JE, Costa MA, Abizaid A, Abizaid AS, Feres F, Serruys PW, et al. Lack of neointimal proliferation after implantation of
sirolimus-coated stents in human coronary arteries. Circula- tion 2001 ; 103 : 192 - 5
30. Sousa JE, Costa MA, Abizaid AC, Rensing BJ, Abizaid AS, Serruys PW, et al. Sustained suppression of neointimal proli- feration by sirolimus-eluting stents : one-year angiographic and intravascular ultrasound follow-up. Circulation 2001 ; 104 : 2007 - 11
31. Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Falotico R, et al. RAVEL Study Group. Randomized Study with the Sirolimus-Coated Bx Velocity Balloon-Expandable Stent in the Treatment of Patients with de Novo Native Coronary Artery Lesions. A randomized comparison of a sirolimus-
eluting stent with a standard stent for coronary revasculariza- tion. N Engl J Med 2002 ; 346 : 1773 - 80
32. Sousa JE, Costa MA, Sousa AG, Abizaid AC, Seixas AC, Serruys PW, et al. Two-year angiographic and intravascular ultrasound follow-up after implantation of sirolimus-eluting stents in human coronary arteries. Circulation 2003 ; 107 : 381 - 3
33. Moses JW, Leon MB, Popma JJ, et al. for the SIRIUS investi- gators. TCT 2002
34. Degertekin M, Regar E, Tanabe K, Smits PC, van der Giessen WJ, Serruys PW, et al. Sirolimus-eluting stent for treatment of complex instent restenosis : The first clinical experience. J Am Coll Cardiol 2003 ; 41 : 184 - 9
35. Holmes DR Jr, Leon MB, Moses JW, Popma JJ, Cutlip D, Kuntz RE, et al. Analysis of 1-year clinical outcomes in the SIRIUS trial : a randomized trial of a sirolimus-eluting stent versus a standard stent in patients at high risk for coronary restenosis. Circulation 2004 ; 109 : 634 - 40
36. Lemos PA, Serruys PW, van Domburg RT, Saia F, Arampatzis CA, de Feyter PJ, et al. Unrestricted utilization of sirolimus-
eluting stents compared with conventional bare stent implan- tation in the "real world" : the Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital(RESEARCH) re-
gistry. Circulation 2004 ; 109 : 140 - 2
37. Hong MK, Mintz GS, Lee CW, Song JM, Han KH, Park SJ, et al. ASian Paclitaxel-Eluting Stent Clinical Trial. Paclitaxel coat- ing reduces in-stent intimal hyperplasia in human coronary arteries : a serial volumetric intravascular ultrasound analysis from the ASian Paclitaxel-Eluting Stent Clinical Trial(ASPECT).
Asian Paclitaxel-Eluting Stent Clinical Trial. Circulation 2003 ; 107 : 517 - 20
38. Grube E, Silber S, Hauptmann KE, Mueller R, Buellesfeld L, Russell ME, et al. TAXUS I : six-and twelve-month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circula- tion 2003 ; 107 : 38 - 42
39. Stone GW, Ellis SG, Cox DA, Hermiller J, O'Shaughnessy C, Russell ME, et al. One-Year Clinical Results With the Slow-
Release, Polymer-Based, Paclitaxel-Eluting TAXUS Stent : The TAXUS-IV Trial. Circulation 2004 ; 109 : 1942 - 7 40. Abizaid A, Albertal M, Costa MA, Abizaid AS, Staico R, Sousa
JE, et al. First human experience with the 17-beta-estra- diol-eluting stent : the Estrogen And Stents To Eliminate Restenosis(EASTER) trial. J Am Coll Cardiol 2004 ; 43 : 1118 - 21
41. Kim W, Jeong MH, Hong YJ, et al. The effects of local estra- diol delivery in a porcine setnt restenosis model. Korean Cir- culation J 2002 ; 32 : II - 121
42. Lincoff AM, Kereiakes DJ, Mascelli MA. Abciximab suppres- ses the rise in levels of circulating inflammatory markers after percutaneous coronary revascularization. Circulation 2000 ; 104 : 163 - 7
43. Schwarz M, Nordt T, Bode C, Peter K. The GP IIb/IIIa inhibitor abciximab(c7E3) inhibits the binding of various ligands to the leukocyte integrin Mac-1(CD11b/CD18, alpha(M)beta(2)).
