Introduction
Children with cerebral palsy (CP) disturbs mobility because it induces low postural control, decreased coordination of movement, and spasticity of the legs.
Impaired balance control in CP limits individuals in independent standing or walking (Bleck, 1994), daily functional activities, and social participation. A deficit of trunk stability and lower limb mobility associated various compensation movements while children with CP move. The compensation movements result from greater sway to balance control in body segments (Bennett, 1987).
Balance is definitely a skill necessary to maintain the body’s center of gravity relative to the base of support (Corrêa et al, 2006). Maintaining balance during static or dynamic activities demands complex
mechanism among cognitive, motor, vestibular, cer- ebellar, and proprioceptive systems (Du Pasquier et al, 2003). In children with CP, these mechanisms are known to be affected. Unilateral CP has revealed higher values of postural sway during stance, asym- metric pressure distribution with greater weight on the unaffected leg, and decreased ability to maintain stable posture (Pavão et al, 2013). This asymmetric distribution of weight bearing may lead to muscle atrophy, weakness on the affected side, and reduced balance (Gracies, 2005; Murphy and Such-Neibar, 2003). For a better symmetric alignment and balance recovery, it is important to transfer weight to both lower limbs and maintain independent standing (Newell et al, 1997). Also, children with CP have changed balance control mechanism because of com- pensatory movement due to deficit in ankle joint Corresponding author: Chung-hwi Yi [email protected]
Immediate Effect of Fabric Ankle Foot Orthosis on Balance in Children With Unilateral Cerebral Palsy
Yon-ju Sim1,3, MSc, PT, You-jin Yang2,3, MSc, PT, Chung-hwi Yi4,5, PhD, PT
1Dept. of Physical Therapy, The Graduate School, Yonsei University
2Dept. of Physical Therapy, The Graduate School, Sahmyook University
3Dept. of Rehabilitation Medicine, Wonju Medical Center
4Dept. of Physical Therapy, College of Health Science, Yonsei University
5Dept. of Ergonomic Therapy, The Graduate School of Health and Environment, Yonsei University
Abstract
1)Balance control deficits have been indicated to be a primary problem among cerebral palsy (CP) patients. Fabric ankle foot orthosis (AFO) can allow more efficient balance control by facilitating proprioception. The purpose of this study was to investigate the immediate effect of fabric AFO on balance, compared to a barefoot condition in children with unilateral CP. Twelve children with unilateral CP participated in this study. Their balance ability was evaluated using pediatric balance scale and bubble test. Both pediatric balance scale and bubble test showed significant improvement with the use of the fabirc AFO (p<.05). The fabric AFO could improve functional balance ability, and promote better balance among children with unilateral CP. We demonstrated that fabric AFO contributed to improving balance among children with unilateral CP, classified as Gross Motor Function Classification System level
Ⅰ and Ⅱ. Consequently, fabric AFO might be an assistive device leading to the improvement of balance instead of the typical AFOs.
Key Words: Ankle-foot orthosis; Balance; Cerebral palsy; Foot drop.
control (Ferdjallah et al, 2002).
Ankle-foot orthosis (AFO) is prescribed to im- prove ankle joint stability, pressure distribution, and neuromuscular abnormalities, stability for standing, and walking in children with such condition (Ramstrand and Ramstrand, 2010). However, there have been limitations in AFOs for children with CP.
AFOs are designed to limit inappropriate ankle joint movement in one or more planes (Morris, 2002). In certain situations, it is possible that AFO may cause ankle instability, negatively affect balance, and mus- cle weakness (Ramstrand and Ramstrand, 2010).
Restrictions to joint motion, sensory input, and mus- cle strength can affect balance maintenance limits (Ramstrand and Ramstrand, 2010). Balance ability occurs when proprioception in the plantar region are activated. AFOs are used to improve function and prevent deformities, but they have negative effects, such as restriction of function, expensive cost, and visual unattractiveness (Christovão et al, 2015). In fact, children with CP rarely wear AFO all day long.
The device may be durable and stable, but it allows insufficient mobility. School-aged children’s activities also make them susceptible to injury (Christovão et al, 2015).
