Systemic lupus erythematosus (SLE) patients frequent- ly present with neuropsychiatric symptoms that vary from overt neurological and psychiatric disorders to more subtle signs, such as headache, mood disorders, and defects in cognitive function. Neurological and psy-
chiatric illness occur in 25-70% of SLE patients and are responsible for significant morbidity and mortality (1).
Primary central nervous system (CNS) involvement (CNS lupus) results from a combination of factors relat- ed to an autoimmune response including vasculopathy, coagulopathy from the presence of antiphospholipid an- tibodies, and vasculitis. Five categories of mechanisms that underlie CNS manifestations in SLE are ischemia, hemorrhage, white matter damage, neuronal dysfunc- tion and deficient psychological reactions (2). MR imag- ing findings of neuropsychiatric SLE are highly variable.
Moritani et al. described that diffusion-weighted imag-
MR Manifestations of the Brain in Neuropsychiatric Systemic Lupus Erythematosus Patients
1Kyu Chan Oh, M.D., Woo Mok Byun, M.D., Han Won Jang, M.D., Kum Rae Kim, M.D.
1Department of Diagnostic Radiology, College of Medicine, Yeungnam University, Korea
Received September 18, 2007 ; Accepted November 15, 2007
Address reprint requests to : Woo Mok Byun, M.D., Department of Diagnostic Radiology, College of Medicine, Yeungnam University, 317-1, Daemyungdong, Namku, Daegu 705-717, Korea.
Tel. 82-53-620-3046 Fax. 82-53-653-5484 E-mail: [email protected]
Purpose: The primary goal of this study was to evaluate the MR findings of systemic lupus erythematosus (SLE) patients with neuropsychiatric symptoms.
Materials and Methods: The MR images of 38 patients with SLE were evaluated based on the presence of the following abnormal lesions: the locations of the abnormal signal intensity lesions in the white matter, infarctions, a small vessel vasculopathy, leukoen- cephalopathy, hemorrhage, abscess, and other lesions.
Results: The MR images showed an abnormality in 22 of 38 (58%) episodes. Abnormal signal intensities were noted in the subcortical and periventricular white matter in six cases, acute territorial infarctions in five cases, multiple small acute embolic infarc- tions in four cases and a brain abscess in two cases. A reversible posterior leukoen- cephalopathy was found in one case. In addition, another patient had vasogenic edema with focal central cytotoxic edema at the pons. The entire cerebral and corpus callo- sum volumes were significantly smaller in four patients with SLE as compared to the volumes in healthy control subjects.
Conclusion: SLE may induce variable MR imaging findings of the CNS. Recognition of the variable findings is helpful for easy diagnosis and prompt treatment.
Index words :Brain diseases
Lupus erythematosus, systemic Central nervous system
Magnetic resonance (MR)
ing shows primarily two patterns of acute or subacute parenchymal lesions in patients with SLE: acute or suba- cute infarction and vasogenic edema with or without microinfarcts (3). In 69% of cases, MRI demonstrated in- volvement of the CNS both in asymptomatic patients (64.3%) and in patients with neuropsychiatric manifes- tations (73.3%), including microembolic signals, cere- bral infarctions (associated with antiphospholipid syn- drome), atrophy, basal ganglia involvement, posterior leukoencephalopathy, subcortical calcification or hemo- siderin deposits (T2*) and dilated perivascular spaces (4). Cerebral small vessel angiopathy is the predominant histopathological abnormality associated with SLE. On MRI, T2-weighted images of the brain reveal small punctuate lesions of increased signal intensity that are localized mainly in the periventricular and subcortical white matter in many SLE patients (2). As CNS changes resulting from hypertension or the aging process may reveal periventricular and subcortical lesions, the most common cerebral MR imaging findings due to small ves- sel angiopathy in SLE are not specific.
It is necessary to characterize and to evaluate the vari- able and unusual CNS manifestations of SLE on MR im- ages to understand the pathogenic mechanisms and treatment. The aim of this study was to evaluate the CNS MR imaging findings of SLE.
