관상동맥 스텐트 재협착 아주대학교 의과대학 순환기내과학교실
14
0
0
전체 글
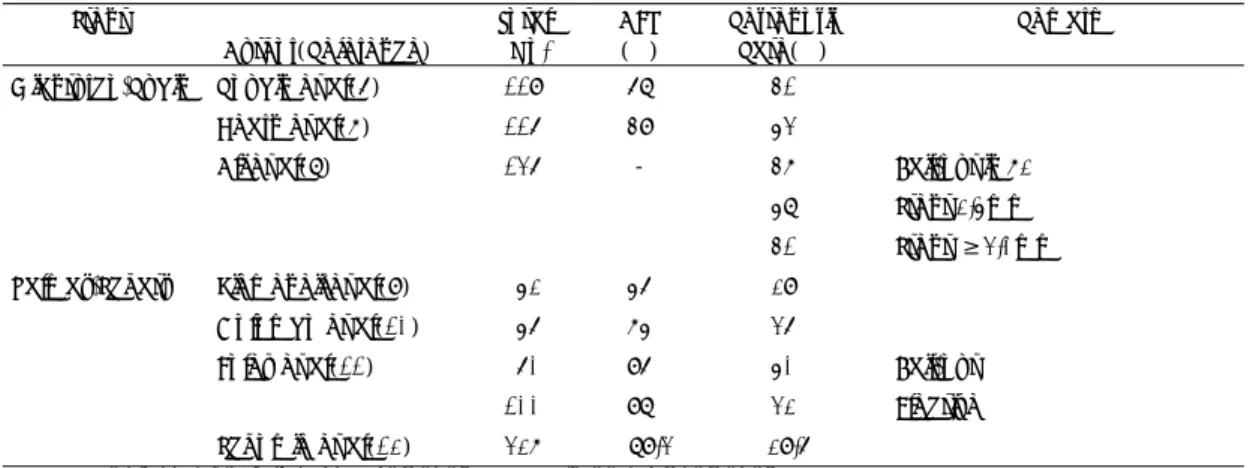
(2) 의 초록들을 검토하여 스텐트재협착의 예방과 치료에 대. (proliferation), 기질화(organization), 재구도(remo-. 한 관심을 모으고 적절한 전략을 생각해 보기로 하였다.. delling) 등이며 각각의 반응은 모두 재협착의 요인으 로 작용할 수 있다.. 스텐트재협착의 빈도. 스텐트 시술이 아닌 다른 관상동맥성형술에서는 혈 관의 병적 재구도(pathological remodeling)에 의한. 관상동맥협착에서 스텐트 시술이 풍선성형술보다 재. 혈관의 만성수축(chronic recoil)과 신생내막증식(ne-. 협착을 유의하게 감소시킨다는 것을 증명한 대표적인. ointimal formation 혹은 hyperplasia)이 재협착의 중. 연구는 BElgium NEtherlands Stent-I(Benestent-. 요한 기전이다33-37). 그러나 스텐트 시술에서는 스텐트. I) trial2)과 STent REStenosis Study-I(STRESS-. 가 혈관의 만성수축을 방지하며, 혈관과 스텐트의 수축. I) 이다. 현재 관상동맥 풍선성형술이 시행되고 있는. 은 재협착의 중요한 기전으로 생각되지 않으며38-42),. 대상병변의 30~40% 정도에 불과하는 제한된 범위에. 신생내막증식에 의한 혈관 내강감소가 가장 중요한 기. 서 시행된 연구이나 6개월 재협착율이 풍선성형술의. 전이다39-42). 신생내막증식은 주로 스텐트 시술시 발생. 32~42% 보다는 낮으나 아직 22~32%에 이르고. 하는 혈전형성43)과 혈관손상44-46)에 의해서 유발된다.. 있었다. 그동안 보고된 스텐트재협착율은 13%4)에서. 스텐트혈전은 불완전한 스텐트확장, 혈관손상, 스텐트의. 3). 61% 까지로 그 차이가 심하나, 각각의 연구가 스텐트. hemocompatibility, 병변부위의 혈류양상, 혈소판과 트. 시술의 적응증, 대상병변, 시술방법 및 항응고치료방. 롬빈 억제 정도 등에 의해서 영향을 받는다. 혈관손상. 법, 스텐트종류등이 다르므로 결과를 직접 비교하기는. 은 많은 인자가 영향을 주겠으나, 혈관의 확장정도(풍. 어렵다. 그동안에 발표된 임상연구들을 스텐트 시술의. 선/혈관 비율), 확장압력, 스텐트 디자인, 스텐트 시술. 적응증, 병변, 스텐트종류에 따라 도표로 정리하여 보았. 전 시행한 혈관성형술의 종류와 결과, 병변의 특성등이. 다(Table 1~6).. 영향을 줄 수 있을 것으로 생각된다. 신생내막은 손상. 5). 후 1주이내에 유의한 증식을 보이기 시작하며 1~2개 월후에는 감소한다44,45). 신생내막의 섬유세포조직(fibr-. 스텐트재협착의 기전. ocellular tissue)은 새로 형성된 증식성 근섬유아세포 관상동맥 성형술후에는 시술시 발생한 혈관손상에. (proliferating myofibroblast)나 혈관외막 근섬유아. 대한 일련의 혈관치유반응(vascular healing respo-. 세포(adventitial myofibroblast)에서 기원한다고 하 며46), 켈로이드(keloid scar)나 평활근종(smooth. nse)이 일어나는데, 혈관수축(vessel recoil), 혈전형성. muscle cell tumor)과 유사한점이 많다. 부검소견에. (thrombosis), 염증반응(inflammmation), 증식반응 Table 1. Restenosis rate of bail-out intracoronary stenting Stent. Total No.. AFU (%). Restenosis Rate(%). 119. 68. 41. Hearn et al(7). 116. 49. 53. Ali et al(8). 136. -. 47. Bail-out in 72%. 58. Stent 2.5mm. 41. Stent ≥3.0mm. Author(Reference) Gianturco-Rubin. Palmaz-Schatz. Roubin et al(6). Kiemeneij et al(9). 52. 56. 29. Colombo et al(10). 56. 75. 36. Foley et al(11) Schomig et al(12). Remark. 60. 96. 50. Bail-out. 100. 98. 32. Elective. 327. 89.3. 29.6. AFU:angiographic follow-up, Restenosis:≥50% in diameter stenosis. - 252 -.
(3) Table 2. Restenosis rate of intracoronary stenting for native coronary lesions Stent. Total. AFU. Restenosis. No.. (%). Rate(%). Serruys et al(2). 262. 93. 22. Serruys et al(4). 202. 98. 13. Author(Reference) Palmaz-Schatz. Remark Benestent-I Elective, de novo Benestent-II Elective, de novo Heparin coated PS. Fischmann et al(3). 207. 85. 31.6. STRESS-I Elective, de novo. Masotti et al(13). 229. -. 22. START. Ellis et al(14). 200. 91. 36. Restenotic in 73%. Schomig et al(15). 164. 38.5. Restenotic. Savage et al(16). 300. 90. 14. De novo. 39. Restenotic. Foleyet al(17). 80. 99. 33. Single stent. van der Giessen et al(18). 70. -. 25.7. WEST under way. Elective, de novo. ACS MultiLink. 32.3. AFU:angiographic follow-up, Restenosis:≥50% in diameter stenosis, Benestent:BElgium NEtherlands Stent, STRESS:STent REStenosis Study, START:STent versus angioplasty restenosis trial, WEST:West european stent trial Table 3. Restenosis rate of intracoronary stenting for chronic total occlusion Stent Author(Reference) Palmaz-Schatz. Mori et al(19). Total. AFU. Restenosis. No.. (%). Rate(%). 43. 100. Remark. 27.9. Goldberg et al(20). 59. 88. 20. Suttorp et al(21). 36. 94. 40. PS stent in 84%. AFU:angiographic follow-up, Restenosis:≥50% in diameter stenosis. Table 4. Restenosis rate of intracoronary stenting for restenotic lesion Stent Author(Reference) Wallstent Palmaz-Schatz Wiktor. Total. AFU. Restenosis. Remark. No.. (%). Rate(%). Eeckhout et al(22). 59. -. 17. Right coronary artery. Colombo et al(23). 128. 89. 25. PS stent in 91%. Savage et al(16). 217. -. 39. 91. -. 30. De Jaegere et al(24). AFU:angiographic follow-up, Restenosis:≥50% in diameter stenosis. 서도 스텐트재협착은 주로 평활근세포의 증식, 혈전 47). 다35,36,38,42,48,49). 스텐트재협착은 Palamz-Schatz 스 텐트에서 가장 많이 연구되었는데, Hoffmann등42)은. 형성, 염증세포침윤이 특징적이었다 . 혈관내 초음파검사는 혈관과 스텐트의 모양과 특성. 스텐트 시술과 관련하여 유발된 신생내막증식이 스텐트. 을 잘 관찰할 수 있어서 스텐트재협착의 양상과 기전. 재협착의 중요한 원인이며 스텐트내 전부위에서 일어. 을 연구하는데 매우 유용한 검사법으로 사용되고 있. 난다고 하였다. Dagawa등48)은 Palamz-Schatz 스텐. - 253 -.
