서론
장골동맥을 단독으로 침범한 동맥류(Isolated iliac arterial aneurysm)는 매우 드문 질환으로 복부에서 발생하는 동맥류 의 2% 정도로 알려져 있다(1, 2). 장골동맥류의 파열은 드물 기는 하나 대량출혈을 일으켜 매우 위험한 상태이므로 발견시 적절한 치료를 해야 한다. 기존에는 수술적 치료를 시행하였으 나 파열에 의한 응급 수술시는 40~60%에 이르는 사망률을 보이며 선택적 수술(elective surgery)을 하더라도 11%에 이른 다(1, 3-5). 최근에 인터벤션 시술을 통한 동맥류의 치료가 매 우 효과적이며 기존의 수술과 비슷하거나 우월한 성적을 보고 하고 있다(5-7). 이에 본원에서 경험하였던 장골동맥류에 대한 인터벤션 시술의 치료결과를 보고하고자 한다.
대상과 방법
2006년 10월부터 2011년 9월까지 본원을 내원한 동맥류 환 자 중 장골동맥에 국한된 총 7명의 환자를 대상으로 하였다.
남자 4명, 여자 3명으로 평균연령은 65.7세(33~79세)였다. 6 예는 증상이 없이 우연히 발견되었고 1명의 경우 좌측 총장골 동맥의 파열로 응급실에 내원하였다.
모든 환자에서 시술 전 CT와 혈관조영술로 동맥류의 크기 와 침범범위를 확인하였다. 총장골동맥만을 침범한 경우가 3 명, 총장골동맥류가 장골동맥 기시부까지 침범한 경우가 1명, 내장골동맥만을 침범한 경우가 3명이었다. 이 중 3명의 경우 양측에 동맥류가 있으나 2명의 경우 동맥류의 직경이 30 mm 이하로 크기가 작은 측은 시술을 시행하지 않았다. 이 중 1명은
J Korean Soc Radiol 2012;66(5):415-420
Received December 9, 2011; Accepted March 14, 2012 Corresponding author: Byung Seok Shin, MD Department of Radiology, Chungnam National University Hospital, 282 Munhwa-ro, Jung-gu, Daejeon 301-721, Korea.
Tel. 82-42-280-7333 Fax. 82-42-253-0061 E-mail: [email protected]
This study was financially supported by research fund of Chungnam National University in 2010.
Copyrights © 2012 The Korean Society of Radiology
Purpose: To report the results of treatment isolated iliac arterial aneurysms by in-
terventional procedures.Materials and Methods: Over a period of 5 years, 7 isolated iliac artery aneurysms
(4 in the common iliac artery, 3 in the internal iliac artery) in 7 patients (3 women, 4 men; mean age, 65.7 years) were treated using interventional procedures. The mean aneurysm size was 35 mm (range, 30-45 mm). The common iliac aneurysms were treated using a unilateral stent graft (2 balloon expandable, 2 self-expandable) with coil embolization of the internal iliac artery (n = 3), except for 1 aneurysm that rup- tured. Coil embolization alone was performed for aneurysms involving only the in- ternal iliac artery (n = 3).Results: All patients were treated successfully, except for 1 with an initial remnant
of type 2 endoleak. There were no perioperative complications. No leakage or com- plication occurred at the mean follow-up of 14 months (range 2-29 months). One patient with a ruptured aneurysm died of multi-organ failure during the follow-up period. Three aneurysms had decreased in size on follow-up CT.Conclusion: Interventional procedures with stent grafting and coil embolization are
safe and effective treatments for isolated iliac artery aneurysms.Index terms
Aneurysm Iliac Artery StentsTherapeutic Embolization
Interventional Procedures of the Isolated Iliac Arterial Aneurysm
1장골동맥에 국한된 동맥류의 인터벤션 시술
1Joon Young Ohm, MD
1, Byung Seok Shin, MD
2, Moonsang Ahn, MD
3, Mi-Hyun Park, MD
4, Ho Jun Kim, MD
51Department of Radiology, The Catholic University of Korea College of Medicine, Bucheon St. Mary’s Hospital, Bucheon, Korea Departments of 2Radiology, 3Surgery, Chungnam National University Hospital, Daejeon, Korea
4Department of Radiology, Dankook University Hospital, Cheonan, Korea
5Department of Radiology, Konyang University Hospital, Daejeon, Korea
rea)를 사용하였다. 풍선확장형 스텐트 그라프트는 먼저 10 mm 풍선카테터에 설치하여 9 Fr 피포를 통하여 설치한 후 추 가로 직경 12 mm 풍선카테터를 이용하여 완전히 확장시켰다.