Fabric AFO is designed to be more flexible and less restrictive. The sole of the feet is provided min- imal support and stability by the straps while the heel-opened design increases sensory inputs during ground contact. Moreover, fabric AFO is approx- imately 90% less expensive than AFOs and have
lighter materials. This study was to investigate the effects of fabric AFO on balance among children with unilateral CP.
Methods
Subjects
Twelve children with unilateral CP were recruited from a local hospital and pediatric rehabilitation cen- ters in Wonju City, Republic of Korea. The inclusion criteria were a diagnosis of unilateral CP, aged be- tween 7 and 16 years, Modified Ashworth Scale level 1∼2, and able to understand the test instructions.
Gross Motor Function Classification System levelⅠ or Ⅱ were included in this study. The exclusion cri- teria were cognitive or visual disorder, severe ankle deformities, botulinum toxin injections, and orthopedic surgery performed in the last one year. The demo- graphic characteristics of the children are summar- ized in Table 1. Ethical approval for this study was granted by Yonsei University Wonju Institutional Review Board. Their parents constructed informed consent form.
Fabric ankle foot orthosis
The fabric AFO (AIDER drop foot brace, AIDER Inc., Seongnam, Republic of Korea) offers elasticity and breathable effect, which is made up of scratch-resistant Velcro, air-prene, and span-mesh.
The fabric AFO consists of an ankle band with an arch strap and a toe strap. The tension of the ankle band provides stability in the ankle, the arch strap assists in mediolateral support, and a toe strap pre- vents foot drop. The ankle band is put on the ankle, the arch strap goes across the top of the medial mal- leolus and then fastened with Velcro. A toe strap is attached on the medial side of the big toe and this strap goes across the ankle band, a strap on the little toe side is attached on the medial side of ankle band and then fastened with Velcro (Figure 1). The fabric AFO is lighter, more portable, and more comfortable
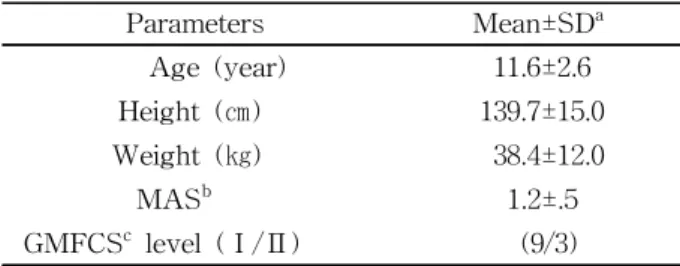
Parameters Mean±SDa
Age (year) 11.6±2.6
Height (㎝) 139.7±15.0
Weight (㎏) 38.4±12.0
MASb 1.2±.5
GMFCSc level (Ⅰ/Ⅱ) (9/3)
amean±standard deviation, bmodified Ashworth scale,
cgross motor function classification system.
Table 1. General characteristics of the subjects (N=12)
than typical AFOs. The benefits of the fabric AFO are that its heel-opened design allows to stimulate pro- prioception and induces flexible movement of the ankle.
Pediatric balance scale (PBS)
Pediatric Balance Scale (PBS) is modified from the Berg Balance Scale. The PBS was developed to de- termine a functional balance ability for the school- age children with motor impairments. The PBS con- tains 14 items including sitting/standing balance, transfers, sitting/standing unsupported, standing with eye closed/with feet together, stepping, standing with one leg in front, one leg standing, retrieving object from the floor, placing alternate foot on the foot- board, and reaching forward. According to the degree of performance or performance time, score is graded on a scale of 0 (no completion) to 4 (completion without difficulty) point. The PBS has been demon-
strated to have good test-retest and inter-rater reli- ability when used with school-age children with mild to moderate motor impairments [intraclass correlation coefficient (ICC=.99)] (Franjoine et al, 2003; Jantakat et al, 2015).
