소장폐색은 응급실에서 자주 볼 수 있는 급성 복증의 원인 이며, 임상증상과 환자의 병력 및 영상진단검사로 진단된다. 급 성복증의 많은 경우는 수술적 처치 없이 치료가 되나 일부는 수술이나 이에 따르는 치료를 해야 하므로 영상진단으로 외과 적 질환을 가려내고, 정확한 원인을 알아내는 것이 중요하다.
소아 소장 폐색의 원인은 일반적으로 장중첩증과 충수염이 가장 흔하다. 그 외 수술 후 유착, 내 헤르니아(Internal hernia), 농양, 결핵, 염증성 장질환, 메켈씨 게실, 회전이상 (malrotation), 소장종양, 난소염전 등 다양한 원인이 있다(1- 4).
단순복부사진은 장폐색의 진단 시에 첫 번째로 사용되는 영 상 검사이나, 폐색의 정확도는 46%-80%이다(1, 2). 그리고 정확한 폐색 부위와 원인 및 감돈 여부를 알아내는 정확도는 더 낮다. 다음 단계로 시행할 수 있는 검사법은 장관 내 조영 제를 이용한 검사 방법이다. 특히 고위관장법(enteroclysis)은 심한 정도의 부분 폐색과 다발성의 불완전한 폐색을 규명하는
데 많은 도움이 된다. 하지만, 급성 완전 폐색, 혹은 감돈과 천 공이 동반된 고도의 장폐색에는 금기이다. 또한, 장운동이 급 격히 떨어져 있는 환자에도 사용해서는 안 된다. 최근에는 장 폐색의 진단에 CT가 큰 역할을 수행하고 있다. CT는 장벽의 병변 외에 장간막, 장간막 혈관, 골반강의 병변도 평가할 수 있 으며 즉각적인 수술을 요구하는 감돈으로 인한 장간막 허혈 여부를 다른 영상진단법보다 정확히 진단할 수 있다(1-4).
저자들은 소아 장폐색의 원인질환을 알아보고, 소장폐색의 원인 질환의 진단과 위치파악에서 CT 의 유용성에 대해서 알 아보고자 하였다.
대상과 방법
본 연구는 1998년 1월부터 2003년 12월까지 6년 동안 임 상적 또는 복부 단순촬영에서 급성 장폐색의 징후나 증상을 보였던 소아 환아 중 CT를 시행하고 비수술적 치료 또는 수 술로 확진된 19명을 대상으로 하였다. 환자의 나이는 평균나 이가 6.2세(5개월-15세)였고, 남 여비는 10:9이었다. 신생아
소아의 소장폐색: 진단과 위치 파악에 있어 CT의 유용성1
이영철・김영통・배원경・김일영
목적: 소장폐색의 원인 질환 진단과 폐색 위치 확인에 CT의 진단적 유용성을 알아보고자 하였 다.
대상과 방법: 소장폐색이 의심되어 CT검사를 시행한 환아 중 원인질환이 규명된 19명의 소아
환자를 대상으로 하였다. 신생아와 십이지장 폐색은 제외했다. CT 소견은 장간막과 장간막 혈 관의 병변, 소장벽 비후, 막힌 장폐색, 감돈 등을 분석하여 원인질환을 진단하고 소장 폐색의 위치를 알아보았다. 폐색의 위치는 다섯 부위로 나누었다. 수술 전 진단명과 확진이 된 후의 진단명과 비교하였다.
결과: 본 연구에서 소장폐색 원인 질환은 장중첩증(n=6), 충수돌기천공(n=4), 경장간막 내 헤 르니아(n=2), 수술 후 유착(n=1), 원인불명의 다발성 띠형성(n=1), 이물질(자두씨) (n=1), 소장선암(n=1), 메켈씨 게실염(n=1), 결핵성 복막염(n=1), 살모넬라장염에 의한 장천공 (n=1)이었다.
CT 소견은 장간막울혈(n=13), 대망 또는 장간막 침윤(n=10), 국소적 소장벽 비후(n=7)와 막힌 장폐색(n=3), 감돈(n=1)등 이었다. 소장 폐색의 위치는 CT 소견으로 모든 예(n=19) 에서 알 수 있었다. 장폐색의 원인 파악은 14예(74%)에서 CT로 진단 가능 하였으며 5예에서 는 진단이 어려웠다.
