www.krspine.org
Management of High-Grade Spinal Meningioma
Young-Hoon Kim, M.D., Ph.D., Sang-Il Kim, M.D., Ph.D., Hyung-Youl Park, M.D., Hun-Chul Kim, M.D., Chang-Hee Cho, M.D., Jong-Min Kim, M.D.
J Korean Soc Spine Surg 2021 Jun;28(2):63-69.
Originally published online June 30, 2021;
https://doi.org/10.4184/jkss.2021.28.2.63
Korean Society of Spine Surgery
Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea, 88, Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea
Tel: +82-2-831-3413 Fax: +82-2-831-3414
©Copyright 2017 Korean Society of Spine Surgery pISSN 2093-4378 eISSN 2093-4386
The online version of this article, along with updated information and services, is located on the World Wide Web at:
http://www.krspine.org/DOIx.php?id=10.4184/jkss.2021.28.2.63
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://
creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Korean Society of
Spine Surgery
Management of High-Grade Spinal Meningioma
Young-Hoon Kim, M.D., Ph.D., Sang-Il Kim, M.D., Ph.D., Hyung-Youl Park, M.D.
*, Hun-Chul Kim, M.D., Chang-Hee Cho, M.D., Jong-Min Kim, M.D.
Department of Orthopedic Surgery, Seoul St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea
*
Department of Orthopedic Surgery, Eunpyeong St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea Study Design: Review article.
Objectives: To review previous studies regarding high-grade spinal meningioma and to discuss its characteristics and proper management.
Summary of Literature Review: Although most cases of spinal meningioma are benign, some spinal meningiomas show atypical and aggressive clinical features. However, these high-grade spinal meningiomas are rare and their characteristics and proper management remain still unclear.
Materials and Methods: Review of the relevant articles.
Results: High-grade spinal meningioma shows a poorer prognosis than grade 1 spinal meningioma, with a higher recurrence rate and lower survival rate. The treatment of choice is complete resection of the tumor. If subtotal resection is performed or the histology of spinal meningioma is grade 3, adjuvant radiotherapy is considered. Systemic treatment can be considered when high-grade spinal meningioma shows metastasis and standard treatment is not feasible. However, there are drawbacks to many of these adjuvant therapies and few systemic therapies have been approved or shown to be efficacious. Recent studies have revealed genetic mutations associated with certain types of spinal meningioma, and immunotherapy is also under clinical trials.
Conclusions: High-grade spinal meningioma is a rare tumor with a poor prognosis. The initial surgical treatment is the most important factor for preventing recurrence. Adjuvant radiotherapy is considered in most cases of high-grade spinal meningioma. Due to the absence of sufficient evidence for the establishment of a treatment guideline, ongoing research and clinical trials are needed.
Key words: Spine, Meningioma, Atypical, Anaplastic, Management
Received: February 2, 2021 Revised: February 22, 2021 Accepted: May 14, 2021 Published Online: June 30, 2021
Corresponding author: Sang-Il Kim, M.D, Ph.D.
ORCID ID: Young-Hoon Kim: https://orcid.org/0000-0003-1237-4600 Sang-Il Kim: https://orcid.org/0000-0002-2758-0012 Hyung-Youl Park: https://orcid.org/0000-0002-0084-8867 Hun-Chul Kim: https://orcid.org/0000-0002-5219-2628 Chang-Hee Cho: https://orcid.org/0000-0002-6850-7284 Jong-Min Kim: https://orcid.org/0000-0002-9911-5048 Department of Orthopedic Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222, Banpo-daero, Seocho-gu, Seoul, 06591, Republic of Korea
TEL: +82-2-2258-6775, FAX: +82-2-535-9837 E-mail: [email protected]
서론
척추 수막종은 신경초종과 함께 가장 흔한 일차 척추 종양 으로, 전체 일차 척추 종양의 약 25%에서 46%를 차지한다고 보고되었다.1-4) 척추 수막종은 경막 내의 수막세포성 지주막 세포(meningothelial arachnoid cap cell)에서 기원하는 것으로 알려져 있으며, 일반적으로 경막 내 척수 외 공간에 위치하여 느리게 자라는 국한성 종양이다. 흉추에 가장 흔하지만 전 척 추에서 발생할 수 있고, 50~80세 사이의 중장년층에서 호발하 며, 남성보다 여성에서 흔하기 때문에 여성호르몬과의 관련 성에 대해서도 보고된 바 있다.1,5,6) 종양 자체로 인한 증상은 없고, 종양의 크기가 커지면서 신경을 압박하여 신경학적 증 상이 발생하여 발견된다. 2016년 세계보건기구(World Health Organization, WHO)에서 발표한 분류에 따르면 수막종은 조 직학적으로 15개의 아형이 있는데, 크게 3등급으로 나누었
다.7) 대부분의 척추 수막종은 양성 종양으로 WHO 1등급에 해 당하며, 주변 조직으로의 침습이나 전이는 하지 않고 WHO 1
Young-Hoon Kim et al Volume 28 • Number 2 • June 30 2021
www.krspine.org
64
등급의 수막종은 예후가 양호한 것으로 알려져 있다.1,5,8) 하지 만 WHO 2등급이나 3등급의 경우에서는 임상적으로 공격적 인 특징을 보이는 경우가 많다. 하지만 척추 수막종이 드문 종 양인데다가 대부분이 WHO 1등급에 해당하고, WHO 2, 3등급 에 해당하는 고등급의 척추 수막종은 아주 드물기 때문에 대 규모 연구가 부족하여 자세히 알려진 바가 없다. 본 논문에서 는 기존의 보고들을 종합하여 정리하여 보고자 한다.