자가팽창형 스텐트 그라프트를 사용한 경우 1명에서는 상부 직경 16 mm, 하부직경 12 mm, 길이 10 cm의 깔대기형(ta- pered shape)의 스텐트 그라프트를 15 Fr 피포를 통하여 설치 하였다. 나머지 1명에서는 8 Fr 피포를 통하여 직경 12 mm, 길 이 10 cm의 원통형 스텐트 그라프트를 설치하였으나 원위부에 서의 1형 endoleak가 의심되어 풍선확장술을 추가로 시행하였 으나 지속적인 유출이 관찰되어 외장골동맥까지 직경 12 mm, 길이 8 cm의 스텐트 그라프트를 추가로 설치하였다. 그러나 여전히 소량의 조영제 유출이 의심되어 2형 endoleak로 판단하 고 시술을 마쳤다(Fig. 1).
내장골동맥류에 대한 색전술은 반대측의 총대퇴동맥을 천자 하여 5 Fr 피포 내로 5 Fr 카테터를 삽입하여 골반 내 혈관조영 술과 선택적 내장골동맥조영술을 시행하고 2.0 Fr 미세도관 (ProgreatTM; Terrumo corp., Tokyo, Japan)을 이용하여 내장 골동맥의 각각의 분지동맥을 초선택하여 직경 3~6 mm의 미 세색전코일(MicroNester® Embolization coil; Cook Medical Inc., Bloomington, IN, USA)을 이용하여 모든 분지를 폐색시 켰다. 이후 동맥류에서 내장골동맥 기시부까지 직경 8~14 mm, 길이 14 cm의 색전코일(Nester®)을 이용하여 색전술을 시 행하였다. 총 14~27개(평균 20개)의 색전코일을 사용하였으며 시술 후 혈관조영술로 폐색 정도와 조영제 유출을 확인하였다.
결과
모든 환자에서 스텐트 그라프트 설치술과 혈관폐색술을 성 공적으로 시행하였다. 시술 후 추적기간은 52일에서 877일(평 균 384일)이었으며 6명에서 추적 CT를 시행하였다. 시술과 관련되거나 추적기간 중 발생한 합병증은 없었다. 각 환자의 시술과 결과에 대하여 Table 1에 정리하였다.
총장골동맥류 4명 중 총장골동맥류의 파열로 스텐트 그라프 트를 시행하였던 1명은 1일 후 시행한 CT에서 endoleak는 없 고 더 이상의 출혈은 없었으나 52일 후 다기관 기능부전으로 전신상태가 악화되어 사망하였다. 시술 후 2형 endoleak가 의 심되어 추가적인 스텐트 그라프트를 설치하였던 환자는 3개월 추적 CT에서는 더 이상의 endoleak는 보이지 않았으며 동맥류 의 직경이 36 mm에서 33 mm로 감소하였다(Fig. 1). 이외 5 개월 추적 CT를 시행한 1명은 동맥류에 endoleak는 없었고 동 맥류의 크기 변화는 없었다. 나머지 1명에서는 추적 CT검사는 시행하지 않았으나 12개월 추적기간 동안에 동맥류와 관련된 29개월 후 추적 CT에서 반대측 내장골동맥류의 크기가 30
mm로 증가되어 색전술을 시행하였으나 이는 시술 후 추적조 사가 불가능하여 본 연구에서는 제외하였다.
총장골동맥류의 크기는 30~45 mm(평균 35 mm)이며 내 장골동맥류는 32~40 mm(평균 36 mm)였다. 총장골동맥류 의 모든 예에서 대동맥 분지와 정상분절의 길이는 15~30 mm 였으나 총장골동맥만을 침범한 3명 중 2명은 내장골동맥 입구 와의 거리가 15 mm 미만이었다.