결론: 소아의 소장폐색의 원인은 다양하며, CT는 소장 폐색의 원인과 위치를 평가하는데 도움 을 된다.
1순천향대학교 천안병원 영상의학과
이 논문은 2004년 10월 29일 접수하여 2007년 11월 1일에 채택되었음.
와 십이지장 폐색은 제외했다. 19명의 환아 중 17명은 수술로 확진하였고, 2명의 환아는 비수술적 치료를 통해 확진되었는 데 이중 1명은 바륨정복술로 장중첩증으로, 1명은 대장내시경 을 이용한 조직생검을 통해 결핵으로 진단받았다. 19명의 환 아 중 3명에서 이전에 장 수술 병력이 있었는데 1명은 급성충 수염으로, 1명은 신생아 때 말단 소장폐색으로 회맹장문합술 (ileocecectomy)을, 1명은 선천성거대결장으로 수술받은 과거 력이 있었다.
사용된 CT 기종은 8 채널의 MDCT인 GE Prospeed와 GE Lightspeed Ultra(GE medical systems, Milwaukee, U.S.A.) 를 사용하였고 , 모든 환아는 1 mL/kg의 비이온성 경정맥 조 영제 Iopromide(Ultravist, Schering, Seoul, Korea)를 자동주 입기(MCTPlus, Medrad, Pittsburgh, PA, U.S.A.)를 이용하여 1 mL/sec로 주입하여 5 mm 절편 두께와 5 mm 절편 간격으
로 횡격막 상연에서 골반강 하연까지 CT 촬영을 시행하였다.
그러나 조영제의 경구 주입 혹은 항문을 통한 조영제 주입은 시행하지 않았다.
CT 사진 분석은 장폐색의 원인질환 및 폐색의 위치를 모르 는 상태에서 2명의 영상의학과 의사의 합의로 후향적 분석을 하였으며 주로 소장폐색의 원인 질환과 폐색의 위치를 분석하 였다.
CT 소견은 혈관 울혈이나 대망 또는 장간막 침윤, 소장 벽 비후, 막힌 장폐색, 감돈(strangulation), 복수, 충수돌기결석, 림프절 종대 등을 평가하였다. 혈관 울혈은 장간막 혈관 분포 에 따라 명확히 조영되는 혈관들이 비교적 매끈한 모양을 보 이며 확장된 경우로 하였으며, 대망 또는 장간막 침윤은 불규 칙한 선상의 섬유화 또는 소결절이 있거나 주변 혈관벽이 불 명확한 경계면을 보이는 경우 등을 비정상 소견으로 보았다.
A
B
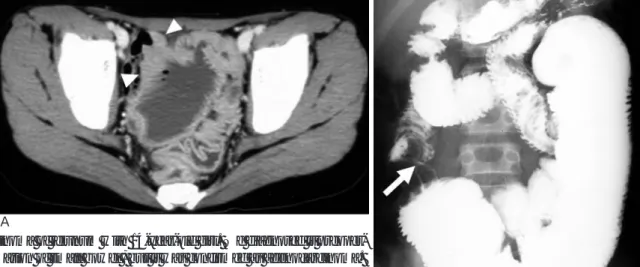
Fig. 2. Foreign body (plum stone) in terminal ileum in a 9-year-old girl.
She had operated ileocecectomy due to distal small bowel obstruction during neonatal period. We diagnosed it preoperatively as partial small bowel obstruction caused by foreign body.
A. Small bowel series show 2 cm sized, ovoid filling defect (arrow) in terminal ileum near the anastomotic site of the previous ileocecectomy (arrowhead).
B. CT scan show 2 cm sized intraluminal foreign body (arrow).
A B
Fig. 1. Appendiceal perforation with abscess in 5-year-old girl.
A, B. CT scans show enhanced bowel wall thickening and periappendiceal abscess in right lower quadrant abdomen and pelvic cavity.