Bubble test
The Wii Fit balance system (Wii, Nintendo, Kyoto, Japan) is a useful measurement tool for balance abil- ity, which has implemented an inexpensive scien- tific-grade force plate and does not demand speci- alized equipment (Clark et al, 2010; D’Addio et al, 2014; Goble et al, 2014). The popularity for use of Wii Fit balance system in balance training and test has been on the rise in clinical setting (Bateni, 2012;
Goble et al, 2014; Jelsma et al, 2013). It contains force sensor to assess force distribution and the re- sultant pathways in the center of pressure. It meas-
A B
C D
Figure 1. Procedures of wearing the fabrc ankle-foot orthosis (A→B→C→D).
ures one’s body sway through the recording (30∼50
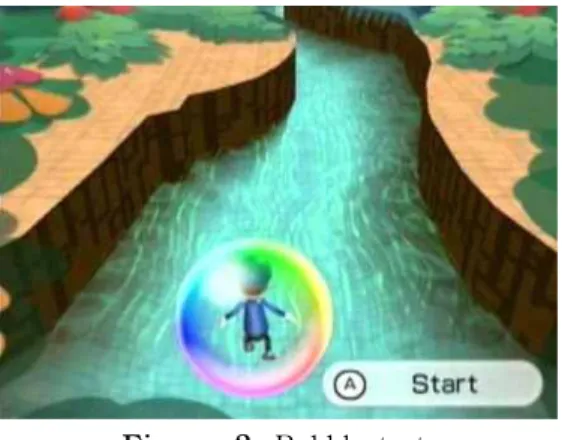
㎐ sampling frequency) from front to back and side to side directions on the Wii Fit balance board (Goble et al, 2014). Bubble test is an example of the Wii Fit balance system. In a bubble test, the im- agery person is encased in a large bubble and is es- tablished to shift his/her weight to move down along the river without touching the river’s edge, causing the bubble to burst. Bubble test requires to ex- quisitely controlled mobility of the center of body mass within the time limit (Figure 2). The more stable the weight shift is, the longer distance (in meters) achieved (Bateni, 2012). The Wii Fit balance system had good to excellent test-retest reliability (ICC=.66∼.94) for the center of pressure pathways measurement and concurrent validity with the force plate (Clark et al, 2010).
Experimental procedures
To minimize the learning effect, the children per- formed PBS and bubble test in barefoot condition first, followed by a 5-minute rest (Sim et al, 2014).
After the children wore the fabric AFO on the af- fected side, they walked a few minutes for adapta-
tion and then performed a test. The bubble test was repeatedly performed three times in each session, and then the average value was taken.
Statistical analysis
Statistical analysis was performed using SPSS ver.
21.0 (SPSS Inc., Chicago, IL, USA). One sample Kolmogorov-Smirnov Z-test was used to assess normality of the data distribution. To compare the differences in the mean values for balance with and without the fabric AFO in children with unilateral CP were analyzed using paired t-test. The level of statistical significance level was p<.05.
Results
PBS and bubble test
When children wore with the fabric AFO, sig- nificant differences were observed in the PBS and bubble test (Table 2). In the PBS test for functional balance and bubble test, there was significant im- provement in balance compared with barefoot con- dition (p<.05).
Discussion
This study investigated the effect of the fabric AFO, which is a light, portable, comfortable orthosis, on balance in children with unilateral CP. This study showed that PBS and bubble test increased significantly. This means that balance control improved. Though PBS is not accurate and detailed uses a force plate, it easily measures, involves less Figure 2. Bubble test.
Without fabric AFOa With fabric AFO t p
PBSb (score) 49.25±3.39c 50.83±2.92 -3.506 .005*
Bubble test (m) 315.74±115.84 417.42±187.54 -3.737 .003*
aankle-foot orthosis, bpediatric balance score, cmean±standard deviation, *significant at p<.05.
Table 2. Comparison of PBS and bubble test with and without fabric AFO in children with unilateral cerebral
palsy (N=12)
cost, and reflects functional balance ability in daily living (Berg et al, 1992). Functional balance ability, which is an important aspect for the performance of functional skills, allows a child to perform functional activities, social activities, recreational participation, and physical activities at home and in school for children with CP (Franjoine et al, 2003). With fabric AFO, children with unilateral CP got a score in one leg standing item, standing with one leg in front item, and reaching forward item. In order to perform this task, balance control is required. Children with unilateral CP have performed this task more easily than in barefoot condition. The ankle strap of the fabric AFO supports the ankle joint, thus it is useful for standing balance.
With fabric AFO conditions, the bubble test showed significant improvement, longer distance, and better the balance. Unlike in barefoot condition, the fabric AFO allows the heel to contact the Wii Fit balance board directly and help prevent foot drop, leading to im- provement of balance ability. Heel contact of the af- fected side might maintain ankle stability and selective movement at the ankle joint (Raine et al, 2009). It is considered that the fabric AFO provided weight shift in various directions during the performance of the bubble test. Many studies reported significant improve- ment on balance and gait in stroke with the use of elastic AFO (Daher et al, 2013, Hwang et al, 2012).