본론
1. 개요
WHO의 분류법은 조직학적 특징과 세포형태학적 특징을 바탕으로 결정하여 3등급으로 나누고 있으며, 세포/조직형태 에 따라 종양의 재발이 다르다는 Perry 등의 연구가 그 기반이 되었다.7,9) 수막종에 대한 WHO 분류는 1993년에 처음 발표되 었는데, 진단기준이 모호하여 평가자간 차이가 크게 발생하였 다.10) 2000년에 발표된 개정 분류법에서는 명확한 진단기준이 제시되어 현재까지 큰 변화없이 사용되고 있다. 다만, 2000년 개정 분류법에는 고등급의 진단 기준에 포함되지 않았던 뇌
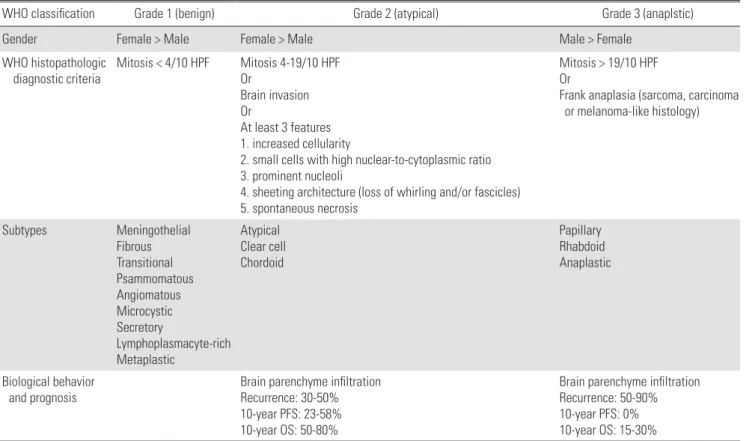
침습이 2007년 개정 분류법부터 2등급의 독립적인 진단 기준 으로 포함되었다.10) 가장 최근 개정된 것은 2016년에 발표된 것으로서, 1등급은 양성으로 9개의 아형이, 악성인 3등급에는 3개의 아형이, 비정형인 2등급에는 3개의 아형이 있다(Table
1).7,10) 10개의 고배율 현미경 검사 시야(high power field, HPF)
에서 4~19개의 유사분열이 확인되거나, 뇌를 침범하였거나, 5 가지의 세포/조직형태학적 특징 중에 3가지 이상을 가지면 2 등급으로 분류할 수 있다. 명백한 악성 세포가 확인되거나, 10 개의 HPF에서 20개 이상의 유사분열이 확인되면 3등급으로 분류한다.