장관벽의 두께는 3 mm이상을 비정상 소견으로 보았으며, 막 힌 장폐색의 CT 소견은 C-모양, U-모양 또는“coffee bean”
모양의 장관과 꼬인(torsion) 부위로 장간막 혈관이 수렴하는 (converging) 모양을 보이는 경우로 하였다. 장 점막이 조영 증강을 보이지 않을 때 감돈으로 진단하였고, 림프절 종대는 10 mm 이상을 비정상소견으로 보았다(1-4).
소장 폐색의 위치는 국소적 소장벽 비후, 막힌 장폐색, 폐색 이행부위, 장중첩증을 시사하는 과녁소견을 보이는 부위로 결 정하였고 각각 우상복부, 우하복부, 좌상복부, 좌하복부, 골반 강으로 나뉘었고 상하, 좌우의 경계는 배꼽을 기준으로 하였 다. 그리고 수술 전 진단명과 확진이 된 후의 진단명과 비교
하였다.
결 과
본 연구에서 소장폐색 원인 질환은 장중첩증(n=6), 충수돌 기천공(n=4) (Fig. 1), 경장간막 내 헤르니아(n=2), 수술 후 유착(n=1), 원인불명의 다발성 띠형성(n=1), 이물질(자두씨) (n=1) (Fig. 2), 소장선암(n=1), 메켈씨 게실염(n=1), 결핵 성 복막염(n=1), 살모넬라장염에 의한 장천공(n=1)이었다.
소장폐색의 CT 소견은 장간막 혈관울혈(n=13), 대망 또는 장간막 침윤(n=10), 국소적인 소장벽 비후(n=7) (Fig. 3), 막
B A
Fig. 3. Adenocarcinoma of jejunum with 14-year-old girl. We diagnosed it preoper- atively as inflammation of small bowel , but it was confirmed as adenocarcinoma.
A. CT scan shows markedly dilated small bowel with wall thickening (arrow- heads) in pelvic cavity.
B. Small bowel series shows annular luminal narrowing of jejunum (arrow) with markedly distended proximal jejunum.
A B
Fig. 4. Transmesenteric internal hernia in 10-year-old boy. We diagnosed it preoperatively as small bowel obstruction with strangu- lation caused by small bowel volvulus . It was confirmed as closed loop obstruction caused by transmesenteric internal hernia.
A. Contrast-enhanced CT scan demonstrates lack of bowel wall enhancement in affected loop (a), but other unaffected bowel loops (b, c) show minimal mucosal enhancement (arrow).
B. Operative photograph shows mesenteric defect (arrow) and strangulated bowel loops (arrowhead).
힌 장폐색(n=3) (Fig. 4, 5)등이 주로 보였으며, 감돈의 소견 은 경장간막 내 헤르니아의 1예에서 보였다(Fig. 4). 복수는 충수돌기천공(n=1), 메켈씨 게실염(n=1)에서 보였다. 림프절 종대는 결핵성 복막염(n=1)과 경장간막 내 헤르니아(n=1)에 서 보였다. 충수돌기천공 환아 4예중 2예에서 충수결석(n=2) 과 골반농양(n=1)을 보였고, 살모넬라장염에 의한 장천공은 우하복부에 다발성의 농양을 보였다.
소장 폐색의 위치는 CT소견으로 모든 예(n=19)에서 알 수 있었고 우상복부(n=2), 우하복부(n=10), 좌상복부(n=2), 좌 하복부(n=2), 골반강(n=3)이었으며, 수술 소견과도 일치하였 다.
소아 소장폐색의 원인 질환은 14예(74%)에서 CT로 진단 이 가능 하였고(Fig. 1, 2) CT로 진단이 어려웠던 경우는 5 예(36%)였다. CT로 진단할 수 있었던 질환은 장중첩증(n=6), 충수염에 의한 장천공(n=4), 경장간막 내 헤르니아(n=1), 수 술 후 유착(n=1), 이물질(자두씨) (n=1), 결핵성복막염 (n=1)이었다(Table 1). 근위부장관 내부에 원위부 장관이 끼 어들어가는 특징적인 과녁모양을 보이면 장중첩증으로 진단하 였고(1-3, 5) 우하복부와 골반강에 국한된 염증과 장벽비후 및 조영증강, 농양 내 혹은 인접한부위에 충수돌기결석이 보 이면 충수염에 의한 장천공으로 진단하였다(2, 6-8). 장관의 수렴과 장간막의 결손부위를 통한 주요 장간막 줄기(main
mesenteric trunk)의 전위를 보이면 경장간막 내 헤르니아로 진단하였고(1-4, 9), 이전에 수술 병력이 있고, CT에서 장폐 색을 일으킬만한 특별한 원인이 없는 경우에 수술 후 유착으 로 진단하였다(2-4). 조영 전 CT에서 하복부 장관 내에 고 음영의 이물질이 보여 이물질에 의한 장폐색으로 진단하였고 (2, 10-12), 하복부에 1 cm 이상 커져 있는 다발성의 염증성 림프절, 그리고 장과 장간막에 심한 염증성 침윤이 있으면 결 핵성 복막염으로 진단하였다(1-4).