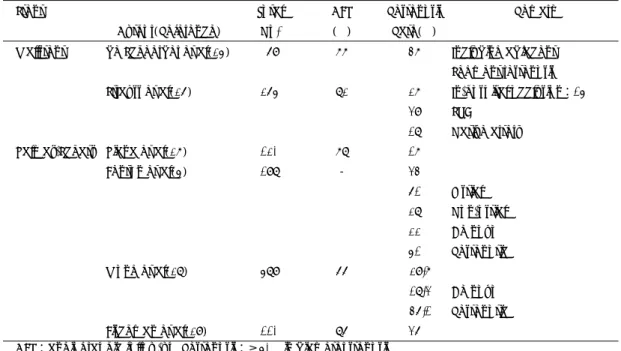
(4) Table 5. Restenosis rate of intracoronary stenting for saphenous vein graft Stent Wallstent. Total. AFU. Restenosis. Author(Reference). No.. (%). Rate(%). Remark. de Scheerder et al(25). 69. 77. 47. 265. 82. 27. In-hospital occlusion:15%. 39. SVG. 18. Native artery. Including adjacent Segment restenosis. Strauss et al(26). Palmaz-Schatz. Piana et al(27). 120. 78. 17. Fenton et al(5). 198. -. 34 61. Wong et al(28). 589. 66. 110. Fischman et al(29). Ostial. 28. Non-ostial. 22. De novo. 51. Restenotic. 29.7. 86. 18.3. De novo. 46.1. Restenotic. 36. AFU:angiographic follow-up, Restenosis:≥50% in diameter stenosis. Table 6. Comparison of restenosis rate of various intracoronary stent Author(Reference). Total. AFU. No.. (%). Palmaz-Schatz. 66. 42. Gianturco-Roubin. 34. 35. Wallstent. 36. 56. 665. 34. Stent Yokoi et al(30). Remark long lesion:length≥20mm. Hssse et al(31). Palmaz-Schatz Palmaz-Schatz AVE Micro. 270. 39. Wiktor. 232. 44. Rau et al(32). restenosis:≥70% in diameter Palmaz-Schatz. 65. 20. AVE Micro. 40. 28. AFU:angiographic follow-up, Restenosis:≥50% in diameter stenosis. 트의 근위경계부(proximal margin)는 조직증식과 혈. Schatz II 스텐트를 이용한 연구53)에서도 스텐트 중간. 관수축, 원위경계부(distal margin)와 관절부(articul-. 부분의 신생내막증식이 가장 심한 것으로 보아 병변. ation)는 주로 혈관수축, 스텐트내부(in-stent)는 조직. 자체가 스텐트 디자인보다 스텐트재협착의 위치와 더. 증식이 재협착의 주된 기전이라고 하였다. 재협착이 가. 욱 많은 관련이 있는 것으로 생각된다.. 장 흔한 곳은 중간부분으로 관절이 있는 독특한 스텐 42,50-52). 트 디자인(design) 때문으로 생각하였으나. 스텐트 시술후 시간경과에 따른 재협착의 진행과정. , Ho-. 은 3개월에 22.0%, 6개월에 31.9%, 12개월에 33.. ffmann등42)의 연구결과 및 관절이 없는 Palmaz-. 2%로 풍선성형술과 유사하여 6개월 이후에는 거의. - 254 -.
(5) 증가히지 않으며, 스텐트 시술후 6개월까지는 혈관내 경이 감소하였으나, 그후에는 17개월까지도 유의한 변화가 없었다고 보고하였다54,55). Asakura등56)은 혈관내시경(angioscope)으로 신생내막의 투명도(intimal transparency)를 관찰해보니 6개월 정도에 신 생내막증식이 절정을 이루고, 그후에는 줄어든다고. Expansion)74)와 STRESS-III75)에서 진행중이다.. 2. 스텐트 재질 및 디자인 스텐트재질에 따른 혈전형성은 stainless steel, tantalum, nitinol등이 모두 큰 차이를 보이지 않는 것으 로 알려져 있다76,77). 그러나, 스텐트 재질과 디자인에 따라 혈관손상과 신생내막증식에 많은 영향을 줄 수. 하였다.. 있는 것으로 알려져 있다78-80). Roger등78)은 토끼 대 퇴동맥에서 stainless steel로 만든 slotted tube type. 스텐트재협착과 관련된 인자. 과 corrugated ring type 스텐트를 비교한 결과 corrugated ring type이 혈관손상, 혈전형성, 및 신. 1. 스텐트 시술 및 병변과 관련된 사항 스텐트재협착에 관여할 수 있는 많은 인자들에 대한 연구는 대부분 시술 및 병변의 특성과 관련된 연구이다. 스텐트, 풍선, 혈관의 크기, 풍선/혈관 비율8,29,49,57-60), 시술후 내강증가정도8,15), 시술후 최소내강직경29,57,61,62), 다수의(multiple) 스텐트14,57,58,61,63,64), 고압력확장 술. 49,58,63). , 병변길이15,57), 석회화65), 시술전 죽상반면. 적66), 동심성병변(concentric lesion)67), 복재정맥이 식편의 궤양성 병변68), 완전폐쇄나 대동맥개구부위 병변(aorto-ostial lesion68), 재협착병변15,16,58,62,69), 당뇨병62)등이 관여하며, 유전인자로 ACE(angiotensin converting enzyme) DD genotype70,71)이 관 여할 가능성도 보고되고 있다. 스텐트의 충분한 확장과 혈전방지를 위하여 고압력 확장술72)이 도입되면서 시술시 혈관손상의 가능성이 더 욱 많아졌을 것으로 생각되는데, Mehran등49)은 스텐트 시술시 풍선/혈관 비율(1.1기준)과 풍선확장압력(16 atm기준)을 이용하여 혈관손상 정도(injury score)를 평가한 결과 혈관손상 정도는 신생내막증식과 내강감 소와 밀접한 관련이 있고 스텐트재협착의 예측인자이 며 작은 혈관에서 혈관손상 정도가 높다고 하였다. Hoffmann등73)은 Palmaz-Schatz 스텐트 경계부위 (margin) 재협착은 경계부위의 조직이 정상이 아닌 경 우 경계부위에서 스텐트에 의한 신내막조직증식이 일 어나 재협착이 잘 오므로 스텐트 시술시 모든 병변을 포함하는 충분한 길이의 스텐트를 사용하여야 하며 스 텐트경계부위의 조직은 정상이어야 한다고 하였다. IVUS-guided 스텐트 시술의 재협착에 대한 영향은 CRUISE(Can Routine Ultrasound Impact Stent. 생내막증식이 적다고 하였다. Squire등79)도 역시 토 끼 대퇴동맥에서 풍선을 서서히 부풀리면서 스텐트확 장을 관찰한 결과, slotted tube type 스텐트에서는 낮은 확장압력(4기압)에서는 스텐트의 양쪽 끝만 아 령모양(dumbell shape)으로 확장되고 기압을 높이 면 가운데가 확장되면서 종축(longitudinal axis)을 따라 수축하며 이때 스텐트 양쪽끝이 혈관을 침투하 거나 긁으면서 손상을 주게되어서, corrugated ring type 스텐트보다 확장이 균일하지 않고, 더 많은 종 축수축, 내막손상, 및 신생내막증식을 일으키며 이것 이 재협착의 원인이 될 수 있다고 하였다. Sheth등80) 은 nitinol과 stainless steel로 만든 slotted tube type 스텐트를 비교한 결과 nitinol스텐트가 혈관손상 과 신생내막증식이 적다고 하였다. Slotted tube type 의 스텐트에서는 이미 기술한 바와 같이 스텐트확장 시 양끝부분이 가장 strain과 stress를 많이 받는 부 분으로 제일 먼저 확장되며 이때 많은 혈관손상을 받 게 되는데, nitinol은 stainless steel과 달리 낮은 압 력에서 아주 쉽게 확장되는 two crystalline phase를 보이는 독특한 stress-strain relation을 가지고 있 어서 slotted tube type에서도 균일한 확장이 가능하 기 때문이라고 하였다. 스텐트 디자인이나 재질간의 비교에 관한 큰 규모 의 무작위 임상연구는 아직 보고된바 없고, 각각의 다 른 연구를 이용하여 차이를 비교하기도 매우 어렵다. Rau등32)은 Palmaz-Schatz 스텐트와 AVE Microstent를, Yokoi등30)은 20mm이상의 긴 병변에서 Palmaz-Schatz 스텐트, Gianturco-Roubin 스텐트,. - 255 -.