수막종의 대부분은 두개골 내에 발생하기 때문에 척추 수 막종의 발생률에 대한 자료는 아직 부족하다. 2015년에 발표 된, 2004년에서 2010년까지의 미국 암 등록 자료의 분석에 따 르면, 척추 수막종의 발생률은 10만명 당 0.33명이었다.8) 등급 별 분포를 살펴보면, 대부분(96.1%)의 척추 수막종은 WHO 1 등급이었고, 2등급은 2.5%, 3등급은 1.4%를 차지하였다. 2020 년에 발표된 Systematic review에서는, 1811명의 척추 수막종 환자 중에 2등급은 63명(4.4%)이었고, 3등급은 10명(0.8%)이 었다.1) 하지만 2016년에 개정된 WHO 진단 분류법을 적용하
Table 1. Definition of WHO grade for meningioma according to the 2016 update of the WHO classification
WHO classification Grade 1 (benign) Grade 2 (atypical) Grade 3 (anaplstic)
Gender Female > Male Female > Male Male > Female
W HO histopathologic
diagnostic criteria Mitosis < 4/10 HPF Mitosis 4-19/10 HPF Or
Brain invasion Or
At least 3 features 1. increased cellularity
2. small cells with high nuclear-to-cytoplasmic ratio 3. prominent nucleoli
4. sheeting architecture (loss of whirling and/or fascicles) 5. spontaneous necrosis
Mitosis > 19/10 HPF Or
F rank anaplasia (sarcoma, carcinoma or melanoma-like histology)
Subtypes Meningothelial
Fibrous Transitional Psammomatous Angiomatous Microcystic Secretory
Lymphoplasmacyte-rich Metaplastic
Atypical Clear cell Chordoid
Papillary Rhabdoid Anaplastic
B iological behavior
and prognosis Brain parenchyme infiltration
Recurrence: 30-50%
10-year PFS: 23-58%
10-year OS: 50-80%
Brain parenchyme infiltration Recurrence: 50-90%
10-year PFS: 0%
10-year OS: 15-30%
WHO: World Health Organization, HPF: high power field, PFS: progression-free survival, OS: overall survival.
면, 비정형 수막종의 비율이 20%까지 올라간다는 보고도 있 다.10,11)
고등급의 수막종에서는 타 장기로의 전이까지 보고된 바 있
다.12,13) Kessler 등은 단일기관에서 경험한 고등급의 수막종 환
자 168명 중 6명에서 조직학적으로 확인된 전이를 확인하였 는데 그 중 폐전이가 가장 흔하였다.13)
2. 위험 인자
성별, 남성, 방사선 조사력 등이 고등급의 수막종의 위험 인 자로 알려져 있다.10) 수막종은 일반적으로 나이가 많을수록 발생률이 올라가고 50~60대에서 가장 흔히 발생하는데, 고 등급 수막종의 경우 양성 수막종보다 진단 시의 연령이 더 낮 다. 또한 양성 수막종의 경우 여성과 남성의 비율이 4:1에 달 하는데 비해 고등급 수막종의 경우 그 차이가 줄어드는 것 으로 보고되었다.10) 약 70~80%의 수막종에서 프로게스테론 수용체(progesteron receptor)와 에스트로겐 수용체(estrogen receptor)가 발현되는데, 프로게스테론 수용체 발현이 낮을수 록 수막종이 더 침습적이고 재발률도 높다고 알려져 있다.14,15) 또한 일부 환자에서 유전적인 경향을 보여, 관련된 유전인자 에 대한 연구도 활발히 이루어지고 있는데, 대표적인 것으 로 Neurofibromatosis 2 (NF2)가 있다.16) NF2는 22번 염색체 (chromosome 22q)에 위치하고 있는데, 이 유전자의 결핍이 발 생하면 수막종이 더 공격적인 특징을 보여 재발률도 높다고 알려져 있다.16)
3. 치료 1) 수술적 치료