Materials and Methods
A total of 38 patients that had SLE with neuropsychi- atric symptoms were evaluated by the use of intracra- nial MRI. All patients fulfilled the American College of Rheumatology criteria for SLE (5, 6). The patients in- cluded 27 women and 11 men, ages 11 to 81 years (mean age, 46 years). The symptoms of the patients are described in Table 1. MR examinations were performed using 1.5T (Vision; Siemens, Eralngen, Germany) im- agers. Axial T1-weighted images (400-600/25-30 [TR/TE] were obtained before and after the administra- tion of gadopentetate dimeglumine (Magnevist;
Schering, Berlin, Germany; 0.1 mmol/kg of body weight). Axial T2-weighted images (2000-2500/100-120 [TR/TE]) or turbo-T2-weighteed images (3000-4000/90- 100 [TR/TE]) were obtained before administration of gadopentetate dimeglumine. Fluid-attenuated inversion- recovery (FLAIR) images (10,000/140 [TR/TE]) were ac- quired. The section sickness was 3 mm, with an inter- section spacing of 0%. A matrix size of 256×256 with a 20- to 24-cm field of view was used. The number of sig-
nal acquisitions was two. Axial diffusion-weighted im- ages (4000-5000/70-80 [TR/TE]) were obtained with single-shot, spin-echo-type echo-planar imaging (field of view, 210×210 mm; image matrix, 256×256; section thickness, 5.0 mm with 3.0 mm gaps). The diffusion gra- dient strength was 66 mT/m. MR angiography (TOF- MRA: 16.8/6.9 [TR/TE], Contrast enhanced carotid MRA: 4.2/1.6 [TR/TE]) was performed in fourteen cases.
MR images were evaluated based on the presence or absence of abnormal lesions: locations of the abnormal signal intensity lesions in the white matter, territorial in- farctions, small vessel vasculopathy, leukoencephalopa- thy, hemorrhage, abscess and other lesions. Apparent diffusion coefficient (ADC) and signal intensity changes on ADC and diffusion-weighted images were evaluated.
We compared patients with SLE and control subjects in the same age range and sex for evaluation of brain atro- phy, using examination of the images with visual in- spection. Control subjects for comparison were selected in cases without apparent cranial symptoms, such as a routine MR examination for a health examination. An examination of antiphospholipid antibody was evaluat- ed in eleven cases. The presence of antiphospholipid an- tibody was compared with the clinical and MR imaging findings. Follow-up MR examinations for the evaluation
Table 1. Clinical Symptoms of Patients with Neuropsychatric SLE
Symptom Number (%)
Headache 18 (47.3%)
Motor weakness 10 (26.3%)
Mental change 05 (13.1%)
Seizure 3 (7.9%)
Neck stiffness 2 (5.2%)
Extremity tingling sensation 2 (5.2%)
Dizziness 1 (2.6%)
Dysarthria 1 (2.6%)
Tremor 1 (2.6%)
Hypothermia 1 (2.6%)
Table 2. MR Imaging Findings of Patients with Neurosychiatric SLE
Finding Number (%)
Normal 16 (42%)
Multiple small white matter lesions 06 (16%) Acute territorial infarctions 05 (13%) Multiple embolic infarctions 04 (11%)
Brain abscess 2 (5%)
Hematoma 1 (3%)
Aneurysm 1 (3%)
Reversible posterior leukoencephalopathy 1 (3%) Diffuse reversible encephalopathy in the pons 1 (3%)
Brain atrophy 04 (11%)
of disease progression or improvement were performed in ten cases.
Results
The MR images showed abnormalities in 22 of 38 (58%) episodes. The MR imaging findings of the patients are described in Table 2. Six patients had multiple punc- tuate lesions in both the cerebral subcortical and periventricular white matter (Fig. 1). Multiple small acute embolic infarctions were seen in four cases, and one case with embolic infarctions developed multiple brain abscesses (Fig. 2). Brain abscesses were found in two cases and were seen with multiple patterns. We supposed that one case with brain abscess developed from a septic embolic infarction. Another patient with an acute embolic infarction showed a combined multifo-
cal small hematoma in both temporal lobes and an aneurysm in the right middle cerebral artery, distal to M2 (Fig. 3). A reversible posterior leukoencephalopathy was found in one case. Both basal ganglia, the thalamus- es, the occipital cortex, brainstem and left cerebellum showed iso signal intensity on a diffusion-weighted im- age and high signal intensity on an ADC image repre- senting reversibility (Fig. 4). Vagogenic edema was caused by sudden hypertensive crisis. After treatment of hypertension, there was marked improvement of the le- sions as seen on follow-up MR images after twelve days.