These results are similar to the current study.
To improve balance control (postural schema), tac- tile stimuli from sensory input are activated (Hillier et al, 2015). In particular, proprioception is important for maintaining a dynamic stability of joint, and acts to induce the normal movement by providing the po- sition sense of the body and recognition of the pos- ture to the central nervous system (Docherty et al, 2004). Clinically, proprioception is an important ele- ment of assessment and treatment in neurological populations, while deficit of proprioception causes damages of voluntary movement control, protective ability, recovery from unexpected pertubations, bal- ance control, and gait ability (Edwards, 2002). Unlike
typical AFOs, the fabric AFO is a heel-opened de- sign that allows obtaining proprioception and pres- sure during standing (Kim et al, 2013). Therefore, heel-opened fabric AFO can provide greater inter- action of the postural schema message by increasing tactile stimuli to the central nervous system. Also, the fabric AFO is made of light material that is of benefit to the weakened muscles of the lower legs in children with unilateral CP. Fabric AFO could be easily put in socks.
This finding demonstrates that the fabric AFO constitutes an important device for improving func- tional balance ability in children with unilateral CP.
Thus, the fabric AFO should be appropriately applied not only to indoor but also to outdoor environmental demands to improve balance control in children with unilateral CP. This study had several limitations.
First, the results cannot be generalized to all children with CP due to the small number of subjects.
Second, this study had a cross-sectional design, and immediate effect could be determined. Third, we could not compare to typical AFOs. Nevertheless, this study provides meaningful information in using the fabric AFO in children with unilateral CP.
Conclusion
This study compared balance with and without the fabric AFO in children with unilateral CP. The re- sults were that PBS and bubble test increased sig- nificantly when compared to those without the fabric AFO. Based on the findings, wearing the fabric AFO was shown to give better results than barefoot condition. These results demonstrated that the fabric AFO might be used as an assistive device instead of typical AFOs in the clinic or individual. The fabric AFO is a lighter and less expensive alternative than typical AFOs for balance training in children with unilateral CP. A following-up study is required to effectively render balance when children with unilat- eral CP wear the fabric AFO for a long period.
References
Bateni H. Changes in balance in older adults based on use of physical therapy vs the wii fit gam- ing system: A preliminary study. Physiotherapy.
2012;98(3):211-216. http://dx.doi.org/10.1016/j.physio.
2011.02.004
Bennett F. The effectiveness of early intervention for infants at increased biologic risk. The effective- ness of early intervention for at-risk and handi- capped children. Orlando, FL, Academic Press Inc., 1987:79-112.
Berg KO, Maki BE, Williams JI, et al. Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil.
1992;73(11):1073-1080.
Bleck EE. I. Cerebral palsy hip deformities: Is there a consensus? Ⅱ. Botulinum toxin a: A clinical experiment. J Pediatr Orthop. 1994;14(3):281-282.
Christovão TC, Pasini H, Grecco LA, et al. Effect of postural insoles on static and functional balance in children with cerebral palsy: A randomized controlled study. Braz J Phys Ther. 2015;19(1):
44-51. http://dx.doi.org/10.1590/bjpt-rbf.2014.0072 Clark RA, Bryant AL, Pua Y, et al. Validity and reli-
ability of the nintendo wii balance board for as- sessment of standing balance. Gait posture. 2010;
31(3):307-310. http://dx.doi.org/10.1016/j.gaitpost.
2009.11.012
Corrêa J, Corrêa F, Franco R, et al. Corpral oscillation during static biped posture in children with cere- bral palsy. Electromyogr Clin Neurophysiol.
2006;47(3):131-136.
D’Addio G, Iuppariello L, Gallo F, et al. Comparison between clinical and instrumental assessing us- ing wii fit system on balance control. Medical Measurements and Applications (MeMeA), 2014 IEEE International Symposium on. 2014:1-5.
Daher N, Lee S, Yang YJ. Effects of elastic band orthosis (aider) on balance and gait in chronic stroke patients. Phys Ther Rehabil Sci. 2013;
2(2):81-86.