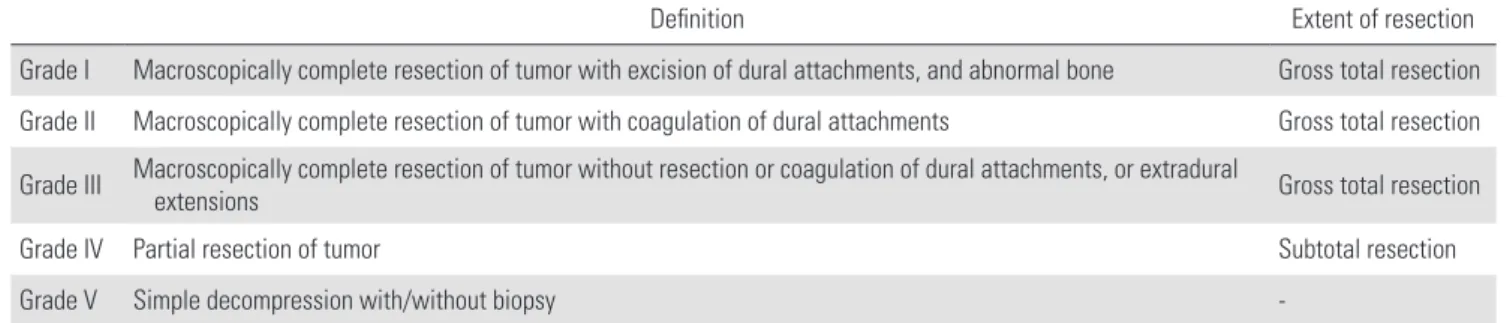
수막종의 치료는 수술적 절제이며, 완전 절제가 종양 재 발을 막기 위해 가장 중요하다. Simpson 등이 제시한 수막종 의 수술적 절제 등급을 많이 사용하는데(Table 2),17) 일반적 으로 수막종의 재발은 Simpson 1단계의 절제를 시행하였을 때 가장 낮고 4등급으로 올라갈수록 높아진다고 알려져 있
다.3,18,19) Nakamura 등은 Simpson 1단계로 절제한 43예에서 경
막에 대한 조직학적 검사를 시행하였는데, 15예(35%)에서 경
막의 내층과 외층 사이에 종양이 침범하였음을 확인하였다.18) Yamamuro 등은 Simpson 1단계로 절제한 WHO 1등급의 척추 수막종 25예에서 경막을 분석한 결과, 19예에서 경막 침범이 보였고 15예에서는 심지어 전층을 침범하였다고 보고하기도 하였다.20) 따라서 재발의 위험성이 있을 경우, Simpson 1단계 의 절제가 중요하며, 그렇지 못하면 재발에 대한 장기적인 추 시의 필요성을 언급하였다.18,20) 두개골 및 척추를 모두 포함하 는 1,571예의 수막종에 대한 치료 결과 분석에서도 Simpson 4 단계인 아전절제를 했을 경우 1-3등급의 전절제보다 재발 위 험도가 2~3배 정도 높아졌다.21) 고등급의 척추 수막종에 국 한하여 소규모의 여러 후향적 연구에서도 비슷한 결과를 확 인할 수 있다. Sun 등은 수술을 시행한 WHO 2등급의 비정형 척추 수막종 20명에 대한 후향적 분석에서, Simpson 1~3단 계 절제를 받은 18명의 환자에서 재발은 확인되지 않았으나, Simpson 4단계 절제를 받은 2명 중에 1명에서 종양이 재발하 였다고 보고하였다.22) Han 등은 20예의 고등급 척추 수막종 에 대한 수술적 치료를 시행하였는데 16예가 Simpson 2단계, 4예가 3단계의 절제를 받았고 3예(15%)에서 종양이 재발하 였다고 하였다.23) Ye 등의 보고에서, 25명의 고등급 척추 수막 종 환자(WHO 2등급: 20명, 3등급: 5명) 중에 13명의 환자에서 종양이 재발하였는데, Simpson 1-3단계의 절제보다 Simpson 4단계의 절제에서 1년이나 5년 무진행 생존율(progression- free survival, PFS)이 모두 유의하게 낮았다.24) Voldrich 등은 Simpson 1단계의 수술이 2단계보다 수술 합병증의 위험도는 높아질 수 있지만 재발률은 떨어지기 때문에, 젊은 환자에서 해부학적으로 Simpson 1단계의 절제가 가능하다면 1단계의 절제를 권고하였다.25)
2) 방사선 치료
WHO 1등급의 수막종에 비해 고등급의 수막종 환자에서 는 재발률이 높고 생존율까지 떨어진다고 알려져 있다.10,11) 따라서, 재발률을 낮추기 위한 보조 방사선 치료(adjuvant radiotherapy)를 시행하는 경우들이 있는데, 그 필요성에 대해
Table 2. Simpson grades of resection
Definition Extent of resection
Grade I Macroscopically complete resection of tumor with excision of dural attachments, and abnormal bone Gross total resection Grade II Macroscopically complete resection of tumor with coagulation of dural attachments Gross total resection Grade III M acroscopically complete resection of tumor without resection or coagulation of dural attachments, or extradural extensions Gross total resection
Grade IV Partial resection of tumor Subtotal resection
Grade V Simple decompression with/without biopsy -
Young-Hoon Kim et al Volume 28 • Number 2 • June 30 2021
www.krspine.org
66
서는 아직 논란이 있다. 특히 척추 수막종에 대한 별도의 연 구는 거의 없고 두개골 내 수막종과 함께 시행한 연구들이 대 부분이며, 이 또한 전향적 연구는 매우 부족하다. Adelberg 등
