1125
Treatment in Pediatric Renal Trauma: A Conservative Management Approach
Young Ho In, Ji Hyeong Yu, Luck Hee Sung, Choong Hee Noh, Jae Yong Chung
From the Department of Urology, College of Medicine, Inje University, Seoul, Korea
Purpose: The management of pediatric trauma is substantially derived from the results of adult trauma patient. Despite the increasing of pediatric renal trauma, the management of them still remains controversial. The aim of this study is to evaluate our experience with the expectant con- servative management of blunt trauma in children.
Materials and Methods: We retrospectively studied 45 pediatric patients with renal trauma between 1995 and 2007. We reviewed medical records for clinical symptoms, mechanism of injury, assigned grade of renal injury, associated injuries, indication of surgery, and treatment outcomes. We graded renal injuries according to the American Association for the Surgery of Trauma Organ Injury Scale.
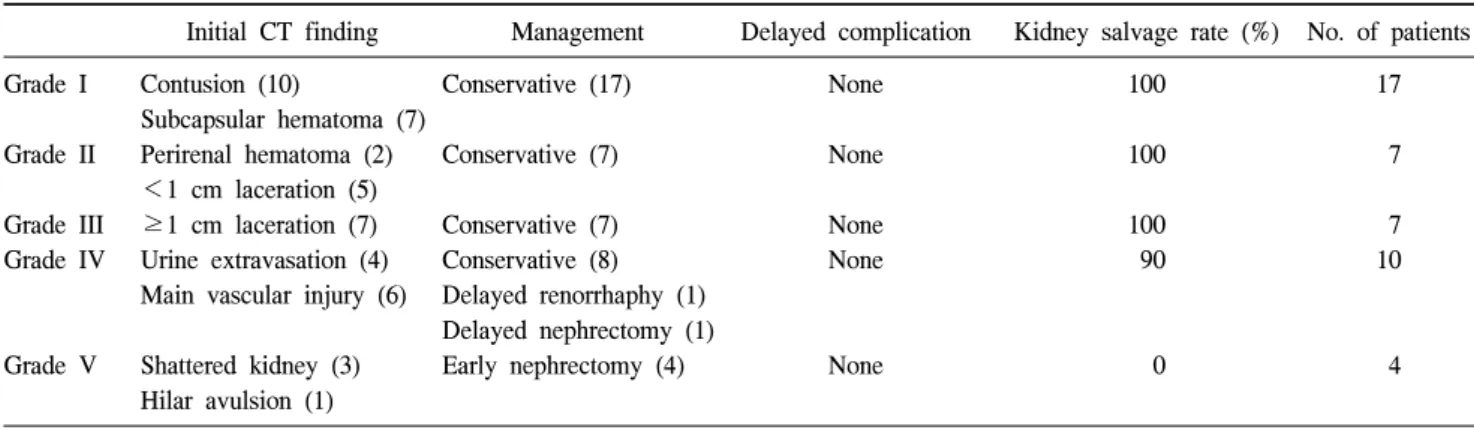
Results: All patients of grade I, II, III, and IV were managed conser- vatively at beginning, if the hemodynamic state is stable. Among them, 2 patients of grade IV were done delayed operation. One patient underwent delayed renorrhaphy for persistent anemia and hypotension, and the other patient needed delayed nephrectomy because of persistent fever and worsening abdominal pain with significant urinary extrava- sation. All patients of grade V were undergone early nephrectomy.
Conclusions: Except for persistent fever with significant extravasation and grade Ⅴ injury, initial conservative management of blunt renal trauma in children is effective and recommendable at beginning, if the hemo- dynamic state is stable. Prospective larger randomized controlled trials will be needed. (Korean J Urol 2009;50:1125-1132)
Key Words: Pediatrics, Kidney, Injuries, Treatment outcome
Korean Journal of Urology Vol. 50 No. 11: 1125-1132, November 2009
DOI: 10.4111/kju.2009.50.11.1125
인제대학교 의과대학 비뇨기과학교실 인영호ㆍ유지형ㆍ성락희
노충희ㆍ정재용
Received:June 8, 2009 Accepted:October 12, 2009 Correspondence to: Jae Yong Chung
Department of Urology, Sanggye Paik Hospital, Inje University, 761-1, Sanggye-dong, Nowon-gu, Seoul 139-707, Korea
TEL: 02-950-1137 FAX: 02-933-6133
E-mail: [email protected]
Ⓒ The Korean Urological Association, 2009
서 론
2008년 미국 내 보고에 의하면, 손상은 소아 사망에 이르 게 하는 원인 중 약 59.5%를 차지하며 [1], 국내의 한 연구 보고에서는 소아의 응급실 내원 후 사망 원인을 보면 사고 에 의한 원인이 41.8%로 가장 많았다 [2]. 이처럼 소아 손상 에서 교통사고가 많은 비중을 차지하며, 보행자 사고는 5-9 세에 호발하고, 남아에서 여아보다 2배 더 많다. 비뇨생식 기 손상으로 사망에 이르는 경우는 매우 드물지만, 소아에 서 비뇨생식기계 손상은 중추신경계 다음으로 외상이 잘 일어나는 호발 부위이다 [3]. 지금까지는 이러한 소아 신손
상의 경우도 성인의 치료 경험에 기초하고 있으나, 성인과 다른 해부학적, 생리학적 특수성과 선천성 기형이 있는 경 우에는 더 쉽게 손상을 받을 수 있는 점을 고려하였을 때, 아직도 진단 방법과 치료 방법에서 보존적 치료와 조기 수 술적 치료 사이에 논란의 여지가 있어 [4], 본원에서의 경험 을 분석하여 소아 신손상의 보존적 치료의 안전성과 보존 적 치료에 실패한 경우에 대하여 알아보고자 하였다.