Docherty CL, Arnold BL, Zinder SM, et al.
Relationship between two proprioceptive meas- ures and stiffness at the ankle. J Electromyogr Kinesiol. 2004;14(3):317-324.
Du Pasquier RA, Blanc Y, Sinnreich M, et al. The effect of aging on postural stability: A cross sectional and longitudinal study. Neurophysiol Clin. 2003;33(5):213-218.
Edwards S. Neurological Physiotherapy: A problem solving approach. 2nd ed. London, Churchill Livingstone, 2002:16.
Ferdjallah M, Harris GF, Smith P, et al. Analysis of postural control synergies during quiet standing in healthy children and children with cerebral palsy. Clin Biomech. 2002;17(3):203-210.
Franjoine MR, Gunther JS, Taylor MJ. Pediatric bal- ance scale: A modified version of the berg bal- ance scale for the school-age child with mild to moderate motor impairment. Pediatr Phys Ther.
2003;15(2):114-128.
Goble DJ, Cone BL, Fling BW. Using the wii fit as a tool for balance assessment and neuro- rehabilitation: The first half decade of
“wii-search”. J Neuroeng Rehabil. 2014;11:12.
http://dx.doi.org/10.1186/1743-0003-11-12
Gracies JM. Pathophysiology of spastic paresis. I:
Paresis and soft tissue changes. Muscle Nerve.
2005;31(5):535-551.
Hwang YI, An DH, Yoo WG. Effects of the dual AFO on gait parameters in stroke patients.
NeuroRehabilitation. 2012;31(4):387-393. http://dx.
doi.org/10.3233/NRE-2012-00808
Hillier S, Immink M, Thewlis D. Assessing proprio- ception: A systematic review of possibilities.
Neurorehabil Neural Repair. 2015:1545968315573055 Jantakat C, Ramrit S, Emasithi A, et al. Capacity of adolescents with cerebral palsy on paediatric balance scale and berg balance scale. Res Dev Disabil. 2015;36C:72-77. http://dx.doi.org/10.1016/
j.ridd.2014.09.016
Jelsma J, Pronk M, Ferguson G, et al. The effect of the nintendo wii fit on balance control and
gross motor function of children with spastic hemiplegic cerebral palsy. Dev Neurorehabil.
2013;16(1):27-37. http://dx.doi.org/10.3109/17518423.
2012.711781
Kim HJ, Chun MH, Kim HM, et al. Effects on foot external rotation of the modified ankle-foot or- thosis on post-stroke hemiparetic gait. Ann Rehabil Med. 2013;37(4):516-522. http://dx.doi.org/
10.5535/arm.2013.37.4.516
Morris C. A review of the efficacy of lower‐limb orthoses used for cerebral palsy. Dev Med Child Neurol. 2002;44(3):205-211.
Murphy N, Such-Neibar T. Cerebral palsy diagnosis and management: The state of the art. Curr Probl Pediatr Adolesc Health Care. 2003;33 (5):146-169.
Newell K, Slobounov S, Slobounova B, et al.
Short-term non-stationarity and the development of postural control. Gait posture. 1997;6(1):56-62.
Pavão SL, dos Santos AN, Woollacott MH, et al.
Assessment of postural control in children with
cerebral palsy: A review. Res Dev Disabil.
2013;34(5):1367-1375. http://dx.doi.org/10.1016/j.ridd.
2013.01.034
Raine S, Meadows L, Lynch-Ellerington M. Bobath Concept: Theory and clinical practice in neuro- logical rehabilitation. 1st ed. Oxford, Wiley- Blackwell, 2009;123-125.
Ramstrand N, Ramstrand S. AAOP state-of-the-sci- ence evidence report: The effect of ankle-foot orthoses on balance-a systematic review. J Prosthet Orthot. 2010;22(10):4-23.
Sim YJ, Lee DR, Yi CH. Immediate effect of fabric ankle-foot orthosis on spatiotemporal gait pa- rameters in children with spastic cerebral palsy.
Phys Ther Korea. 2014;21(1):29-36. http://dx.doi.
org/10.12674/ptk.2014.21.1.029
This article was received March 21, 2015, was re- viewed March 21, 2015, and was accepted May 1, 2015.