CT로 진단이 어려웠던 질환은 경장간막 내 헤르니아(n=1) (Fig. 4), 원인불명의 다발성 띠(n=1) (Fig. 5), 소장선암 (n=1) (Fig. 3), 메켈씨 게실염(n=1) (Fig. 6), 살모넬라장염 에 의한 장천공(n=1) 이었다(Table 1).
고 찰
장관 폐색의 진단 및 원인의 평가에는 단순 복부 촬영과 장 관 조영술이 이용되기도 하나, 진단이 어려울 수 있다. 장관 폐 색유무와 원인의 진단, 폐색위치 파악에는 CT가 유용한 검사 방법이다. (나선식전산화단층촬영(Helical CT))는 빠른 영상 기법으로 장관 벽을 포함한 다양한 복부 장기의 관류정도를 정확히 알 수 있으며, 심각한 합병증 및 허혈 등도 평가할 수 있다. 최근에는 다평면재구성 영상(multiplanar reformatted
A
B
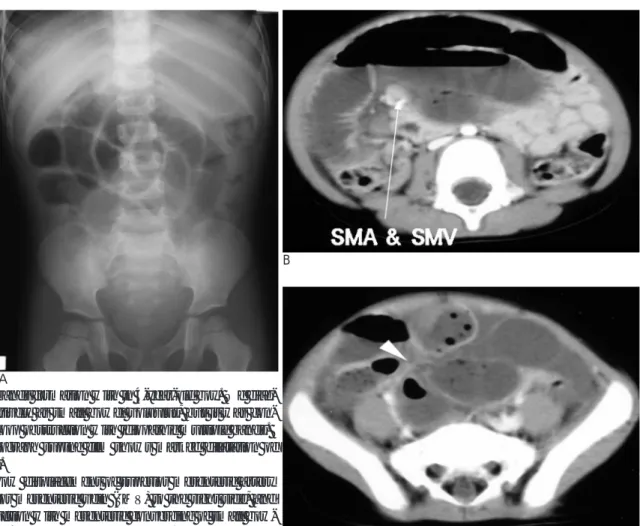
Fig. 5. Idiopathic bands formation with in 4-year-old boy. We diag- nosed it preoperatively as small bowel volvulus, but it was con- firmed by closed loop obstruction with idiopathic multiple bands.
A. Abdomen radiograph supine film shows marked dilatation of small bowel loops.
B, C. CT scans show displacement of superior mesenteric artery (SMA) and superior mesenteric vein (SMV) to the right side, and closed loop obstruction with mesenteric converging of small bow- el loops (arrowhead) in the right lower abdomen. C
image) 기법의 도움으로 소장 폐색의 진단에 더 많은 도움을 준다.