(6) Wallstent를 비교하였는데, 두 연구 모두 재협착율. 된다고 보고되었다88-95). Waksman등89)은 방사선요. 에 의의있는 차이는 없었다(Table 6). 현재 ACS. 법을 한 경우 섬유화와 주변조직의 손상이 현저히 감소. MultiLink 스텐트와 Palmaz-Schatz 스텐트(MU-. 하였다고 하였고, 스텐트 시술을 하기전에 방사선요. LTILINK-USA), Gianturco-Roubin II 스텐트와. 법을 한 경우에 신생내막증식 억제효과가 가장 좋다. Palmaz-Schatz 스텐트(GR-II), Wiktor 스텐트와. 고 하였다95). 현재 transcatheter iridium-192를 사. Gianturco-Roubin 스텐트를 비교하는 무작위 연구. 용한 SCRI-PPS trial96,97)과 beta radiation source. 들이 진행중이다81).. 를 이용한 임상연구98)가 진행되고 있다.. 그외에 스텐트내의 혈류속도(flow velocity)와 와. 세포배양과 토끼외장골동맥에서 radioactive wire. 류형성(turbulence)82), 스텐트 디자인에 따른 혈관손. 나 스텐트가 평화근세포나 신생내막의 증식을 억제하는. 상의 정도 및 지속성과 신생내막증식의 정도83), 스. 것이 관찰된 후99,100), 돼지 관상동맥에서 β-particle. 84). 텐트 길이와 혈소판 활성화 에 관한 연구들이 진행되. emitting 스텐트를 이용한 continuous low-dose en-. 고 있다.. dovascular irradiation이 신생내막증식은 억제하며 스텐트의 내피화(endothelialization)는 방해하지 않는. 스텐트재협착의 예방. 다고 보고되었다101,102). 현재로는 β-particle irradiation의 용량과 조직반응의 관계는 확실히 밝혀지. 스텐트재협착의 중요한 원인이 시술후 곧 일어나는 신생내막증식이므로 이를 유발하는 혈전형성과 시술 시의 혈관손상을 최소화하고 진행되는 신생내막증식 을 적극적으로는 억제하는 것이 재협착방지의 기본전 략이 되어야 한다. 이는 어느 한가지 방법만으로 이루 어지기는 어려울 것으로 생각되며 방사선요법, 전신 및 국소 약물요법 및 유전요법, 시술방법, 스텐트 재 질과 디자인의 개선등이 이상적으로 이루어질때 가능 할 것으로 생각된다.. 지 않았고103,104), 장기 효과(long-term effect)도 아 직 미흡하다85,104).. 2. Polymeric Coated Stents Stainless steel 스텐트의 우수한 biocompatibility 가 인정되면서, metal 스텐트의 기계적 장점을 유지하 면서 동시에 혈전형성과 신생내막증식 억제를 위한 local drug delivery가 가능한 polymeric coated metal 스텐트에 대한 연구가 많이 진행되고 있다. van der Giessen등105)은 polyglycolic acid/polylactic acid,. 1. 방사선요법(Irradiation Therapy). polycaprolactone, polyhydroxybutarate valerate,. 스텐트재협착의 매우 중요한 기전인 신생내막증식. polyorthoester,. polyethylenoxide/polybutylene. 은 다른 조직의 손상후 치유과정과 유사하며 이것은. terepthalate 등의 biodegradable polymer와 non-. ionizing irradiation에 의해 억제가 가능하다. 이러한. bio-degradable polymer인 polyurethane, silicone,. 이유에서 재협착방지에 대한 방사선요법은 지속적인. polyethylene terephthalate는 동물실험에서 심한 염. 연구가 이루어져 왔다.. 증반응을 유발한다고 보고하여 이러한 polymer의 사. 초기의 체외방사선요법(external irradiation)의 연. 용은 매우 비관적이며, high-molecular-weight po-. 구들에서 신생내막증식 억제효과가 서로 상이하였는. ly-L-lactic acid106), fibrin107), polyamine plus. 데 연구모델에 따른 혈관손상의 정도와 방사선조사. dextran sulfate trilayer4)의 사용은 낙관적이다. Ben-. 85,86,87). . Porcine coronary. estent-II pilot study4)에서 heparin coated Pal-. ba-lloon overstretch model 등 여러 재협착모델. maz-Schatz 스텐트를 사용한 결과 스텐트재협착율. 에서 catheterbased endovascular γ 혹은 β-irra-. 은 13%로 놀라운 감소를 보였다. 그러나 대상환자가. diation은 radioactive source에 관계없이 10~18. 매우 제한되었음을 감안해야 하며, heparin coated. Gy 이상을 준 경우 신생내막증식을 의의있게 줄이고. Palmaz-Schatz 스텐트의 항혈전효과와 신생내막증. dose-dependent한 억제효과는 6개월 후에도 지속. 식 억제효과는 확실히 증명되지 않았고, 다른 poly-. 량의 차이 때문으로 생각된다. - 256 -.