총장골동맥류의 치료로 스텐트 그라프트 설치술을 시행하였 고 내장골동맥까지 침범한 1명과 정상분절의 길이가 짧은 2명 에서는 2형 endoleak를 예방하기 위하여 내장골동맥의 기시부 를 코일로 색전술을 시행한 후 스텐트 그라프트를 설치하였다.
동맥류 파열로 응급실에 내원한 1명은 동맥류로 인하여 내장골 동맥 입구가 압박을 받고 있었고 정상동맥의 길이가 15 mm 이 상으로 측정되어 스텐트 그라프트만을 설치하였다. 내장골동 맥에만 단독으로 발생한 3명에서는 내장골동맥의 기시부까지 의 정상분절 길이가 20~70 mm(평균 43 mm)로 원위부의 각 각의 분지에서 기시부까지 색전술만을 시행하였다.
모든 환자에서 장골동맥류에 대한 확인을 위하여 동맥류가 침범한 반대측 총대퇴동맥을 천자하여 5 Fr 피포(sheath)를 삽입하고 돼지꼬리형 카테터를 복부대동맥에 위치시켜 골반혈 관조영술을 시행하였다. 동맥류의 침범범위를 확인하여 총장 골동맥류의 경우 상부로 대동맥 분지와 하부로 내장골동맥 입 구와의 거리, 그리고 정상 총장골동맥의 직경을, 내장골동맥류 의 경우 내장골동맥의 기시부위의 정상동맥의 길이와 직경을 측정하였다.
총장골동맥에 스텐트 그라프트의 설치를 위해서 3명에서는 동측 총대퇴동맥을 천자하여 8 Fr 또는 9 Fr 피포(Radiofocus®; Terrumo corp., Tokyo, Japan)를 삽입하고 스텐트 그라프트를 설치하였고 1명에서는 15 Fr 피포(S&G Biotech Inc., Seong- nam, Korea)를 삽입하기 위해 외과전문의에 의하여 총대퇴동 맥 절개술을 시행하여 피포를 삽입하고 시술하였다. 내장골동 맥의 폐색술을 같이 시행한 경우는 스텐트 그라프트를 설치하 기 전 5 Fr 카테터를 내장골동맥까지 진입시켜 직경 8~14 mm, 길이 14 cm의 색전코일(Nester® Embolization coil; Cook Medical Inc., Bloomington, IN, USA)을 폐색시켰으며 총 5~12개의 색전코일을 이용하였다.
총장골동맥류에 대한 인터벤션 시술을 초기에 시행한 2명에서 는 직경 6~12 mm, 길이 58 mm의 풍선확장형 스텐트 그라프트 (Jostent® Peripheral Stent Graft; Abbott Vasc. Inst., Rangend- ingen, Germany)를 사용하였으며 최근 시행한 2명에서는 자가 확장형 스텐트 그라프트(S&G Biotech Inc., Seongnam, Ko-
D A
E
B C
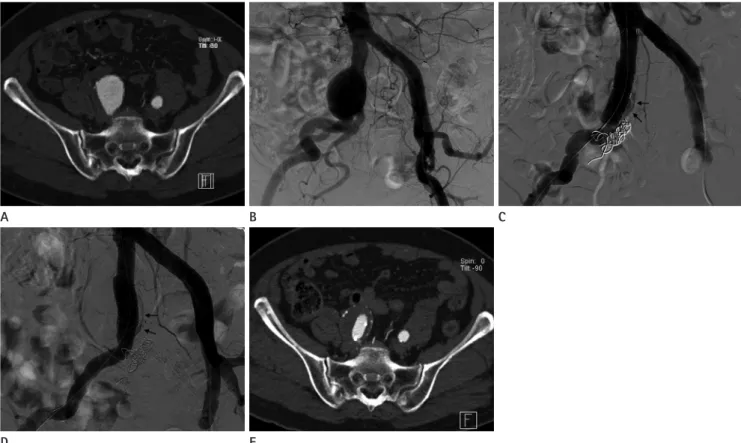
Fig. 1. Imaging results of a 77-year-old patient with a right common iliac aneurysm initially measuring 36 mm who underwent stent graft placement with coil embolization of the internal iliac artery.