26)은 고등급의 수막종에서 방사선치료가 재발률을 낮추고 생 존율을 높인다고 하였고, Kaur 등27)도 재발률을 낮추는데 도 움이 된다고 하였다. 따라서 1등급에 비해 재발이 흔한 고등 급의 수막종에서 방사선치료가 많이 이루어져왔다. Yolcu 등 은 2004년부터 2015년까지 미국의 National Cancer Database 를 분석하여 척추 수막종에 대한 방사선치료의 비율을 조사 하였는데, 수술 후 보조 방사선치료가 시행되는 비율이 점점 높아지고 있지만 전체적인 생존율에는 유의미한 호전은 없었 다고 하였다.28) 최근에 발표된 연구들에서도 아직까지 결과 가 상반되는 경우가 많다. 일부 연구에서는 방사선치료가 재 발률을 낮추거나 악성 척추종에서는 생존율을 높일 수도 있다 고 하는 반면, 다른 연구에서는 재발률이나 생존율에 모두 유 의미한 효과가 보이지 않는다고도 하였다.11,21,29,30) 하지만 미 국 국립종합암센터네트워크(National Comprehensive Cancer Network, NCCN)의 수막종에 대한 가이드라인이나 유럽 신경 종양학회 가이드라인을 보면, 모든 고등급 수막종에 대한 수 술적 치료 후에, 절제 범위에 관계없이, 보조 치료로 방사선 치 료를 고려하도록 권고하고 있다(Fig. 1).31,32)
3) 전신 치료
수막종 세포는 유사분열 활성도가 높지 않기 때문에 항암요 법의 필요성이 떨어진다. 또한, 방사선 치료와 마찬가지로 대 단위 무작위 연구가 없기 때문에 명확한 치료법이 아직까지 없는 실정이다. NCCN에서는 단 3종류의 약물을 권유하고 있
는데, a-IFN, somatostatin receptor agonist, vascular endothelial growth factor (VEGF)이다.31) 이러한 전신치료는, 수술이나 방 사선 치료 이후 재발하거나 진행하여 같은 치료가 불가능한 경우에만 사용되고 있다. 유럽 신경종양학회에서는 증거가 부 족하기 때문에 전신치료에 대한 권고 사항이 아예 없다.
수막종에서 T-cell 등과의 면역 체계와의 관련성이 알려지면 서, 면역치료에 대한 연구가 진행되고 있다.10) 수막종 세포 또 한 면역 관문을 이용하여 면역 체계를 저해하여 국소적인 면 역저하상태를 만드는 것으로 알려져 있다. 면역 관문 경로 중 에 하나인 Programmed-death 1 (PD-1) 과 PD-1 리간드 (ligand) 인 PD-L1 가 높을수록 수막종의 등급이 높은 것으로 나타났 다. 따라서 면역 관문 억제제(immune checkpoint inhibitor)로 서 현재 항암제로 사용 중인 PD-1 항체 및 PD-L1 항체를 이용 한 임상 연구들이 진행 중에 있으며, 그 밖에 여러 면역 관문 억제제들의 치료 효과가 연구되고 있다.5,10)
4. 예후
앞서 기술한 대로, 두개골 내 수막종을 제외한 척추 수막 종 단독에 대한 보고는 많지가 않다. Setzer 등은 WHO 1등급 의 척추 수막종이 1.4%의 재발률을 보이는 것에 비해, 2등급 은 50%, 3등급은 100%의 재발률을 보였다고 하였다.2) Ye 등 의 단일 기관 연구에서 고등급 척추 수막종 25예를 분석한 결 과, 5년 내 재발률이 60%에 이른다고 하였다.24) Zhang 등은, Clear cell 수막종 환자 84명에 대해 92%에서 전절제를 시행하 였음에도 불구하고 1년, 5년, 10년 재발률이 각각 13%, 29%, 54%라고 발표한 바 있다.33) 이러한 높은 재발률은 생존율에도 영향을 미친다. Poulen 등의 보고에 따르면, WHO 2등급의 척 추 수막종 수술 이후 5년 생존율이 89.7%라고 하였다.30) 2, 3 등급을 모두 포함한 Ye 등의 보고에서는 5년 생존율이 68%였 다.24) 2004년부터 2015년까지의 미국 내 암 데이터베이스에 서 WHO 2, 3등급의 척추 수막종에 대한 자료를 분석한 결과, 287명이 확인되었는데 2등급과 3등급 사이에 생존율의 차이 는 유의미하지는 않았지만 3등급에서 낮은 경향(p=0.07)을 보 였다.34)
결론
대부분의 척추 수막종은 WHO 1등급으로, 2 등급 및 3 등급 의 고등급 척추 수막종은 드문 종양으로 아직까지 자세하게 알려져 있지 않다. 여러 연구에서 WHO 1등급의 양성 수막종 에 비해 재발률이 높고 생존율도 떨어진다고 보고되었다. 조 직학적 등급에 상관없이, 척추 수막종의 1차 치료는 종양의 전 절제이며, 아전절제를 하였거나, 3등급일 경우에는 수술 후 방 Fig 1. Summary of management strategies for high-grade spinal menin-
gioma.