In one patient, the pons on a diffusion-weighted image showed iso- or slightly hyperintense lesions and an ap- parent diffusion coefficient (ADC) image revealed an in- creased ADC, suggesting vasogenic edema and focal central cytotoxic edema (Fig. 5). The diffuse reversible leukoencephalopathy in the pons improved in one
A B C
Fig. 2. A 65-year-old female patient with acute multifocal embolic infarctions in both centrum semiovales.
Multifocal high signal intensities (arrows) at both centrum semiovales are seen on a diffusion weighted image (A). Follow-up con- trast enhanced T1-weighted images after 4 months reveal rim-enhancing lesions at the cerebellar vermis and left fronto-parietal lobe representing an abscess (B, C).
A B
Fig. 1. A 28-year-old male patient with multiple punctuate lesions represent- ing small vessel vasculopathy.
An initial axial FLAIR image (A) shows multifocal punctate lesions (arrows) at both the cerebral subcortical and left periventricular white matter. A fol- low-up axial FLAIR image (B) after four months showed a decrease of the size and number of lesions
month as seen on a follow-up MR examination. Both of the entire cerebral and entire corpus callosum volumes were significantly smaller in four patients with SLE as compared with the volumes in healthy control subjects.
In general, symptoms of brain atrophy include cognitive impairment, mental change, and seizure, but the above four patients did not have the above symptoms.
Antiphospholipid antibody was positive in five of the eleven cases (45%). The MR imaging findings of the pa- tients with a positive antiphospholipid antibody were multiple punctate lesions in the cerebral subcortical and periventicular white matter representing small vessel vasculopathy (n = 2), multiple acute embolic infarctions (n = 2) and a normal brain (n = 1). There was no corre-
lation between a positive antiphospholipid antibody and clinical symptoms. A follow-up MR study was per- formed for patients with acute territorial infarction (n = 3), reversible posterior leukoencephalopathy (n = 1), diffuse reversible leukoencephalopathy in the pons (n = 1), acute embolic infarction (n = 2), multiple punctuate subcortical and periventricular white matter lesions (n
= 1) and a normal brain (n = 2). A decrease of the size and number of the multiple punctate subcortical and periventricular white matter lesions were seen on a fol- low-up MR study after four months.. Five of fourteen cases showed occlusion or stenosis of the extracranial internal carotid and intracerebral arteries.
A B C
Fig. 4. A 42-year-old female patient with reversible posterior leukoencephalopathy.
Both basal ganglia, both thalamuses and the brainstem show iso signal intensity on a diffusion-weighted image (A) and high signal intensity on an ADC image (B) representing vasogenic edema. There are no more abnormal signal intensities seen on a follow-up T2 weighted image (C) after 12 days. Figures of the occipital cortex and left cerebellar lesions are not shown.
A B C
Fig. 3. A 26-year-old female patient with hematomas and an aneurysm.
Acute and subacute hematomas at both temporal lobes are demonstrated on T1-weighted images (A, B). Right internal carotid an- giography shows a 9.8×5.3 mm sized saccular aneurysm in the distal M2 segment of the right middle cerebral artery (C).
Discussion
Systemic lupus erythematosus (SLE) is a prototypical multisystem disease with multiple autoantibodies in- volvement, and is a chronic, inflammatory, autoim- mune disease of unknown etiology primarily affecting females of childbearing age. Between 30% and 70% of SLE patients have significant neuropsychiatric distur- bances during the course of the disease (7). The signs and symptoms of neuropsychiatric-SLE span a wide spectrum, ranging from overt findings such as seizure, stroke, psychosis, transverse myelitis, and aseptic meningitis to more subtle abnormalities of memory, concentration, intellect, and mood (8).
Abreu et al. reported that the most frequent brain imaging findings were more prevalent in neuropsychi- atric SLE; the most frequent finding in all MR examina- tions was focal high signal intensity in the periventricu-
lar white matter, as seen on T2-weighted and FLAIR im- ages (9). Histopathological findings suggest that these ab- normalities are caused by microinfarcts, hemorrhage, is- chemic demyelination, multiple-sclerosis-like demyeli- nation, and bland vasculopathy. The vessels affected are predominantly arterioles and capillaries (10). Jennings et al. reported on the frequency and pattern of signal ab- normalities seen on conventional MRI in patients with suspected neuropsychiatric systemic lupus erythemato- sus; MRI was normal or nearly normal in 34% of cases.