A, B. Initial CT image (A) and angiogram (B) show a saccular aneurysm of the common iliac artery involving the orifice of the internal iliac ar- tery.
C. Angiography obtained after placement of the stent graft suggested a distal type 1 endoleak (arrows). Note the embolization coils in the right internal iliac artery.
D. Angiography obtained after placement of an additional stent graft into the external iliac artery with sufficient overlapping with the initial stent graft suggested a persistent endoleak (arrows), despite full dilatation of the balloon catheter. The presence of a type 2 endoleak was sus- pected after angiography.
E. CT image obtained after 3 months shows no further leakage. The size of the aneurysm has decreased to 33 mm.
Table 1. Isolated Iliac Aneurysms: Location, Interventional Procedures, and Outcomes
Pt No. Age/Sex Site Interventional Procedures Initial Result Outcome 1 79/M CIA, left
ruptured
Stent graft (D: 12 mm, L: 58 mm) Complete occlusion Died of multiorgan failure after 52 days
2 66/F CIA, right Stent graft (D: 12 mm, L: 58 mm) Coil embolization
Complete occlusion No symptoms No follow-up CT image 3 77/F CIA, right Stent graft (D: 12 mm, L: 10 and 8 cm)
Coil embolization
Endoleak (Type 2) Decrease in aneurysm size (36→33 mm) at 3 months CT
4 68/M CIA, left Stent graft (D: 16–12 mm, L: 10 cm) Coil embolization
Complete occlusion No change in aneurysm size at 5 months CT
5 33/M IIA, right Coil embolization Complete occlusion Decrease in aneurysm size (35→12 mm) at 29 months CT
6 69/M IIA, left Coil embolization Contrast filling into
of orifice
Complete occlusion
No change in aneurysm size at 8 months CT 7 68/F IIA, right Coil embolization Complete occlusion Decrease in aneurysm size (40→34 mm)
at 29 months CT Note.-CIA = common iliac artery, IIA = internal iliac artery
는 복부대동맥류와 연관이 있다고 한다(1, 2, 8).
본원에 내원한 환자와 같이 대부분의 환자는 증상이 없이 우 연히 발견되는 경우가 많으며 동맥류에 의한 증상은 주변조직 의 압박으로 인한 증상이나 혈전증, 동맥색전증으로 나타나기 도 한다. 그러나 동맥류가 파열되는 경우 복강 내로 다량의 출 혈이 있어 매우 위험하다. 파열된 장골동맥류의 크기는 평균 6 cm 이상인 것으로 알려져 있으며 직경이 3~5 cm인 경우 1년 에 2.6 mm 이상 급격히 증가하여 파열의 위험성이 증가하므 로 크기가 3 cm 내지 3.5 cm 이상인 경우 증상이 없더라도 치 료를 권장하고 있으며 증상을 동반한 경우도 반드시 치료를 하 여야 한다(1, 8-10).
장골동맥류에 대한 인터벤션 시술은 스텐트 그라프트 설치 술과 동맥색전술로 나눌 수 있다. 총장골동맥류에서 스텐트 그 라프트를 이용한 치료방침을 정하는 데 중요한 사항은 동맥류 증상은 보이지 않았다.
내장골동맥류를 코일색전술로 치료한 3명 중 내장골동맥 기 시부에 조영제가 보이던 환자는 8개월 추적 CT에서 동맥류 내 부는 혈전으로 모두 채워져 있는 것을 확인하였고 동맥류의 크 기 변화는 없었다. 나머지 2명에서는 29개월 후 시행한 추적 CT에서 동맥류의 크기는 각각 35 mm에서 12 mm로, 40 mm에서 34 mm로 감소하였다(Fig. 2).