소장 폐색의 흔한 원인은 성인에서는 수술 후 유착이며(약
50%-75%), 소아에서는 장중첩증과 충수염이 가장 흔하다 (1-4). 그리고 본 연구에서도 소아 소장 폐색의 원인으로 장 중첩증이 31%(n=6)로 가장 많았으며, 수술 후 유착은 1예로
A B
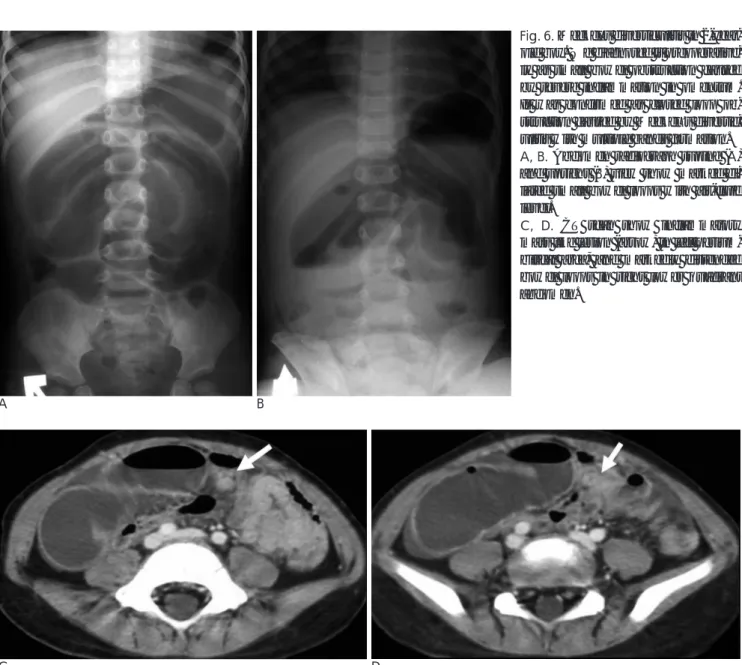
Fig. 6. Meckel’s diverticulitis in 2-year- old boy. We diagnosed it preoperative- ly as small bowel obstruction caused by severe inflammation in omentum.
It was confirmed as closed loop ob- struction caused by Meckel’s divertic- ulitis with multiple bands formation.
A, B. Abdomen radiograph supine (A) and upright (B) view show marked di- lated small bowel loops with air-fluid level.
C, D. CT scan show inflammatory mass like lesion (arrow) in left perium- bilical area, and markedly distended bowel loops in right lower quadrant abdomen.
C D
Table 1. CT Predictability and Findings of Small Bowel Obstruction
Mesenteric Omental or Localized Closed Correct
Causes vascular mesenteric bowel wall loop preop.
prominence infiltration thickening obstruction by CT(%)
Intussusception (6) 4 2 06 (100)
Appendiceal perforation (4) 2 4 3 04 (100)
Transmesenteric internal hernia (2) 2 2 01 (50)
Postoperative bands (1) 1 01 (100)
Idiopathic multiple bands (1) 1 1 1
Foreign body (Plum Stone) (1) 1 01 (100)
Small bowel adenocarcinoma (1) 1
Meckel’s diverticulitis (1) 1 1 1
Salmonellar enteritis with bowel perforation (1) 1 1 1
Tuberculous peritonitis (1) 1 1 01 (100)
계 (n=19) 13 10 7 3 14 (74)
일반적 통계와 비교했을 때 낮은 빈도를 보였는데, 이는 연구 된 예가 19명으로 상대적으로 적었고, 또한 이전에 장관 수술 병력이 있는 소아에서는 수술 후 유착성 장폐색이 많아서 복 부 CT를 시행하지 않고, 바로 응급 개복수술을 시행했기 때 문으로 생각된다.
본 연구에서는 CT에서 가장 흔한 소견은 장간막 혈관울혈 (n=13), 대망 또는 장간막 침윤(n=10)등의 소견이었다. 원인 불명의 다발성 띠형성의 1예와 2예의 경장간막 내 헤르니아 에서 막힌 장폐색의 소견을 보였는데 3예 중 1예에서만 수술 전 원인질환의 진단이 가능하였기 때문에, 막힌 장폐색의 여 부와 병변의 위치 파악은 CT로 가능하였으나 원인진단을 규 명하기는 어려웠다.
본 연구에서 국소적 소장벽 비후, 장중첩증을 시사하는 과 녁소견, 막힌 장폐색, 폐색이행부위 가 있는 부위를 판단하여 모든 예(n=19)에서 폐색의 위치를 알아낼 수 있었다.
저자들의 연구에서 CT에서 장관 폐색의 원인 진단이 가능 했던 질환은 장중첩증, 충수돌기천공, 수술 후 유착, 이물질(자 두씨), 결핵성 복막염이며, 진단이 어려웠던 질환은 소장선암, 원인불명의 다발성 띠형성, 메켈씨 게실염, 살모넬라장염에 의 한 장천공 등이었다. 경장간막 내 헤르니아는 1예는 진단이 가 능하였으나 1예는 진단이 어려웠다.