In 60% of cases, multifocal small high-signal lesions were observed on T2-weighted images, and were fre- quently observed in the frontal and parietal subcortical white matter (11). In our study, intracranial MR images were normal in 16 of 38 cases (42%), and periventricular and subcortical mulifocal lesions were seen in five cas- es. Periventricular lesions detected on MRI can be im- possible to differentiate from multiple sclerosis. White matter punctuate hyperintensities increase with age in
A B
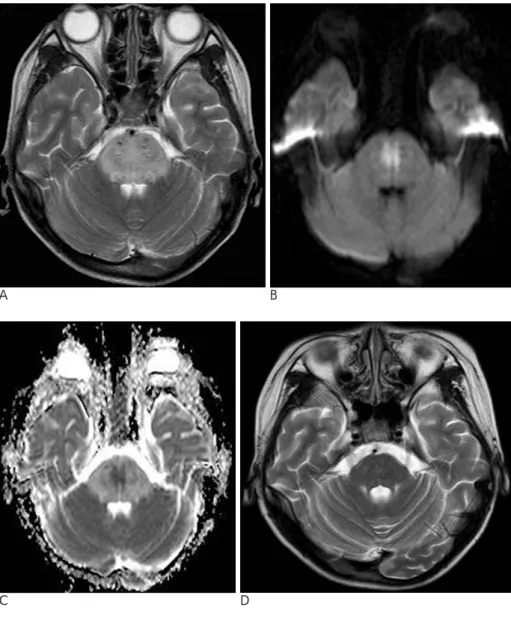
Fig. 5. An 11-year-old male patient with diffuse reversible leukoen- cephalopathy in the pons.
A T2-weighted image (A) shows dif- fuse high signal intensity with swelling at the pons. Iso signal intensi- ty with focal central high signal inten- sity on a diffusion-weighted image (B) is noted. The ADC image (C) reveals increased intensity with a central focal decreased ADC representing vaso- genic edema with central focal cy- totoxic edema. There is no more ab- normal signal intensity except for sub- tle central gliosis seen on a follow-up T2-weighted image (D) after one month.
C D
the general population and are also associated with hy- pertension, and it is not possible to differentiate be- tween SLE from other vasculopathies using convention- al MRI (12). Therefore, the different frequencies of white matter focal lesions of SLE may be caused by the inclusion of other vasculopathy-induced nonspecific findings.
Dahl et al. reported that microembolic signals on tran- scranial Doppler ultrasonography of 55 patients were detected in five cases (9%) and cerebral infarcts were found in nine cases (18%). These investigators reported that an embolism may be an important pathogenic fac- tor for cerebral infarcts and cognitive dysfunction in pa- tients with SLE (13). Multiple small embolic infarctions on diffusion-weighted images were seen in four cases (13%) in our study. The sources of multiple acute em- bolic infarctions were not determined. An autopsy of a 57-year-old woman with systemic lupus erythematosus (SLE) documented the presence of multiple brain in- farcts and cerebral arterial emboli that originated from the verrucae of Libman-Sacks endocarditis (14).
Magnano et al. described five cases of reversible pos- terior leukoencephalopathy in patients with SLE.
Reversible posterior leukoencephalopathy is preceded by hypertension, renal insufficiency, and recent expo- sure to high doses of immunosuppressant medication (15). A patient with reversible posterior leukoen- cephalopathy due to hypertension was found in our study. Both basal ganglia, both thalamuses, the occipital cortex, brainstem and left cerebellum showed iso signal intensity on diffusion-weighted images and high signal intensity on an ADC image representing vagogenic ede- ma. After treatment of hypertension, there was marked improvement of the lesions on follow-up MR images af- ter a period of 12 days.
A brain abscess in SLE is rare. SLE patients with Libman-Sacks endocarditis have mitral and aortic valve abnormalities that can lead to a septic cerebral em- bolism (16). In one patient with multiple acute embolic infarctions in both centrum semiovales, abscesses in the right centrum semiovale and cerebellum developed af- ter four months. The cause of multiple brain abscesses was not determined, but we supposed that a brain ab- scess developed from a septic embolic infarction.