고찰
장골동맥을 단독으로 침범한 동맥류 중 70%는 총장골동맥 에 발생하고 나머지 20~25%는 내장골동맥에 발생하며 외장 골동맥에서는 매우 드물게 발생하는 것으로 알려져 있다. 또한 양측을 동시에 침범한 경우는 30%로 알려져 있으며 10~20%
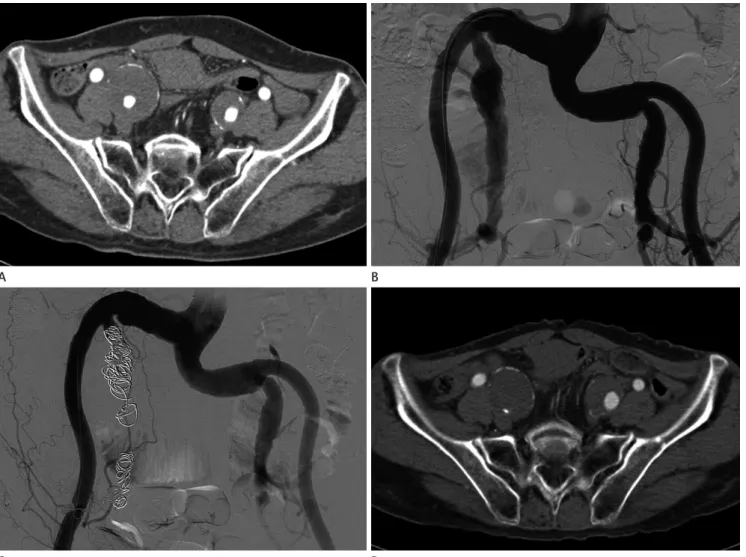
Fig. 2. Imaging results of a 68-year-old patient with a right internal iliac aneurysm initially measuring 40 mm who underwent coil embolization.
A, B. Initial CT image (A) and angiogram (B) show a large right internal iliac aneurysm and a small left internal iliac aneurysm.
C. Angiography obtained after coil embolization confirmed successful exclusion of the aneurysm.
D. CT image obtained after 29 months shows the decrease in size of right internal iliac aneurysm (40 mm→34 mm).
C D
A B
감소하였고 32개월 추적검사에서 평균 29%가 감소되었다는 보고가 있어 시술 후 endoleak가 새로이 관찰되고 동맥류의 크 기가 증가되는 경우는 반드시 추가적인 치료를 시행하여야 한 다(1, 7, 12-14).
저자들의 증례에서 시술과 관련하여 합병증이 발생하지 않 았으나 스텐트 그라프트의 설치에는 최소 8 Fr 이상의 피포를 사용하여야 하므로 총대퇴동맥부위에 혈종 등의 합병증에 유 의하여야 한다. 양측을 침범한 장골동맥류에 대한 치료시 엉덩 이나 골반의 허혈, 그리고 대장의 허혈이 발생할 수 있다. 장골 동맥류에 스텐트 그라프트 설치술 후 3년 장골동맥의 개통률 은 86~97.5%로 보고하고 있으며(6, 14-16) 스텐트 그라프트 내 혈전의 발생과 폐색, 원위부의 혈전색전증이 합병증으로 발 생할 수 있다.
결론적으로 총장골동맥 또는 내장골동맥을 단독으로 침범한 동맥류에서 스텐트 그라프트와 색전술을 이용한 인터벤션 치 료법은 안전하고 유용한 시술이다.
참고문헌
1. Uberoi R, Tsetis D, Shrivastava V, Morgan R, Belli AM; Sub- committee on Reporting Standards for Arterial Aneurysms of The Society for Vascular Surgery. Standard of practice for the interventional management of isolated iliac artery aneurysms. Cardiovasc Intervent Radiol 2011;34:3-13 2. Sandhu RS, Pipinos II. Isolated iliac artery aneurysms.