Thromb Res 2002 ; 107 : 121 - 8
44. Kim W, Jeong MH, Hong YJ, Lee SH, Park WS, Kang JC, et al. The long-term clinical results of a platelet glycoprotein
IIb/IIIa receptor blocker(Abciximab : ReoProⓇ) coated stent in patients with coronary artery disease. Korean J Med 2003 ; 65 : 652 - 64
45. Hong YJ, Jeong MH, Kim W, Lim SY, Lee SH, Kang JC, et al.
Effect of Abciximab-coated stent on in-stent intimal hyper- plasia in human coronary arteries. Am J Cardiol 2004(in press) 46. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus
intravenous thrombolytic therapy for acute myocardial infarc- tion : a quantitative review of 23 randomised trials. Lancet 2003 ; 361 : 13 - 20
47. The PCAT Collaborators. Primary coronary angioplasty com- pared with intravenous thrombolytic therapy for acute myocar- dial infarction : six-month follow-up and analysis of indivi- dual patient data from randomised trial. Am Heart J 2003 ; 145 : 47 - 57
48. Smith D. Primary angioplasty should be first line treatment for acute myocardial infarction : FOR. BMJ 2004 ; 328 : 1254 - 6 49. Grzybowski M, Clements EA, Parsons L, Welch R, Tintinalli
AT, Zalenski RJ, et al. Mortality benefit of immediate revascu- larization of acute ST-segment elevation myocardial infarc- tion in patients with contraindications to thrombolytic therapy.
JAMA 2003 ; 290 : 1891 - 8
50. Stone GW, Grines CL, Cox DA, Garcia E, Tcheng JE, Lansky AJ, et al. for the Controlled Abciximab and Device Investi- gation to Lower Late Angioplasty Complications(CADILLAC) Investigators. Comparison of angioplasty with stenting, with or without abciximab, in acute myocardial infarction. N Engl J Med 2002 ; 346 : 957 - 66
51. Wharton TP Jr, Grines LL, Turco MA, Johnston JD, Souther J, Grines CL, et al. Primary angioplasty in acute myocardial infarc- tion at hospitals with no surgery on-site(the PAMI-No SOS study) versus transfer to surgical centers for primary angio- plasty. J Am Coll Cardiol 2004 ; 43 : 1943 - 50
52. Andersen HR, Nielsen TT, Rasmussen K, Thuesen L, Kelbaek H, Mortensen LS, et al. for the DANAMI-2 Investigators. A
comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med 2003 ; 349 : 733 - 42
53. Widimsky P, Budesinsky T, Vorac D, Groch L, Zelizko M, Formanek P, et al. PRAGUE Study Group Investigators. Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction : final results of the randomised national multicentre trial-PRAGUE-2. Eur Heart J 2003 ; 24 : 94 - 104
54. Fernandez-Aviles F, on behalf of the GRACIA Group. Primary optimal percutaneous coronary intervention versus facilitated intervention(tenecteplase plus stenting) in patients with ST-
elevated acute myocardial infarction (GARCIA-2). Presented at the European Society of Cardiology Congress 2003, Vienna, Austria, September 2003
55. Kastrati A, Mehilli J, Schlotterbeck K, Dotzer F, Dirschinger J, Schomig A, et al. Bavarian Reperfusion Alternatives Evalua- tion(BRAVE) Study Investigators. Early administration of re- teplase plus abciximab vs abciximab alone in patients with acute myocardial infarction referred for percutaneous coronary intervention : a randomized controlled trial. JAMA 2004 ; 291 : 947 - 54
56. Ellis SG, Armstrong P, Betriu A, Brodie B, Herrmann H, Topol E, et al. Facilitated Intervention with Enhanced Reperfusion Speed to Stop Events Investigators. Facilitated percutanous coronary intervention versus primary percutaneous coronary intervention : design and rationale of the Facilitated Interven- tion with Enhanced Reperfusion Speed to Stop Events (FINESSE) trial. Am Heart J 2004 ; 147 : E16