장중첩증은 CT에서 장간막지방을 포함하고 있는 근위부장 관 내부에 원위부 장관이 끼어들어가는 특징적인 과녁모양을 보이며 CT로 진단이 쉽다(2, 3).
충수염의 천공으로 말미암은 소장폐색은 우하복부와 골반강 에 국한된 염증과 장벽비후 및 조영증강, 농양 내 혹은 인접 한 부위에 충수돌기결석이 보이면 진단할 수 있다. 하지만, 충 수염에 비해 빈도가 흔치 않은 다른 원인에 의한 말단 소장 혹 은 맹장의 장천공과 감별이 어려울 때가 있다(2, 6-8). 본 연 구에서도 3세 된 여아에서 우하복부와 골반강 내 농양, 그리 고 장벽비후를 보여서 수술 전에 급성 충수염으로 진단하였는 데 수술 후 살모넬라 장염에 의한 소장 천공으로 판명되었다.
경장간막 내 헤르니아의 CT소견은 장관의 수렴과 장간막 혈 관의 이상소견을 보이는데, 장간막혈관의 울혈 및 군집과 장 간막의 결손부위를 통한 주요 장간막 줄기의 전위를 보인다 (2, 9). 저자의 1예에서 장간막의 결손부위를 통한 주요 장간 막 줄기의 전위를 보여 진단하였으나, 1예는 장간막울혈과 막 힌 장폐색을 보여 수술 전에 소장 염전증으로 진단하였다(Fig.
4).
저자들의 소장선암은 국소적인 소장 벽비후를 보였지만 주 위에 염증성 반응이 없고 소장 조영검사에서 윤상폐색을 보여 선암으로 충분히 진단할 수 있는 예로 생각되는데 경험부족으 로 인해 수술 전에 진단을 놓친 것으로 생각된다(Fig. 3).
메켈씨게실은 회맹판의 40-90 cm 이내에서 주로 발생한 다. 합병증으로는 출혈, 장폐색 또는 염증 등이다. 출혈은 회 장에 이소성 위선조직이 존재하여 궤양이 있을 때 나타나는 합병증으로 주로 2세 이하의 소아에 많으며, 장관폐색과 염증 은 성인에서 많이 보이는 합병증이다. 메켈씨게실염은 충수염,
염증성 장질환, 기타 소장폐색의 원인 질환과의 감별이 어려 워 수술 전 진단율은 10% 이하이다(2, 13-16). 저자들의 경 우에서는 2세 소아에서 메켈씨게실염에 의한 소장폐색을 보였 는데 수술 전 CT 소견은 장간막 침윤을 동반한 국소적인 벽 비후를 보여 염증성 질환에 의한 장폐색으로 수술 전에 진단 하였다(Fig. 6).
결론적으로 소아에서 소장폐색의 원인은 다양하며, CT는 소 장폐색의 원인질환과 위치를 파악하는데 쉬웠으며, CT에서 혈 관 울혈이나 대망 또는 장간막 침윤, 국소적 벽비후, 막힌 장 폐색, 농양, 충수돌기결석, 복수, 림프절 종대 등의 소견을 분 석함으로써 원인질환을 규명하는데 도움을 줄 수 있다.
참 고 문 헌
1. Jabra A.A., Fishman E.K. Small bowel obstruction in the pediatric patient. CT evaluation. Abdom Imaging 1997;22:466-470
2. Furukawa A, Yamasaki M, Furuichi K, Yokoyama K, Nagata T, Takahashi M. et al. Helical CT in the Diagnosis of Small Bowel Obstruction. Radiographics 2001; 21:341-355
3. Carty HM. Paediatric emergencies: non-traumatic abdominal emergencies. Eur Radiol 2002;12:2835-2848
4. Zalcman M, Sy M, Donckier V, Closset J, Gansbeke DV. Helical CT sign in the diagnosis of intestinal ischemia in small-bowel ob- struction. AJR Am J Roentgenol 2000;175:1601-1607
5. Hamada Y, Fukunaga S, Takada K, Sato M, Hioki K. Postoperative intussusception after incidental appendectomy. Pediatr Surg Interv 2002;18:284-6
6. Harris S, Rudolf LE. Mechanical small bowel obstruction due to acute appendicitis: review of 10 cases. Ann Surg 1996;164:157-161 7. Callahan MJ, Rodriguez DP, Taylor GA. CT of appendicitis in chil-
dren. Radiology 2002;224:325-332
8. Filippi de la Palavesa MM, Vaxmann D, Campos M, Tuchmann C, Guth S, Dietemann JL. Appendiceal stump abscess. Abdom Imaging 1996;21:65-66