Semin Vasc Surg 2005;18:209-215
3. Dorigo W, Pulli R, Troisi N, Alessi Innocenti A, Pratesi G, Azas L, et al. The treatment of isolated iliac artery aneu- rysm in patients with non-aneurysmal aorta. Eur J Vasc Endovasc Surg 2008;35:585-589
4. Soury P, Brisset D, Gigou F, Saliou C, Angel F, Laurian C.
Aneurysms of the internal iliac artery: management strat- egy. Ann Vasc Surg 2001;15:321-325
5. Chaer RA, Barbato JE, Lin SC, Zenati M, Kent KC, McKinsey JF. Isolated iliac artery aneurysms: a contemporary com- parison of endovascular and open repair. J Vasc Surg 2008;47:708-713
6. Pitoulias GA, Donas KP, Schulte S, Horsch S, Papadimitriou DK. Isolated iliac artery aneurysms: endovascular versus open elective repair. J Vasc Surg 2007;46:648-654
7. Patel NV, Long GW, Cheema ZF, Rimar K, Brown OW, Shanley CJ. Open vs. endovascular repair of isolated iliac 의 상부와 하부에 적절한 정상동맥분절(landing zone)이 확보
가 되는가에 달려있다. 이는 1형 endoleak를 방지하기 위한 것 으로 일반적으로 landing zone은 1.5 cm를 권장하고 있다.
Uberoi 등(1)과 Stroumpouli 등(11)은 장골동맥의 침범부위와 범위, landing zone의 상태에 따라 총장골동맥류의 유형과 이 에 따른 치료방법을 다음과 같이 5가지 유형으로 분류하였다.
A형; 상부의 landing zone이 불충분한 총장골동맥류, B형;
상부와 하부의 landing zone이 충분한 총장골동맥류, C형; 하 부의 landing zone이 불충분한 총장골동맥류, D형; 내장골동 맥만 단독으로 침범한 동맥류, E형; 총장골동맥과 내장골동 맥을 동시에 침범한 동맥류이다. A형과 같이 총장골동맥의 동 맥류에서 대동맥의 분지부위까지 1.5 cm가 확보되지 않으면 비록 복부대동맥에 병변이 없더라도 분지형 대동맥 스텐트 그 라프트(bifurcated aortic stent graft)를 설치하여야 한다.
저자들이 경험한 총장골동맥에 국한된 동맥류는 상부의 landing zone이 1.5 cm 이상으로 스텐트 그라프트를 성공적으 로 설치할 수 있었다. 초기에 설치한 Jostent는 길이가 58 mm, 직경 12 mm로 길이의 제한뿐만 아니라 총장골동맥의 상부의 직경이 10 mm보다 큰 경우 시술 후 1형 endoleak의 가능성이 있어 사용에 제한이 있겠다. 또한 후기에 사용한 자가팽창형 스텐트 그라프트에서는 다양한 직경과 필요시 깔대기형으로 제작하여 사용할 수 있는 장점이 있다.
총장골동맥류의 경우 하부로 내장골동맥의 기시부와의 거 리가 짧은 경우 2형 endoleak가 발생할 수 있으며 이를 방지하 기 위해서는 코일이나 vascular plug를 사용하여 충분히 내장골 동맥폐색술을 시행하여야 한다. 이러한 내장골동맥의 기시부 위의 폐색술은 내장골동맥을 단독으로 침범한 동맥류에서도 중요하다. 내장골동맥류와 기시부까지의 길이가 짧은 경우 색 전코일로는 정확한 위치에 설치하기가 어려울 수 있어 보다 정 확한 위치에 설치할 수 있는 vascular plug를 사용하는 것이 유 용할 것으로 보인다. 그러나 기시부까지 동맥류가 침범하거나 정상동맥부위가 매우 짧은 경우 내장골동맥의 기시부의 폐색 술만으로는 불충분하여 총장골동맥이 정상이더라도 스텐트 그 라프트를 설치하여 내장골동맥의 기시부를 완전히 폐색시키는 것이 중요하다.
내장골동맥류의 경우 원위부의 많은 분지동맥에서 2형 en- doleak를 일으킬 수 있어 각각의 작은 분지동맥까지 도관을 진 입시켜 폐색을 먼저 시행하여야 하며 분지동맥의 직경이 작은 경우가 많아 미세도관으로 선택하여 색전술을 시행하는 것이 유용할 것으로 생각된다.