사선 치료를 시행하는 것이 재발률 및 생존율에 도움이 될 것 으로 보인다. 전신치료를 위한 면역억제제 치료가 임상 연구 단계에 있지만 아직까지 치료로서의 명확한 증거는 부족한 실 정이다. 추후 수준 높은 근거들을 축적하기 위한 대단위 무작 위 대조군 연구 등이 필요하겠다.
Acknowledgements
This work was supported by a Small Grant for Exploratory Research (SGER) through the Ministry of Education of the Republic of Korea (grant number:
2018R1D1A1A02086045).
REFERENCES
1. Jamilson Ara
ú
jo Pereira B, Nogueira de Almeida A, Silva Paiva W, et al. Neuro-oncological features of spinal me- ningiomas: Systematic review. Neurochirurgie. 2020 Feb;66:41-4. DOI: 10.1016/j.neuchi.2019.09.027.2. Setzer M, Vatter H, Marquardt G, et al. Management of spinal meningiomas: surgical results and a review of the literature. Neurosurg Focus. 2007 23:E14. DOI: 10.3171/
foc-07/10/e14.
3. Hua L, Zhu H, Deng J, et al. Clinical and prognostic fea- tures of spinal meningioma: a thorough analysis from a single neurosurgical center. J Neurooncol. 2018 Dec;
140:639-47. DOI: 10.1007/s11060-018-2993-3.
4. Duong LM, McCarthy BJ, McLendon RE, et al. Descriptive epidemiology of malignant and nonmalignant primary spi- nal cord, spinal meninges, and cauda equina tumors, United States, 2004-2007. Cancer. 2012 Sep 1;118:4220-7. DOI:
10.1002/cncr.27390.
5. Huntoon K, Toland AMS, Dahiya S. Meningioma: A Re- view of Clinicopathological and Molecular Aspects. Front Oncol. 2020 10:579599. DOI: 10.3389/fonc.2020.579599.
6. Westwick HJ, Shamji MF. Effects of sex on the incidence and prognosis of spinal meningiomas: a Surveillance, Epi- demiology, and End Results study. J Neurosurg Spine. 2015 Sep;23:368-73. DOI: 10.3171/2014.12.Spine14974.
7. Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol. 2016 Jun;
131:803-20. DOI: 10.1007/s00401-016-1545-1.
8. Kshettry VR, Hsieh JK, Ostrom QT, et al. Descriptive
Epidemiology of Spinal Meningiomas in the United States.
Spine (Phila Pa 1976). 2015 Aug 1;40:E886-9. DOI:
10.1097/brs.0000000000000974.
9. Perry A, Stafford SL, Scheithauer BW, et al. Meningioma grading: an analysis of histologic parameters. Am J Surg Pathol. 1997 Dec;21:1455-65. DOI: 10.1097/00000478- 199712000-00008.
10. Wilson TA, Huang L, Ramanathan D, et al. Review of Atypical and Anaplastic Meningiomas: Classification, Molecular Biology, and Management. Front Oncol. 2020 10:565582. DOI: 10.3389/fonc.2020.565582.
11. Delgado-L
ó
pez PD, Corrales-Garcí
a EM. Role of adjuvant radiotherapy in atypical (WHO grade II) and anaplastic (WHO grade III) meningiomas: a systematic review. Clin Transl Oncol. 2020 Jul 10;10.1007/s12094-020-02434-3.12. Noh SH, Kim KH, Shin DA, et al. Treatment outcomes of 17 patients with atypical spinal meningioma, including 4 with metastases: a retrospective observational study. Spine J.
2019 Feb;19:276-84. DOI: 10.1016/j.spinee.2018.06.006.
13. Kessler RA, Garzon-Muvdi T, Yang W, et al. Meta- static Atypical and Anaplastic Meningioma: A Case Series and Review of the Literature. World Neurosurg. 2017 May;101:47-56. DOI: 10.1016/j.wneu.2017.01.070.