Cerebral aneurysms associated with SLE are uncom- mon. There have been a few reported cases of peripher- ally located aneurysms associated with SLE (17-23).
The mechanism of unusual aneurysmal formation in SLE is thought to be due to transmural angiitis or fibri-
noid necrosis producing local weakness in the walls of the small vessels (20). A 26-year-old female presented with an aneurysm in right middle cerebral artery (M2 segment). A follow-up study and treatment for aneurysm were not performed.
Cerebral atrophy has been described to occur in SLE with variable frequency, but its exact cause remains un- clear. Appenzeller et al. reported that in an MRI analy- sis, cerebral atrophy was found in 8.7% of patients with SLE. Reduced cerebral and corpus callosum volumes were related to the disease duration (24). We evaluated brain atrophy by a visual inspection method for a com- parison with a normal control group of subjects that may represent a limitation of our study.
Moritani et al. reported that in four of nine patients with SLE lesions, diffusion-weighted imaging primarily showed hyperintense lesions with a decreased ADC, which indicates acute or subacute infarcts. In four other patients, diffusion-weighted imaging primarily showed iso- or slightly hyperintense lesions with an increased ADC, suggesting vasogenic edema (3). In one patient (an 11-year-old male), diffusion-weighted images showed mild hyperintensity with a slightly increased ADC in the entire pons, which presumably represents vasogenic edema. A very hyperintense spot with ADC reduction was also seen within the lesion, indicating the presence of a microinfarct. In five cases, diffusion-weighted im- ages showed hyperintense lesions with a decreased ADC, which indicates the presence of acute infarcts.
In conclusion, SLE may show variable MR imaging findings of the CNS. It is necessary to recognize the vari- able and unusual MR manifestations of the brain in neu- ropsychiatric systemic lupus erythematosus patients to understand the pathogenesis of the disorder and to pro- vide accurate diagnosis and treatment.
References
1. Cikes N. Central nervous system involvement in systemic connec- tive tissue diseases. Clin Neurol Neurosurg 2006;108:311-317 2. Jennekens FG, Kater L. The central nervous system in systemic lu-
pus erythematosus. Part 2. Pathogenetic mechanisms of clinical syndromes: a literature investigation. Rheumatology 2002;41:619- 630
3. Moritani T, Shrier DA, Numaguchi Y, Takahashi C, Yano T, Nakai K, et al. Diffusion-weighted echo-planar MR imaging of CNS in- volvement in systemic lupus erythematosus. Acad Radiol 2001;8:741-753
4. Cotton F, Bouffard-Vercelli J, Hermier M, Hermier M, Tebib J, Vital Durand D, et al. MRI of central nervous system in a series of 58 systemic lupus erythematosus (SLE) patients with or without overt neuropsychiatric manifestations. Rev Med Interne 2004;25:8-
15
5. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, et al. The 1982 revised criteria for the classification of systemic lu- pus erythematosus. Arthritis Rheum 1982;25:1271-1277
6. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythemato- sus. Arthritis Rheum 1997;40:1725
7. West SG. Neuropsychiatric lupus. Rheum Dis Cli North Am 1994;20:129-158
8. Carbotte RM, Denburg SD, Denburg JA. Cognitive deficit associat- ed with rheumatic diseases: neuropsychological perspectives.