(7) mer들105)과는 달리 polyamine plus dextran sulfate. 확실하지 않다. 가장 많이 시행되는 방법은 풍선성형술. trilayer polymer coated Palmaz-Schatz 스텐트가. 로 성공율이 높고 낮은 합병증을 보이고 있다. 스텐트. 인체내에서 심한 신생내막증식을 유발하지 않는다는. 재협착의 풍선성형술에서 내경증가의 중요기전은 신. 것은 증명되었다. Heparin이외에 Hirudin/Prostacy-. 생내막의 compression과 extrusion으로 생각되었는. 108). , platelet integrin glycoprotein IIb/IIIa. 데116-119), Mehran등120)은 내경증가의 56%는 스텐트. Antibody (AZ1)109), PLA/PEG hirudin/iloprost110),. 의 추가 확장에 의해서 나머지 44%는 신생내막의 감. clin analog. 111). NO donor. 의 신생내막증식 억제효과에 대한 연구들. 소에 의해서 이루어지며, 잔여협착은 18±12%로 비 교적 높다고 하였다. 비교적 좋은 조기 및 임상 추적 성. 이 진행 중이다.. 적을 보이는데, Reimer등119)은 평균 24개월후의 임상. 3. 기타요법 EPILOG(Evaluation in PTCA to Improve Longterm Outcome with Reopro Glycoprotein IIb/IIIa blockade) trial의 stent substudy와 ERASER(Evaluation of Reopro After Stenting to Eliminate Restensosis) trial에서 항혈소판제제인 glycoprotein IIb/IIIa receptor inhibitor의 전신투여 효과가 연 구되고 있고81), DISTRESS(Dispatch Stent Restenosis Study)에서 dispatch catheter를 이용한 heparin local delivery효과에 대한 연구가 진행중이 다81). 그외에 anti-allergic, anti-keloid drug인 Tranilast112)와 somatostatin analogue인 angiopeptin113)이 신생내막증식 억제효과가 있다고 하며, endothelial see-ding 혹은 sodding114,115)에 대한 연구 도 진행중이다.. 적 재협착율을 18%로 보고하였다. 스텐트내의 신생내막조직을 제거하는 방법으로 rotational atherectomy121), directional atherectomy122), extractional atherectomy123), laser angioplasty 124,125) 등이 시행되고 있다. 비교적 병변이 길고 심한 경우 주로 사용되고 있으며, 조기성적은 좋으나 풍선성형을 같이해 야 하며 재재협착율이 비교적 높다122). Laser angioplasy를 제외한 조직제거술의 경우 스텐트 disruption의 위험이 있으므로 혈관내초음검사를 하여 혈관 내로의 스텐트 strut protrusion 유무를 확인해야 한 다126). 현재 진행되고 있는 LARS(Laser Angioplasty versus PTCA for Restenosis in Stents) trial의 결과가 기대된다81). Satler127)는 스텐트재협착의 치료로 focal type, 특히 Palmaz-Schatz 스텐트의 관절부 재협착, 스. 4. 스텐트 시술방법, 스텐트 디자인과 재질. 텐트+풍선성형술, diffuse type은 풍선성형술 단독. 이미 언급한 바와 같이, 스텐트재협착의 예방을 위. 혹은 조직제거술+풍선성형술을 권유하고 있으며. 해서는 전 병변을 스텐트로 덮는(full lesion cove-. 조직제거술전에는 혈관내초음파검사로 신생내막증. rage) 개념이 중요하다고 생각되며, 풍선/혈관 비율. 가의 정도, 불충분한 스텐트확장 유무, 스텐트 strut. 과 확장압력에 의한 혈관손상의 정도와 신생내막증. protrusion 유무 등을 확인하는 것이 중요하다고. 식 및 재협착의 정도가 유의한 관계가 있고 이러한 현. 하였다.. 상은 작은 혈관에서 더욱 심하므로, 스텐트 시술시. 결. “the bigger, the better”라는 기존의 개념이 재고되. 론. 어야 한다고 생각된다. 스텐트 디자인, 재질, 확장방법 등과 확장시 스텐트 geometry와 혈관손상, 신생내막. 스텐트로 인하여 우리는 관상동맥성형술의 재협착. 증식 및 재협착의 관계에 대한 더 많은 연구들이 필요. 방지로의 첫걸음을 시작했다. 그러나 아직 스텐트재. 하다.. 협착율은 높아서 또 재협착을 해결해야 하는 난관에 부딪혀 있다. 현재 스텐트재협착의 예방과 치료에 관. 스텐트재협착의 치료. 해서 활발한 연구가 진행되고 있는 상태이며, 이러한 연구들은 비록 제한된 것이지만 스텐트재협착에 대. 현재 스텐트재협착의 치료로 어떤 방법이 좋은가는. 한 더 새로운 연구를 수행하고 실질적인 전략을 세. - 257 -.
(8) 우는데 기여하는 바가 매우 크다고 생각된다. 스텐트 재협착의 중요한 기전인 신생내막증식은 예방과 치 료차원의 다각적 접근이 같이 이루어져야 해결할 수. 8). 있을 것으로 생각된다.. References 1) Califf RM, Fortin DF, Frid DJ, et al:Restenosis after coronary angioplasty:an overview. J Am Coll Cardiol 66:3-6, 1991 2) Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrsnd V, Materne P, Belardi J, Sigwart U, Colombo A, Goy JJ, van den Huevel P, Morel MA, for the Benestent Study group : A comparison of balloon-expandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 331:489-495, 1994 3) Fischman DL, Leon MD, Baim D, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R, Almond D, Teirstein PS, Fish RD, Colombo A, Brinker J, Moses J, Shaknovich A, Hirshfeld J, Bailey S, Ellis S, Rake R, Goldberg S:A randomized comparison of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 331:496-501, 1994 4) Serruys PW, Emanuelsson H, van der Giessen W, Lunn AC, Kiemeney F, Macaya C, Rutsch W, Heyndrickx G, Suryapranata H, Legrand V, Goy JJ, Materne P, Bonnier H, Morice MC, Fajadet J, Belardi J, Colombo A, Garcia E, Ruygrok P, de Jaegere P, Morel MA on behalf of the Benestent-II Study Group:Heparin-coated Palmaz-Schatz stents in human coronary arteries:early outcome of the Benestent-II pilot study. Circulation 93 : 412-422, 1996 5) Fenton SH, Fischman DL, Savage MP, Schatz RA, Leon MB, Baim DS, King SB, Heuser RR, Curry RC, Rake RC, et al:Long-term angiographic and clinical outcome after implantation of balloon-expandable stents in aortocoronary saphenous vein grafts. Am J Cardiol 74: 1187-1191, 1994 6) Roubin GS, Cannon AD, Agrawal SK, Macander PJ, Dean LS, Baxley WA, Breland J:Intracoronary stenting for acute and threatened closure complicating precutaneous transluminal coronary angioplasty. Circulation 85:916-927, 1992 7) Hearn JA, King SB III, Douglas JS, Carlin SF, Lembo NJ, Ghazzal ZMB:Clinical and angiographic outcomes after coronary stenting for acute or threanted closure after. 9). 10). 11). 12). 13). 14). 15). 16). - 258 -. percutaneous transluminal coronary angioplasty. Initial result with a balloon-expandable, stainless steel design. Circulation 88:2086-2096, 1993 Ali NM, Lowry RW, Tawa CB, Joseph J, Abukhalil J, Marks GF, DeFelice C, Kleiman NS, Raizner AE:Predictors of restenosis after Gianturco-Roubin coronary st-ent deployment. Analysis of 135 consecutive patients from a single center(abstr). J Am Coll Cardiol 23:71A, 1994 Kiemeneij F, Laarman GJ, vsn der Wieken R, Suwarganda J: Emergency coronary stenting with the PalmazSchatz stent for failed transluminal coronary angioplasty:results of a learning phase. Am Heart J 126:2331, 1993 Colombo A, Goldberg SL, Almagor Y, Maiello L, Finci L : A novel strategy for stent deployment in the treatment of acute or threanted closure complicating balloon coronary angioplasty. Use of short or standard(or bo-th)single or multiple Palmaz-Schatz stents. J Am Coll Cardiol 22:1887-1891, 1993 Foley JB, Brown RIG, Penn IM : Thrombosis and restenosis after stenting in failed angioplasty: Comparison with elective stenting. Am Heart J 128:12-20, 1994 Schomig A, Kastrati A, MUdra H, et al:Four-year experience with Palmaz-Schatz stenting in coronary angioplasty complicated by disection with threanted or present vessel closure. 90:2716-2724, 1994 Masotti M, Serra A, Fernandez-Aviles F, Alonso J, Colman T, Zueco J, Delcan JL, Garcia E, Gimeno F, Calabuig J, Betriu A : Stent vs angioplasty restenosis trial (START). Angiographic results at six month follow-up (abstr). Circulation(Suppl I) 94:I-685, 1966 Ellis GS, Savage M, Fischman D, Baim DS, Leon M, Goldberg S, Hirshfield JW, Clemen MW, Teirstein PS, Walker C, Bailey S, Buchbinder M, Topol EJ, Schatz RA:Restenosis after placement of Palmaz-Schatz stent in native coronary arteries:initial results of a multicenter experience. Circulation 86:1836-1844, 1992 Schomig A, Kastrati A, Dietz R, Rauch B, Neumann FJ, Katus HH, Busch U:Emergency coronary stenting for dissection during percutaneous transluminal coronary angioplasty:angiographic follow-up after stenting and after repeat angioplasty of the stented segment. J Am Coll Cardiol 23:1053-1060, 1994 Savage MP, Fischman DL, Schatz RA, Tierstein PS, Leon MB, Baim D, Ellis SG, Heuser R, Walker CM, Curry RC, Gebhardt S, Rake R:Long term angiographic and clinical outcome after implantation of balloon-expanda-ble stent in the native coronary circulation. Palmaz-Sch-atz Stent Study Group. J Am Coll.