14. Pravdenkova S, Al-Mefty O, Sawyer J, et al. Progesterone and estrogen receptors: opposing prognostic indicators in meningiomas. J Neurosurg. 2006 Aug;105:163-73. DOI:
10.3171/jns.2006.105.2.163.
15. Hsu DW, Efird JT, Hedley-Whyte ET. Progesterone and estrogen receptors in meningiomas: prognostic consider- ations. J Neurosurg. 1997 Jan;86:113-20. DOI: 10.3171/
jns.1997.86.1.0113.
16. Zadnik PL, Gokaslan ZL, Burger PC, et al. Spinal cord tumours: advances in genetics and their implications for treatment. Nat Rev Neurol. 2013 May;9:257-66. DOI:
10.1038/nrneurol.2013.48.
17. Simpson D. The recurrence of intracranial meningiomas af- ter surgical treatment. J Neurol Neurosurg Psychiatry. 1957 Feb;20:22-39. DOI: 10.1136/jnnp.20.1.22.
18. Nakamura M, Tsuji O, Fujiyoshi K, et al. Long-term surgical outcomes of spinal meningiomas. Spine (Phila Pa 1976). 2012 May 1;37:E617-23. DOI: 10.1097/
BRS.0b013e31824167f1.
19. Kwee LE, Harhangi BS, Ponne GA, et al. Spinal meningio-
Young-Hoon Kim et al Volume 28 • Number 2 • June 30 2021
www.krspine.org
68
mas: Treatment outcome and long-term follow-up. Clin Neurol Neurosurg. 2020 Nov;198:106238. DOI: 10.1016/
j.clineuro.2020.106238.
20. Yamamuro K, Seichi A, Kimura A, et al. Histological inves- tigation of resected dura mater attached to spinal menin- gioma. Spine (Phila Pa 1976). 2012 Oct 15;37:E1398-401.
DOI: 10.1097/BRS.0b013e318268c419.
21. Behling F, Fodi C, Hoffmann E, et al. The role of Simpson grading in meningiomas after integration of the updated WHO classification and adjuvant radiotherapy. Neurosurg Rev. 2020 Oct 26; 10.1007/s10143-020-01428-7.
22. Sun SQ, Cai C, Ravindra VM, et al. Simpson Grade I-III Resection of Spinal Atypical (World Health Organiza- tion Grade II) Meningiomas is Associated With Symptom Resolution and Low Recurrence. Neurosurgery. 2015 Jun;
76:739-46. DOI: 10.1227/neu.0000000000000720.
23. Han B, Zhang L, Jia W, et al. Clinical features and surgi- cal outcomes of high-grade spinal meningiomas: Report of 19 cases and literature review. J Clin Neurosci. 2020 Feb;
72:264-9. DOI: 10.1016/j.jocn.2019.11.020.
24. Ye J, Lv G, Qian J, et al. Clinical features and prognostic factors of WHO II and III adult spinal meningiomas: anal- ysis of 25 cases in a single center. J Neurooncol. 2016 Jun;
128:349-56. DOI: 10.1007/s11060-016-2119-8.
25. Vold
ř
ich R, Netuka D, Beneš
V. Spinal meningiomas: is Simpson grade II resection radical enough? Acta Neurochir (Wien). 2020 Jun;162:1401-8. DOI: 10.1007/s00701- 020-04280-2.26. Adeberg S, Hartmann C, Welzel T, et al. Long-term out- come after radiotherapy in patients with atypical and ma- lignant meningiomas-clinical results in 85 patients treated in a single institution leading to optimized guidelines for early radiation therapy. Int J Radiat Oncol Biol Phys. 2012 Jul 1;83:859-64. DOI: 10.1016/j.ijrobp.2011.08.010.
27. Kaur G, Sayegh ET, Larson A, et al. Adjuvant radiotherapy for atypical and malignant meningiomas: a systematic re- view. Neuro Oncol. 2014 May;16:628-36. DOI: 10.1093/
neuonc/nou025.
28. Yolcu YU, Goyal A, Alvi MA, et al. Trends in the utilization of radiotherapy for spinal meningiomas: insights from the 2004-2015 National Cancer Database. Neurosurg Focus.