인터벤션 시술 후 3명에서 동맥류 크기의 감소를 보였으며 다른 연구의 3년 추적검사에서 67~83%의 환자에서 크기가
iliac artery aneurysms. J Vasc Surg 2006;44:29-37
13. Sahgal A, Veith FJ, Lipsitz E, Ohki T, Suggs WD, Rozenblit AM, et al. Diameter changes in isolated iliac artery aneu- rysms 1 to 6 years after endovascular graft repair. J Vasc Surg 2001;33:289-284; discussion 294-295
14. Tielliu IF, Verhoeven EL, Zeebregts CJ, Prins TR, Oranen BI, van den Dungen JJ. Endovascular treatment of iliac artery aneurysms with a tubular stent-graft: mid-term results. J Vasc Surg 2006;43:440-445
15. Parsons RE, Marin ML, Veith FJ, Parsons RB, Hollier LH.
Midterm results of endovascular stented grafts for the treatment of isolated iliac artery aneurysms. J Vasc Surg 1999;30:915-921
16. Scheinert D, Schröder M, Steinkamp H, Ludwig J, Biamino G. Treatment of iliac artery aneurysms by percutaneous implantation of stent grafts. Circulation 2000;102(19 Suppl 3):III253-III258
artery aneurysms: a 12-year experience. J Vasc Surg 2009;
49:1147-1153
8. Hiromatsu S, Hosokawa Y, Egawa N, Yokokura H, Akaiwa K, Aoyagi S. Strategy for isolated iliac artery aneurysms. Asian Cardiovasc Thorac Ann 2007;15:280-284
9. Bolin T, Lund K, Skau T. Isolated aneurysms of the iliac artery:
what are the chances of rupture? Eur J Vasc Surg 1988;
2:213-215
10. Santilli SM, Wernsing SE, Lee ES. Expansion rates and out- comes for iliac artery aneurysms. J Vasc Surg 2000;31(1 Pt 1):114-121
11. Stroumpouli E, Nassef A, Loosemore T, Thompson M, Mor- gan R, Belli AM. The endovascular management of iliac artery aneurysms. Cardiovasc Intervent Radiol 2007;30:
1099-1104
12. Boules TN, Selzer F, Stanziale SF, Chomic A, Marone LK, Dillavou ED, et al. Endovascular management of isolated
장골동맥에 국한된 동맥류의 인터벤션 시술
1엄준영
1· 신병석
2· 안문상
3· 박미현
4· 김호준
5목적: 장골동맥에 국한된 동맥류를 인터벤션 시술로 치료한 결과에 대하여 보고하고자 한다.
대상과 방법: 지난 5년간 7명의 환자(여자 3, 남자 4; 평균 65.7세)에서 장골동맥을 단독으로 침범한 7예의 장골동맥 류를 인터벤션 시술로 치료하였다. 동맥류의 평균 크기는 35 mm(30~45 mm)였다. 4예의 총장골동맥류는 스텐트 그라 프트(풍선확장형 2예, 자가확장형 2예)를 동측에 설치하였고 동맥류 파열로 내원한 1명을 제외한 3예에서 내장골동맥 의 코일폐색술을 병행하였다. 내장골동맥에만 국한된 동맥류 3예에서는 코일폐색술만으로 치료하였다.
결과: 모든 환자에서 시술은 성공적이었으나 1명에서 2형 endoleak가 남아있었다. 시술과 관련된 합병증은 없었으며 평 균 14개월(2~29개월)의 추적기간 중에도 endoleak나 합병증은 발생하지 않았다. 동맥류 파열로 내원한 1명은 추적기간 중 다기관 기능부전으로 사망하였다. 추적 CT에서 3예의 동맥류의 크기가 감소되었다.
결론: 장골동맥에 국한된 동맥류에 대하여 스텐트 그라프트와 코일색전술을 이용한 인터벤션 시술은 안전하고 효과적인 치료법이다.
1가톨릭대학교 의과대학 부천성모병원 영상의학과학교실, 충남대학교병원 2영상의학과, 3외과, 4단국대학교병원 영상의학과,
5건양대학교병원 영상의학과