(9) Cardiol 24:1207-1212, 1994 17) Foley JB, Brown RIG, Penn IM:Restenosis following elective implantation of single Palmaz-Schatz stents in de-novo lesions in native vessels. Coro Art Dis 5:73-80, 1994 18) van der Giessen WJ, Emanuelsson HU, Dawkins KD, Rutsch W, Sigwart U, Heydrickx GR, Katus HA, Serruys PW:Six months clinical outcome and angiographic follow-up of the WEST study(abstr). Eur Heart J(Suppl) 17:411, 1996 19) Mori M, Kurogane H, Hayashi T, Yasaka Y, Ohta S, Kajiya T, Takarada A, Yoshida A, Matsuda Y, Nakagawa K, Murata T, Yoshida Y, Yokoyama M:Comparison of results of intracoronary implantation of the PalmazSchatz stent with conventional balloon angioplasty in chronic total coronary arterial occlusion. Am J Cardiol 78:985-989, 1996 20) Goldberg SL, Colombo A, Maiello L, Borrione M, Finci L, Almagor Y:Intracoronary stent insertion after balloon angioplasty of chronic total occlusion. J Am Coll Cardiol 26:713-719, 1995 21) Suttorp MJ, Mast EG, Plokker HWT, Kelder JC, Ernst SMPG, Bal ET:Primary coronary stenting after successful balloon angioplasty of chronic total occlusion:A single-center experience(abstr). Circulation(Suppl I) 94: I-687, 1966 22) Eeckhout E, Stauffer JC, Vogt P, Debbas N, Kappenberger L:A comparison of intracoronary stenting with conventional balloon angioplasty for the treatment of new onset stenoses of the right coronary artery. Am Heart J In press 23) Colombo A, Ferraro M, Itoh A, Martini G, Blengino S, Finci L:Results of coronary stenting for restenosis. J Am Coll Cardiol 28:830-836, 1996 24) de Jaegere P, Serruys PW, Bertrand M, et al:Angiographic predictors of recurrence of restenosis after Wiktor stent implantation in native coronary arteries. Am J Cardiol 72:165-170, 1993 25) de Scheerder IK, Strauss BH, de Feyter PJ, Beatt KJ, Baur LH, Wijns W, Heyndrix GR, Suryapranata H, van den Brand M, Buis B, et al:Stenting of venous bypass graft: A new treatment modality for patients who are poor candidates for reintervention. Am Heart J 123:10461054, 1992 26) Strauss BH, Serruys PW, Bertrand ME, Puel J, Meier B, Goy JJ, Kappenberger L, Rickards AF, Sigwart U: Quantitative angiographic follow-up of the coronary Walls-tent in native vessels and bypass grafts(European expe-rience-March 1986 to March 1990). Am J Cardiol 69:475-481, 1992 27) Piana RN, Moscucci M, Cohen DJ, Kugelmass AD, Sen-. 28). 29). 30). 31). 32). 33). 34). 35). 36). 37). - 259 -. erchia C, Kuntz RE, Baim DS, Carrozza JP:PalmazSchatz stenting for treatment of focal vein graft stenosis: Immediate results and long-term outcome. J Am Coll Cardiol 23:1296-1304, 1994 Wong SC, Baim DS, Schatz RA, Teirstein PS, King SB, Curry RC, Heuser RR, Ellis SG, Cleman MW, Overlie P, et al:Immediate results and late outcomes after stent implantation in saphenous vein graft lesions:the multi-center US Palmaz-Schatz stent experience. The Palmaz-Schatz Stent Study Group. J Am Coll Cardiol 26:704-712, 1995 Fischman D, Savage MP, Bailey S, Werner JA, Rake R, Goldberg S:Predictors of restenosis after saphenous vein graft interventions(abstr). Circulation(Suppl I) 94:I-621, 1966 Yokoi H, Nobuyoshi M, Nosaka H, Kimura T, Yokoi H, Hamasaki N, Nakagawa Y, Tamura T, Nakano Y, Hayashi F: Coronary stenting for long lesions(lesion length >20mm)in native coronary arteries : Comparison of three different types of stent(abstr). Circulation(Suppl I)94:I-685, 1966 Hasse J, Klopper HJ, Silberer E, Weil J, Troger B, Schwarz F, Stroger H, Preusler W, Reifart N:Stenting without oral anticoagulation : Single-centre experience with 1500 stent implantations for coronary revascula-rization(abstr). Eur Heart J(Suppl)17 : 411, 1996 Rau T, Tschirner BI, Mathey DG, Schofer J:Comparison of restenosis rates after placement of PalmazSchatz stents and AVE micro stents(abstr). Eur Heart J (Suppl)17:179, 1996 Post MJ, Borst C, Kuntz RE:The relative importance of arterial remodeling compared with intimal hyperplasia in lumen renarrowing after balloon angioplasty. Circulation 89:2816-2821, 1994 Schwartz RS, Huber KC, Murphy JG, Edwards WD, Camrud AR, Vlietstra RE, Holmes DR:Restenosis and the proportional neointimal response to coronary artery injury:Result in a porcine model. J Am Coll Cardiol 19:267-274, 1992 Mintz GS, Pichard AD, Kent KM, Satler LF, Popma JJ, Leon MB: Intravascular ultrasound comparison of restenotic and de novo coronary artery narrowings. Am J Cardiol 74:1278-1280, 1994 Mintz GS, Popma JJ, Pichard AD, Kent KM, Satler LF, Wong SC, Hong MK, Kovach JA, Leon MB:Arterial remodeling after coronary angioplasty: A serial intravascular ultrasound study. Circulation 94: 35-43, 1996 Kimura T, Kaburagi S, Yokoi H, Nakagawa Y, Nobuyoshi M, Mintz GS, Popma JJ, Leon MB:Time co-.