9. Blachar A, Federle MP, Dodson SF. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria.
Radiology 2001;218:68-74
10. Ihara N, Yashiro N, Kinoshita T, Yoshigi J, Kasai T. Small bowel obstruction due to pickled japanese apricot: CT findings. J Comput Assist Tomogr 2002;26:132-133
11. 양면준, 하현권, 김지훈, 손민지, 김표년, 이문규 등. 소장폐색과 연 관된 식물위석의 CT 소견. 대한방사선의학회지 2001; 44: 209-215 12. Krol CM, Karol I, Khalil H, Shah S. Small-bowel obstruction due to
migratory trichobezoar in a child: CT diagnosis. AJR Am J Roentgenol 2001;177:255-256
13. Bennett GL, Birnbaum BA, Balthazar EJ. CT of meckel’s divertic- ulitis in 11 patients. AJR Am J Roentgenol 2004;182:625-629 14. Baldisserotto M, Maffazzoni DR, Dora MD. Sonographic findings
of Meckel’s diverticulitis in children. AJR Am J Roentgenol 2003;180:425-428
15. Johnston AT, Khan AL, Bleakney R, Keenan RA. Stromal tumor within a meckel’s diverticulum: CT and ultrasound findings. Br J Radiol 2001;74:1142-1144
16. Hughes JA, Hatrick A, Rankin S. Computed tomography findings in an inflamed Meckel’s diverticulum. Br J Radiol 1998;71:882-883
J Korean Radiol Soc 2007;57:571-577
Address reprint requests to : Young Tong Kim, M.D., Department of Radiology, Soonchunhyang University Cheonan Hospital, 23-20 Bongmyoung-dong, Cheonan-si, Chungnam 330-721, Korea
Tel. 82-41-570-3515 Fax. 82-41-579-9026 E-mail: [email protected]
Small Bowel Obstruction in Children:
Usefulness of CT for Diagnosis and Localization
1Young Cheol Lee, M.D., Young Tong Kim, M.D., Won Kyung Bae, M.D., Il Young Kim, M.D.
1Department of Radiology, Cheonan Hospital, Soonchunhyang University
Purpose: To evaluate the usefulness of CT for the diagnosis of the cause and localization of small bowel ob- struction.
Materials and Methods: Out of a group of children who underwent a CT examination for a suspected small bowel obstruction, 19 patients with confirmed underlying disorders were identified and included in the study.
Neonates and patients with duodenal obstruction were excluded from the study. The CT findings were ana- lyzed for the location of obstruction site, abnormalities of the mesentery and mesenteric vessels, bowel wall thickening, closed loop obstruction, and strangulation. The obstruction site was divided into five parts. The preoperative CT diagnosis was compared with the final diagnosis.
Results: Causes of small bowel obstruction were intussusception (n = 6), appendiceal perforation (n = 4), transmesenteric internal hernia (n = 2), postoperative bands (n = 1), idiopathic multiple bands (n = 1), a for- eign body (n = 1), a small bowel adenocarcinoma (n = 1), Meckel’s diverticulitis (n = 1), tuberculous peritoni- tis (n= 1) and Salmonella enteritis with bowel perforation (n = 1). The CT findings showed mesenteric vascu- lar prominence (n = 13), omental or mesenteric infiltration (n = 10), localized bowel wall thickening (n = 7), closed loops obstruction (n = 3) and strangulation (n = 1). The obstruction site was identified in all cases. The causes of obstruction could be diagnosed preoperatively in 14 cases, but a preoperative diagnosis was difficult in 5 cases.
Conclusion: The causes of small bowel obstruction in children are variable, and CT is useful for evaluating the cause and localization of small bowel obstruction.
Index words :Intestine, small Intestinal obstruction
Tomography, X-Ray computed Child