2019 Jun 1;46:E6. DOI: 10.3171/2019.3.Focus1969.
29. Reddy AK, Ryoo JS, Denyer S, et al. Determining the role of adjuvant radiotherapy in the management of meningioma: a Surveillance, Epidemiology, and End Results analysis. Neu- rosurg Focus. 2019 Jun 1;46:E3. DOI: 10.3171/2019.3.Fo- cus1971.
30. Poulen G, Vignes JR, Le Corre M, et al. WHO grade II me- ningioma: Epidemiology, survival and contribution of post- operative radiotherapy in a multicenter cohort of 88 pa- tients. Neurochirurgie. 2020 Apr;66:73-9. DOI: 10.1016/
j.neuchi.2019.12.008.
31. Nabors LB, Portnow J, Ahluwalia M, et al. Central Nervous System Cancers, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2020 Nov 2;18:1537-70. DOI: 10.6004/jnccn.2020.0052.
32. Goldbrunner R, Minniti G, Preusser M, et al. EANO guidelines for the diagnosis and treatment of meningio- mas. Lancet Oncol. 2016 Sep;17:e383-91. DOI: 10.1016/
s1470-2045(16)30321-7.
33. Zhang H, Ma L, Shu C, et al. Spinal Clear Cell Menin- giomas: Clinical Features and Factors Predicting Recur- rence. World Neurosurg. 2020 Feb;134:e1062-e76. DOI:
10.1016/j.wneu.2019.11.093.
34. Wright JM, Wright CH, Cioffi G, et al. Survival in Patients with High-Grade Spinal Meningioma: An Analysis of the National Cancer Database. World Neurosurg. 2019 Sep;129:e749-e53. DOI: 10.1016/j.wneu.2019.06.015.
고등급 척추 수막종의 특징 및 치료
김영훈 • 김상일 • 박형열* • 김훈철 • 조창희 • 김종민
가톨릭대학교 서울성모병원 정형외과학교실, 가톨릭대학교 은평성모병원 정형외과학교실* 연구계획: 문헌고찰
목적: 고등급의 척추 수막종에 대한 역학, 치료, 그리고 예후에 대해 분석하고 현재 치료법의 한계와 이를 극복하기 위하여 시도되고 있는 방법에 대 해 보고하고자 한다.
선행 연구문헌의 요약: 척추 수막종은 WHO의 조직학적 분류법에 따라 3등급으로 나뉘는데, 대부분의 척추 수막종은 1등급으로 양성의 성질을 보이 지만, 소수에서는 생물학적으로 공격적인 특징을 보여 예후가 불량한 것으로 알려져 있다. 고등급의 척추 수막종의 가장 중요한 치료는 수술적 전절 제이지만, 아직까지 대단위 연구가 부족한 실정이다.
대상 및 방법: 관련 연구 고찰
결과: 고등급의 척추 수막종은 1등급의 수막종보다 전절제를 시행하였더라도 재발률이 높고 생존율도 떨어진다고 보고되었다. 재발을 막기 위해 가 장 중요한 것은 수술적 전절제이다. 전아전절제를 하였거나 3등급의 수막종일 경우 수술 후 방사선 치료를 시행할 수 있지만 그 실효성에 대해서는 아직 논란이 있다. 고등급의 수막종에서는 전이를 하기도 하며, 수술적 치료나 방사선 치료가 불가능할 경우에는 전신치료를 시도해볼 수 있지만 아 직까지 효과적인 약제는 없다. 수막종과 관련된 유전자 연구도 활발하며, 면역 체계와의 관련성도 제시되어 면역 치료에 대한 임상연구도 진행 중에 있다.
결론: 고등급 척추 수막종은 매우 드문 종양으로 예후가 불량하다고 알려져 있다. 적절한 초기 치료가 중요하며 수술적 전절제를 얻는 것이 중요하 며, 수술 후 방사선 치료를 시행하는 경우가 있다. 아직까지 고등급의 척추 수막종에 대한 치료의 가이드라인이 충분한 근거를 바탕으로 제시되지는 않았으며, 따라서 앞으로 대단위 무작위 임상 시험 등의 후속 연구가 필요하겠다.
색인 단어: 척추, 수막종, 비정형, 악성, 치료 약칭 제목: 비정형 척추 수막종의 특징 및 치료
접수일: 2021년 2월 2일 수정일: 2021년 2월 22일 게재확정일: 2021년 5월 14일 교신저자: 김상일
서울시 서초구 반포대로 222 가톨릭대학교 서울성모병원 정형외과학교실
TEL: 02-2258-6775 FAX: 02-535-9837 E-mail: [email protected]