(10) 38). 39). 40). 41). 42). 43). 44). 45). 46). 47). 48). urse of geometric remodelling after coronary angioplasty(abstr). Eur Heart J(Suppl)17:219, 1996 Painter JA, Mintz GS, Wong SC, Popma JJ, Pichard AD, Kent KM, Satler LF, Leon MB : Serial intravascular ultrasound studies fail to show evidence of chronic Palm-az-Schatz stent recoil. Am J Cardiol 75: 398-400, 1995 Gordon PC, Gibson CM, Cohen DJ, Carrozza JP, Kuntz RE, Baim DS:Mechanism of restenosis and redilatation within coronary stents : Quantitative angiographic assessment. J Am Coll Cardiol 21:1166-1174, 1993 Karas SP, Gravanis MB, Santoian EC, Robinson KA, Anderberg KA, King SB:Coronary intimal proliferation after balloon injury and stenting in swine : An animal model of restenosis. J Am Coll Cardiol 20:467474, 1992 Dussaillant GR, Mintz GS, Pichard AD, Kent KM, Satler LF, Popma JJ, Wong SC, Leon MB:Small stent size and intimal hyperplasia contribute to restenosis : A volumetric intravcascular ultrasound analysis. J Am Coll Cardiol 26:720-724, 1995 Hoffmann R, Mintz GS, Dussaillant GR, Popma JJ, Pichard AD, Satler LF, Kent KM, Griffin J, Leon MA: Patterns and mechanisms of in-stent restenosis. A serial intrafvascular ultrasound study. Circulation 94: 1247-1254, 1996 Schwartz RS, Holmes DR, Topol EJ:The restenosis paradigm revisited : An alternative proposal for cellular mechanism. J Am Coll Cardiol. 20:1284-1293, 1992 Clowes AW, Reidy MA, Clowes MM:Kinetics of cellular proliferation after arterial injury:Smooth muscle growth in the absence of endothelium. Lab Invest 49: 327-333, 1983 Carter AJ, Laird RJ, Farb A, Kufs W, Wortham DC, Virmani R:Morphological characteristics of lesion formation and time course of smooth muscle cell proliferation in a porcine proliferative restenosis model. J Am Coll Cardiol 24:1398-1405, 1994 Scott NA, Cipolla GD, Ross CE, Dunn B, Martin FH, Simonet L, Wilcox JN:Identification of a potential role for the adventitia in vascualr lesion formation after balloon overstretch injury of porcine coronary arteries. Circulation 93:2178-2187, 1996 Kearney M, Pieczek A, Haley L, Schanifeld R, Rosenfield K, Isner JM : Histopathology of stent restenosis(abstr). Circulation(Suppl I)94:I-620, 1966 Degawa T, Mistuo K, Tsunoda T, Sakatani H, Nakamura S, Yamaguchi T:Differential mechanism of late lumen loss after Palmaz-Schatz stenting:Evaluation by serial. 49). 50). 51). 52). 53). 54). 55). 56). 57). 58). 59). - 260 -. intravascular ultrasound study(abstr). Circulation(Suppl I)94:I-200, 1966 Mehran R, Mintz GS, Pichard AD, Satler LF, Hong MK, Hoffmann R, DeForty D, Morgan C, Griffin J, Leon MB:Impact of vessel wall injury on in-stent restenosis:A serial quantitative angiographic and intravascular ultrasound study(abstr). Circulation(Suppl I)94:I-262, 1966 Yokoi H, Kimura T, Nobuyoshi M:Palmaz-Schatz coronary stent restenosis: Pattern and management. J Am Coll Cardiol 23:117A, 1994 Sturm M, Hausmann D, Nolte CWT, Jost S, Blessing E, Hausleiter J, Amende I:Analysis of the location of restenotic lesions after Palmaz-Schatz stent implantation(abstr). Eur Heart J(Suppl)17:307, 1996 Ikari Y, Hara K, Tamura T, Saeki F, Yamaguchi T:Luminal loss and site of restenosis after Palmaz-Schatz coronary stent implantation. Am J Cardiol 76: 117120, 1995 Werner F, Regar E, Klauss V, Henneke KH, Theisen K, Mudra H:Does a different stent design lead to a different pattern of neointimal proliferation?(abstr). Eur Heart J(Suppl)17:373, 1996 Kastrati A, Schomig A, Dietz R, Neumann FJ, Richardt G:Time course of restenosis during the first year after emergency coronary stenting. Circulation 87 : 14981505, 1993 Masotti M, Serra A, Matias F, Patricio L, Brines R, Tura A, Betriu A : Long-term quantitative angiographic follow-up after coronary stent implantation(abstr). Eur Heart J (Suppl)17:308, 1996 Asakura M, Ueda Y, Hirayama A, Adachi T, Sakata Y, Sakata Y, Mishima M, Kodama K:Neointima covering stent became thinner and transparent at 3 years follow-up:Serial angioscopic and angiographic observation (abstr). Circulation(Suppl I)94:I-454, 1966 Colombo A, Hall P, Nakamura S, Gaglione A, Maiello L, Blegngino S, Martini G, Ferraro M:Angiographic follow-up and restenosis results after Palmaz-Schatz intracoronary stenting without anticoagulation(abstr). Circulation 90(Suppl I):I-124, 1994 Lablanche JM, Danchin N, Grollier G, Bonnet JL, Bedossa M, Vahanian A, McFadden EP, Gauthier L, Bauters C, Bertrand ME:Factors predictive of restenosis after stent implantation managed by ticlopidine and aspirin (abstr). Circulation(Suppl I)94:I-256, 1966 Nunes G, Pinto I, Mattos L, Feres F, Chaves A, Tanajura L, Centemero M, Abizaid AC, Sousa A:Coronary stent implantation in vessels smaller than 3mm is associated with higher restenosis rates(abstr). Eur Heart J(Suppl)17:173, 1996.
(11) 60) Romero M, Suarez de Lezo J, Medina A, Pan M, Hernandez E, Segura J, Melian F, Ruiz M, Zayas R, Ortega JR:Elective stenting for the treatment of lesions located in small coronary arteries(abstr). Eur Heart J (Suppl) 17:217, 1996 61) Fernandez-Aviles F, Alonso JJ, Duran JM, Gimeno F, San Roman JA, Fuente L, Munoz JC, Bermejo J, Garcia E, Paniagua J:Clinical and angiographic restenosis after coronary stenting. Incidence and predictors(abstr). Eur Heart J(Suppl)17:307, 1996 62) Carrozza JP, Kuntz RK, Schatz RA, Leon MB, Goldberg S, Savage M, Fischman D, Senerchia C, Diver DJ, Baim DS:Inter-series differences in the restenosis rate of Palmaz-Schatz coronary stent placement: Differences in demographics and post-procedure lumen diameter. Ca-thet Cardiovasc Diag 31:173-178, 1994 63) Waksman R, Shen Y, Ghazzal Z, Scott NA, Douglas Jr JS, King III SB:Optimal balloon inflation pressure for stent deployment and correlates of stent thrombosis and in-stent restenosis(abstr). Circulation(Suppl I)94:I258, 1966 64) Pulsipher MW, Baker WA, Sawchak SR, Harrison JK, Sketch MH, Wang A, Phillips HR, Stack RS, Zidar JP: Outcomes in patients treated with multiple coronary stents(abstr). Circulation(Suppl I) 94:I-332, 1966 65) Yokoi H, Nobuyoshi M, Nosaka H, Kimura T, Yokoi H, Hamasaki N, Nakagawa Y, Tamura T, Nakano Y, Hayashi F:Palmaz-Schatz stent implantation in calcified lesions : Immediate and follow-up results(abstr). Circulation(Suppl I)94:I-453, 1966 66) Moussa I, Di Mario C, Mosses J, Di Francesco L, Reimers B, Tobis J, Colombo A:The impact of preinterventional plaque area determoned by intravascular ultrasound on luminal renarrowing following coronary stenting(abstr). Circulation(Suppl I)94:I-261, 1966 67) Savage MP, Fischman DL, Rake R, Hirshfeld J, Penn I, Heuser R, Shaknovich A, Moses J, Ricci D, Goldberg S:Effects of lesion morphology on angiographic outcome after balloon angioplasty and coronary stenting: results from the STRESS trial(abstr). Circulation 90 (Suppl I):I-324, 1994 68) Mehran R, Mintz GS, Bucher TA, Greenberg A, Satler LF, Hong MK, Kent KM, Griffin J, Pichard AD:Aortoostial instent restenosis : Mechanisms, treatment, and results. A serial quantitative angiographic and intravascular ultrasound study(abstr). Circulation(Suppl I)94: I-200, 1966 69) Mittal S, Weiss DL, Hirshfeld JW, Kolansky DM, Herrmann HC:Restenotic lesions have a worse outcome after stenting(abstr). Circulation(Suppl I)94 : I-331, 1966. 