Arthritis Rheum 1995;38:1363-1374
9. Abreu MR, Jakosky A, Folgerini M, Brenol JC, Xavier RM, Kapczinsky F. Neuropsychiatric systemic lupus erythematosus:
correlation of brain MR imaging, CT, and SPECT. Clin Imaging 2005;29:215-221
10. Hess DC. Cerebral lupus vasculopathy. Mechanisms and clinical relevance. Ann N Y Acad Sci 1997;823:154-168
11. Jennings JE, Sundgren PC, Attwood J, McCune J, Maly P. Value of MRI of the brain in patients with systemic lupus erythematosus and neurologic disturbance. Neuroradiology 2004;46:15-21 12. Peterson PL, Axford JS, Isenberg D. Imaging in CNS lupus. Best
Pract Res Clin Rheumatol 2005;19:727-739
13. Dahl A, Omdal R, Waterloo K, Joakimsen O, Jacobsen EA, Koldingsnes W, et al. Detection of cerebral embolic signals in pa- tients with systemic lupus erythematosus. J Neurol Neurosurg Psychiatry 2006;77:774-779
14. Fox IS, Spence AM, Wheelis RF, Healey LA. Cerebral embolism in Libman-Sacks endocarditis. Neurology 1980;30:487-491
15. Magnano MD, Bush TM, Herrera I, Altman RD. Reversible poste-
rior leukoencephalopathy in patients with systemic lupus erythe- matosus. Semin Arthritis Rheum 2006;35:396-402
16. Lalani TA, Kanne JP, Hatfield GA, Chen P. Imaging findings in systemic lupus erythematosus. Radiographics 2004;24:1069-1086 17. Kawamata T, Kagawa M, Kubo O, Takeshita M, Ujiie H, Sato K, et
al. Clinicopathological studies of three cases of cerebral aneurysms associated with systemic lupus erythematosus. No Shinkei Geka 1991;19:633-639
18. Kodama S, Asakura T, Kadota K, Kasamo S. A case of systemic lu- pus erythematosus with subarachnoid hemorrhage due to rup- tured aneurysm. No Shinkei Geka 1990;18:571-575
19. Asai A, Matsutani M, Kohno T, Fujimaki T, Takakura K. Multiple saccular cerebral aneurysms associated with systemic lupus ery- thematosus—case report. Neurol Med Chir 1989;29:245-247 20. Nakai Y, Hyodo A, Yanaka K, Akutsu H, Nose T. Distal superior
cerebellar artery aneurysm in a patient with systemic lupus ery- thematosus: case report. Surg Neurol 2000;54:73-76
21. Mimori A, Suzuki T, Hashimoto M, Nara H, Yoshio T, Masuyama JI, et al. Subarachnoid hemorrhage and systemic lupus erythe- matosus. Lupus 2000;9:521-526
22. Orita T, Kajiwara K, Izumihara A. Ruptured aneurysm at the pe- ripheral branch of the posterior cerebral artery with systemic lu- pus erythematosus. No To Shinkei 1992;44:733-737
23. Nagayasu S, Hanakita J, Miyake H, Suzuki T, Nishi S. A case of systemic lupus erythematosus associated with multiple intracra- nial aneurysms. No Shinkei Geka 1986;14:1251-1255
24. Appenzeller S, Rondina JM, Li LM, Costallat LT, Cendes F.
Cerebral and corpus callosum atrophy in systemic lupus erythe- matosus. Arthritis Rheum 2005;52:2783-2789
대한영상의학회지 2008;58:1-7
신경정신의학적 전신성홍반성루프스 환자의 뇌 자기공명영상소견
11영남대학교 의과대학 영상의학과학교실
오규찬・변우목・장한원・김금래
목적: 이 연구의 목적은 신경정신의학적 증상이 있는 전신성홍반성루프스 환자들에게서 나타나는 자기공명영상 소 견에 대해 알아보고자 한다.
대상과 방법: 전신성홍반성루프스가 있는 38명의 환자에게 두개 내 자기공명영상을 이용하여 비정상 병변의 존재 를 평가하였다: 백질 내 비정상적인 신호강도의 위치, 뇌경색, 소혈관질환, 백질뇌병증, 출혈, 농양, 그리고 다른 비 정상 병변.
결과: 38예 중 22예(58%) 에서 비정상적인 자기공명영상 소견을 보였다. 피질하와 뇌실 주위 백질에 비정상 신호 강도를 보인 6예, 급성 구역성 뇌경색을 보인 5예, 작은 급성 다발성 색전성 뇌경색을 보인 4예, 뇌농양을 보인 2 예, 가역성 후방 백질뇌병증을 보인 1예, 그리고 교뇌에 혈관성부종과 국소성 중심 세포독성부종을 보인 1예도 있 었다. 건강한 대조 군과 비교하여 4예 에서는 대뇌와 뇌량의 의미 있는 용적의 감소가 관찰되었다.
결론: 전신성홍반성루프스는 중추신경계에서 다양한 자기공명영상 소견을 보일 수 있다. 이러한 다양한 영상소견을 인지함으로 인해 보다 쉬운 진단과 즉각적 치료에 도움을 줄 수가 있다.