57. The GUSTO Angiographic Investigators. The effects of tissue plasminogen activator, streptokinase, or both on coronary ar- tery patency, ventricular function, and survival after acute myo- cardial infarction. N Engl J Med 1993 ; 329 : 1615 - 22 58. Chesebro JH, Knatterud G, Roberts R, Borer J, Cohen LS,
Ludbrook P, et al. Thrombolysis In Myocardial Infarction (TIMI)
Trial, Phase I : A comparison between intravenous tissue plas- minogen activator and intravenous streptokinase : clinical find- ings through hospital discharge. Circulation 1987 ; 76 : 142 - 54
59. McKendall GR, Attubato MJ, Drew TM, Feit F, Sharaf BL, Williams DO, et al. Safety and efficacy of a new regimen of intravenous recombinant tissue-type plasminogen activator potentially suitable for either pre-hospital or in-hospital administration. J Am Coll Cardiol 1991 ; 18 : 1774 - 8 60. Hong YJ, Jeong MH, Lee SH, Park OY, Kim JH, Kang JC, et
al. The long-term clinical outcomes after rescue percuta- neous coronary intervention in patients with acute myocardial infarction. J Interv Cardiol 2003 ; 16 : 209 - 16
61. Tadros GM, Islam MA, Mirza A, Blankenship JC, Iliadis EA.
Angiographic and long-term outcomes of “rescue” stenting versus PTCA in failed thrombolysis in acute myocardial infarc- tion. Angiology 2004 ; 55 : 169 - 76
62. Saia F, Lemos PA, Lee CH, Arampatzis CA, Hoye A, Serruys PW, et al. Sirolimus-eluting stent implantation in ST-eleva- tion acute myocardial infarction. Circulation 2003 ; 108 : 1927 - 9
63. Lemos PA, Saia F, Hofma SH, Daemen J, Ong AT, Serruys PW, et al. Short-and long-term clinical benefit of siroli- mus-eluting stents compared to conventional bare stents for patients with acute myocardial infarction. J Am Coll Cardiol 2004 ; 43 : 704 - 8
64. Kim W, Jeong MH, Kang DG, Lee YS, Kim KH, Kang JC, et al.
The long-term clinical results of a platelet glycoprotein IIb/IIIa receptor blocker(abciximab : ReoPro®)-coated stent in pa- tients with acute myocardial infarction. Kor Circulation J 2004(submitted)
65. Kim W, Jeong MH, Kim KH, Park JC, Lee SH, Kang JC, et al.
The rescue use of a platelet glycoprotein IIb/IIIa receptor blocker(abciximab ; ReoPro®) in high-risk patients with acute myocardial infarction underwent percutaneous coronary inter-
vention. Kor Circulation J 2001 ; 30 : 492 - 9
66. Antoniucci D, Rodriguez A, Hempel A, Valenti R, Migliorini A, Colombo A, et al. A randomised trial comparing primary infarct artery stenting with or without abciximab in acute myocardial infarction. J Am Coll Cardiol 2003 ; 42 : 1879 - 85
67. Antoniucci D, Migliorini A, Parodi G, Valenti R, Rodriguez A, Santoro GM, et al. Abciximab-supported infarct artery stent implantation for acute myocardial infarction and long-term survival : a prospective, multicenter, randomized trial compar- ing infarct artery stenting plus abciximab with stenting alone.
Circulation 2004 ; 109 : 1704 - 6
68. Kandzari DE, Tcheng JE, Cohen DJ, Bakhai A, Grines CL,
Stone GW, et al. CADILLAC Investigators. Benefits and risks of abciximab use in primary angioplasty for acute myocardial infarction : the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications(CADILLAC) trial.
Circulation 2003 ; 108 : 1316 - 23
69. Waters RE, Singh KP, Roe MT, Lotfi M, Sketch MH, Mahaffey KW, et al. Rationale and strategies for implementing commu- nity-based transfer protocols for primary percutaneous coro- nary intervention for acute ST-segment elevation myocardial infarction. J Am Coll Cardiol 2004 ; 43 : 2153 - 9
70. Fox KAA. Management of acute coronary syndromes : an update. Heart 2004 ; 90 : 698 - 706