70) Amant C, Bauter C, Bodart JC, Lablanche JM, Grollier G, Danchin N, Hamon M, Richard F, Helbecque N, Mc Fadden EP, Amouyel P, Bertrand ME:The D allele of the angiotensin I-converting enzyme is a major risk factor for restenosis after coronary stenting(abstr). Circulation(Suppl I) 94:I-619, 1966 71) Ribichini F, Steffenino G, Dellavalle A, Camilla T, Piazza A, Matullo G, Benetton G, Griffo R, Uslenghi: Plasma angiotensin-converting enzyme levels, and insertion/deletion polymorphism of the enzyme, as predictors of restenosis after elective coronary stenting (abstr). Eur Heart J(Suppl)17:95, 1996 72) Colombo A, Hall P, Nakamura S, Almagor Y, Maiello L, Gaglione A, Goldberg S, Tobis JM: Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation 91:16761688, 1995 73) Hoffman R, A de Very E, Mintz GS, Pichard AD, Kent KM, Deible R, Salter LF:Intravascular ultrasound predictors of restenosis at the margins of Palmaz-Schatz stents(abstr). Circulation(Suppl I)94: I-199, 1966 74) Metz JA, Fitzgerald PJ, Oshima A, Hayase M, Weissman NJ, DJ Diver, Moses J, Pepine CJ, Uren NG, Oesterle SN, Yock PG:Impact of intravascular ultrasound guid-ance on stenting in the CRUISE substudy (abstr). Circul-ation(Suppl I)94:I-199, 1966 75) Strain JE, Rehman DE, Fischman D, Cohen N, Moses JW, for the Stress III Investigators. STRESS III:Preliminary acute results of IVUS vs. Non-IVUS stenting (abstr). Circulation(Suppl I)94:I-200, 1966 76) Sutton CS, Consigny PM, Thakur M:Thrombogenecity of intravascular stent wires(abstr). Circulation 90(Suppl I):I-9, 1994 77) Scott NA, Robinson KA, Nunes GL, Thomas CN, Viel K, King SB, Harker LA, Rowland SM, Juman I, Cipolla GD et al:Comparison of the thrombogenecity of stainless steel and tantalum coronary stents. Am Heart J 129: 866-872, 1995 78) Roger C, Edelman ER:Endovascular stent design dictates experimental restenosis and thrombosis. Circulation 91:2995-3001, 1995 79) Squire JC, Rogers C, Edelman ER:Stent geometry during inflation influences later restenosis(abstr). Circulation(Suppl I)94:I-259, 1966 80) Sheth S, Litvack F, Dev V, Fishbein MC, Forrester JS, Eigler N:Subacute thrombosis and vascular injury resulting from slotted-tube nitinol and stainless steel stents in a rabbit carotid artery model. Circulation 94: 1733-1740, 1996 81) Pepine CJ, Holmes DR, et al:Coronary artery stents: ACC Expert Consensus Document. J Am Coll Cardiol. - 261 -.
(12) 28:782-794, 1996 82) Woscoboinik JR, Gordov EP, Boussignac G, DuboisRande JL, Dupouy P, Aptecar E, Kern MJ, Geschwind HJ: Difference in flow characteristics for different stent models: Implications for stent design from results of an in vitro study(abstr). Circulation(Suppl I) 94: I-260, 1966 83) Hofma SH, van Beusekom HMM, Whelan DMC, van der Giessen WJ:Prolonged vessel wall injury after coronary stenting with different stent design(abstr). Eur Heart J(Suppl)17:172, 1996 84) Beythien C, Gutensohn K, Hamm C, Bau J, Terres W, Meinertz T:Stent length and platelet activation:A flow cyotometry analysis(abstr). Eur Heart J(Suppl)17 : 177, 1996 85) Schwartz RS, Koval TM, Edwards WD, Camrud AR, Bailey KR, Browne K, Vlietstra RE, Holmes DR:Effect of external beam irradiation on neointimal hyperplasia after experimental coronary artery injury. J Am Coll Cardiol 19:1106-1113, 1992 86) Shimatakahara S, Mayberg MR:Gamma irradiation inhibits neointimal hyperplasia in rats after arterial injury. Stroke 25:424-428, 1994 87) Hehrlein C, Kaiser S, Kollum M, Kinscherf R, Metz J, Fritz P:External beam radiation fails to inhibit neointima formation in stented rabbit arteries(abstr). Circula-tion 94:I-210, 1996 88) Wiedermann JG, Marboe C, Amois H, Schwartz A, Weinberger J : Intracoronary irradiation markedly reduces restenosis after balloon angioplasty in porcine model. J Am Coll Cardiol 23:1491-1498, 1994 89) Waksman R, Robinson KA, Crocker IR, Gravanis MB, Cipolla GD, King SB III:Endovascular low-dose irradiation inhibits neointima formation after coronary artery balloon injury in swine : A possible role for radiation therapy in restenosis prevention. Circulation 91:1533-1539, 1995 90) Verin V, Popowski Y, Urban P, Belenger J, Redard M, Costa M, Widmer M, Rouzaud M, Nouet P, Grob E, Schwager M, Kurtz JM, Rutishauser W:Intra-arterial beta irradiation prevents neointimal hyperplasia in a hypercholesterolemic rabbit restenosis model. Circulation 92:2284-2290, 1995 91) Wiedermann JG, Marboe C, Amois H, Schwartz A, Weinberger J : Intracoronary irradiation markedly reduces neointimal proliferation after balloon angioplasty in swine:persistent benefit at 6-month follow-up. J Am Coll Cardiol 25:1451-1456, 1995 92) Waksman R, Robinson KA, Crocker IR, Gravanis MB, Palmer SJ, Wang C, Cipolla GD, King SB III:Intracoronary radiation before stent implantation inhibits. 93). 94). 95). 96). 97). 98). 99). 100). 101). 102). - 262 -. neointima formation in stented porcine coronary arteries. Circulation 92:1383-1386, 1995 Waksman R, Robinson KA, Crocker IR, Wang C, Gravanis MB, Cipolla GD, et al:Intracoronary lowdose beta irradiation inhibits neointim a formation after coronary artery balloon injury in the swine restenosis medel. Circulation 92:3025-3031, 1995 Verin V, Popowski Y, Urban P, Belneger J, Redard M, Costa M, et al:Intraarterial beta irradiation prevents neointimal hyperplasia in hypercholesterolemic rabbit restenosis medel(abstr). J Am Coll Cardiol 2A, 1995 Waksman R, Robinson KA, Crocker IR, Gravanis MB, Palmer SJ, Cipolla GD:Intracoronary beta radiation before versus after stent implantation for inhibition of neointimal formation in the porcine model(abstr). Circulation(Suppl I)94:I-619, 1966 Teirstein PS, Nassullo V, Jani S, Russo RJ, Schatz RA, Steuterman S, Morris NB, Tripuraneni P:A randomized, clinical trial of radiation therapy to reduce restenosis following coronary stenting-early results(abstr). J Am Coll Cardiol 27:15A, 1996 Teirstein PS, Massullo V, Jani S, Popma JJ, Mintz GS, Russo RJ, Schatz RA, Steuterman S, Morris NB, Guarneri EM:Radiation therapy following coronary stenting-6 month follow-up of a randomized clinical trial(abstr). Circulation 94:I-210, 1996 Urban P, Verin V, Popowski Y, Schwager M, Papirov I, Chatelain P, Kurtz JM, Rutishauser W:Clinical feasibility and safety of intraluminal beta irradiation to prevent restenosis after coronary balloon angioplasty (abstr). Circulation(Suppl I)94:I-210, 1996 Fischell TA, Kharma BK, Fischell DR, Loges PG, Coffey CW, Duggan DM, Naftilan AJ:Low-dose, bparticle emission from‘stent’wire results in complete localized inhibition of smooth muscle cell proliferation. Circulation 90:2956-2963, 1994 Hehrlein C, Stintz M, Kinscherf R, Schlosser K, Huttel E, Friedrich L, Fehsenfeld P, Kubler W:Pure β-particle-emitting stents inhibit neointima formation in rabbits. Circulation 93:641-645, 1996 Laird JR, Carter AJ, Kufs WM, Hoopes TG, Farb A, Nott SH, Fischell RE, Fischell DR, Virmani R, Fischell FA:Inhibition of neointimal proliferation with lowdose irradiation from a β-particle-emitting stent. Circulation 93:529-536, 1996 Rivard A, Leclerc G, Bouchard M, Janicki C, Roorda S, Beaudion G, Carrier R:Low-dose-β-emitting radioactive stents inhibit neointimal hyperplasia in porcine coronary arteries:an IVUS assessment(abstr). Circulation(Suppl I)94:I-210, 1966.
(13) 103) Carter AJ, Laird JR, Bailey LR, Hoopes TG, Farb A, Fischell DR, Fischell RE, Fischell TA, Virmani R: Effects of endovascular radiation from a β -particleemitting stent in a porcine coronary restenosis model: A dose-response study. Circulation 94 : 2364-2368, 1996 104) van der Giessen WJ, Serruys PW:b-particle-emitting stents radiate enthusiasm in the search for effective prevention of restenosis. Circulation 94 : 2358-2360, 1996 105) van der Giessen WJ, Lincoff M, Schwartz RS, van Beusekom HMM, Serruys PW, Holmes DR, Ellis SG, Topol EJ:Marked inflammatory sequelae to implantation of biodegradable and nonbiodegradable polymers in procine coronary arteries. Circulation 94: 1690-1697, 1996 106) Tanguay JF, Zidar JP, Phillips HR III, Stack RS:Current status of biodegradable stents. Cardiol Clin 12: 699-713, 1994 107) Holmes DR, Camrud AR, Jorgenson MA, Edwards WD, Schwartz RS:Polymeric stenting in porcine coronary artery model: Differential outcome of exogenous fibrin sleeves versus polyurethane-coated stents. J Am Coll Cardiol 24:525-531, 1994 108) Prietzel K, Pasquantonio JD, Fliedner TU, Stemberger A, Janczewski : Inhibition of neointimal proliferation with a novel, hirudin/prostacyclin analog eluting stent coating in an animal overstretch model(abstr). Circulation(Suppl I) 94:I-260, 1966 109) Aggarwal RK, Martin W, Ireland DC, Azrin MA, de Bono PD, Gershlick AH:Effects of polymer-coated stents eluting antibody to platelet integrin plycoprotein IIb/IIIa on platelet deposition and neointima formation(abstr). Eur Heart J(Suppl)17:176, 1996 110) Pasquantonio J, Beilharz C, Preter D, Fliedner T, Prietzel K, Schmeller ML, Stemberger A, Alt E, Schomig A:A new hirudin/prostacyclin analog releasing polylactic acid stent coating reduces restenosis in sheep(abstr). Eur Heart J(Suppl)17:177, 1996 111) Folts JD, Maalej N, Keaney JF, Loscalzo J:PalmazSchatz stents coated with a NO donor reduces reocclusion when placed in pig carotid arteries for 28 days (abstr). J Am Coll Cardiol 27:86A, 1996 112) Hsu YS, Tamai H, Ueda K, Ono S, Kosuga K, Tanaka S, Matsui S, Motohara S, Uehata H:Efficacy of Tranilast on restenosis after coronary stenting(abstr). Circulation (Suppl I)94: I-620, 1966 113) Hong MK, Kent KM, Tio FO, Foegh ML, Wong SC, Cathapermal S, Bramwell O, Leon MB:Continuous subcutaneous angiopeptin reduces neointimal hyperplasia in a porcine coronary in-stent restenosis model. (abstr). Circulation(Suppl I)94:I-620, 1966 114) Vinogradsky B, Sawa H, Guala A, Lundgren C, Fuji S: Seeding of stents with genetically modified endothelial cells:Overexpression of Urokinase receptor results in increased seeded cell retension(abstr). Circulation(Suppl I) 94:I-261, 1966 115) Bailey SR, Decento YJ, Eugene S:Endothelial “ SODDING ”: Intraprocedural replacement of endothelial cells on endovascular stents(abstr). Circulation(Suppl I) 94:I-261, 1966 116) MacDonald RG, O’Neill BJ, Creighton JE, Brown RIG, Slivocka JE, Penn IM:Is coronary stent expansion the mechanism for successful dilation of stent restenosis? A quantitative angiographic study(abstr). Circulation (Suppl II)84:II-96, 1991 117) Garrat K, Holmes D, Schwartz R, Camrud A, Jorgenson M:Balloon dilatation of restenotic lesions within metallic coronary stents : Initial clinical and histopathologic observation(abstr). J Am Coll Cardiol 19: 109A, 1992 118) Gordon PC, Gibson CM, Cohen DJ, Carrozza JP, Kuntz RE, Baim DS:Mechanism of restenosis and redilation within coronary stents-quantitative angiographic assessment. J Am Coll Cardiol 21:1166-1174, 1993 119) Reimer B, Di Mario C, Tucci G, Ferraro M, Martini G, Blengino S, Moussa I, Colombo A:Long-term clinical outcome after interventional treatment of stent restenosis(abstr). Eur Heart J(Suppl)17:308, 1996 120) Mehran R, Mintz GS, Popma JJ, Pichard AD, Satler LF, Kent KM, Griffin J, Leon MB:Mechanisms and results of balloon angioplasty for the treatment of instent restenosis. Am J Cardiol 78:618-622, 1966 121) Buchbinder M, Goldberg SL, Fortuna R, Braden G, Tierstein P, Di Mario C, Moses J, Almagor Y, Katopodis JN, Blau N, Bailey SR:Rotational atherectomy for intra-stent restenosis:initial experience(abstr). Circulation (Suppl I) 94:I-621, 1966 122) Strauss BH, Umans VA, van Suylen RJ, de Feyter PJ, Marco J, Robertson GC, Renkin J, Heyndrickx G, Vuzevski VD, Bosman FT, et al:Directional atherectomy for treatment of restensosis within coronary stents : Clinical, angiographic and histologic results. J Am Coll Cardiol 20:1465-1473, 1992 123) Goods CM, Jain S, Liu MW, Babu RB, Roubin GS: Intravascular ultrasound-guided transluminal extraction atherectomy for restenosis after Gianturco-Roubin coronary stent implantation. Cathet Cardiovasc Diagn 37: 317-319, 1996 124) Koster RP, Koschyk DH, Kahler J, Steffen W, Terres W, Hamm CW:Laser angioplasty of in-stent restensosis (abstr). Circulation(Suppl I)94:I-621, 1966. - 263 -.
(14) 125) Koster R, Hamm C, Koschyk DH, Terres W, Steffen W, Kahler J, Meinertz T:Laser angioplasty of restenotic and occluded stents(abstr). Eur Heart J(Suppl)17: 308, 1996 126) Bowerman RE, Pinkerton CA, Kirk B, Waller BF:. Disruption of a coronary stent during atherectomy for restenosis. Cathet Cardiovasc Diagn 24 : 248-251, 1991 127) Satler LF: “Remedies”for in-stent restenosis. Cath Cardiovasc Diagn 37:320-321, 1996. - 264 -.
(15)
수치

관련 문서
Heparin-coated Wiktor stents in human coronary arteries (MENTOR trial).. Kiemeney F, Macaya C, Rutsch W, Heyndrickx G, Suryapr- anata H, Legrand V, Goy JJ, Materne P, Bonnier H,
It is well known that a hypersurface of an almost oontact metric manifold or of an odd- dimensional sphere with canonical contact 'structure admits an (j, g, U, v, A)-structure,
Kim K, Lee SJ, Seo J, Suh YJ, Cho I, Hong G-R, Ha J-W, Kim YJ and Shim CY (2022) Assessment of aortic valve area on cardiac computed tomography in symptomatic bicuspid
지질학회지 제 51권 제 1호, p 53 66, (2015년 2월) J Geol Soc Korea, v 51, no 1, p 53 66, (February 2015) DOI http //dx doi org/10 14770/jgsk 2015 51 1 53 ISSN 0435 4036 (Print)