대상 및 방법
1995년 1월부터 2007년까지 둔상성 신손상으로 본원에서 치료를 받은 45명의 소아 환자를 대상으로 하였으며, 의무
Table 1. Characteristics and mechanism of injury Mechanism of injury No. of patients Total No. of patients
Male:Female Mean age
Mechanism of injury
Pedestrian traffic accident (%) Fall (%)
Slip down (%) Others (%)
45 32:13 11.0±5.2 14 (31.1) 11 (24.4) 10 (22.2) 10 (22.2)
Table 2. Clinical manifestation on initial assessment
Clinical manifestation No. of patients (%)
Flank pain 35 (77.7)
Abdominal pain 5 (11.1)
Gross hematuria 27 (60.0)
Microscopic hematuria 34 (75.5)
Nausea/Vomiting 2 (4.4)
Decreased mentality (shock state)a 4 (8.8)
a: defined to any score below 27 of mini-mental state examination
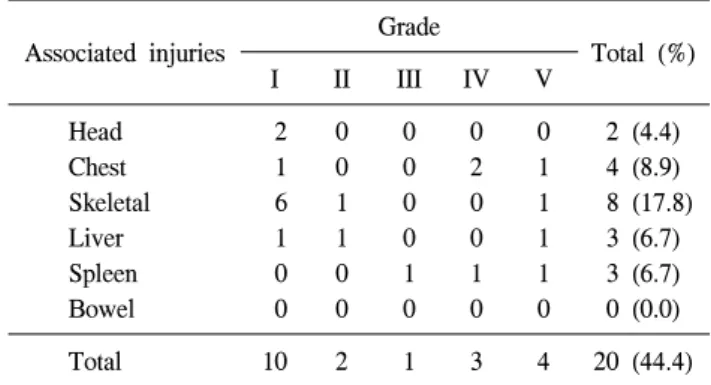
Table 3. Associated extrarenal injuries (n=20) Associated injuries Grade
Total (%)
I II III IV V
Head 2 0 0 0 0 2 (4.4)
Chest 1 0 0 2 1 4 (8.9)
Skeletal 6 1 0 0 1 8 (17.8)
Liver 1 1 0 0 1 3 (6.7)
Spleen 0 0 1 1 1 3 (6.7)
Bowel 0 0 0 0 0 0 (0.0)
Total 10 2 1 3 4 20 (44.4)
였다. 대부분의 경우에 보존적 치료는 예방적 항생제 투여 와 함께 육안적 혈뇨가 없어질 때가지 침상 안정을 취하도 록 하였고, 활력징후와 요량의 근접 관찰, 주기적인 복부 신 체검사와 혈색소 측정을 시행하였다. 입원 4-5일까지는 혈 색소, 혈청 전해질 및 크레아티닌을 매일 검사하였으며, 손 상의 정도가 비활력 분절을 동반한 grade III와 grade IV 이 상의 경우에는 손상 1-2주 이후 전산화단층촬영을 추적 검 사하여 초기의 손상 정도와 비교하여 확인하였다. 대부분 의 환아에서 퇴원 후 신손상의 회복과 신기능의 평가를 위 해 혈색소 수치와 크레아티닌을 시행하였고, 3개월째 전산 화단층촬영을 시행하여 초기의 소견과 비교하였다. 조기 수술적 치료는 초기 진단 후 24시간 이내로 규정하였고, 신 손상으로 인한 합병증을 초기와 지연성으로 구분하여 조사 하였다.
결 과
45명의 대상 환아는 남아 32명, 여아 13명으로 평균 추적 기간은 10.8±5.4개월, 평균 연령은 11.0±5.2세였다. 신손상 기전으로는 교통사고 14명 (31.1%), 추락 11명 (24.4%) 순으 로 많은 비율을 차지하였고 (Table 1), 초기 증상으로는 옆 구리 통증이 35명 (77.7%)으로 가장 많이 나타났으며, 육안
지 않아 보존적 치료를 지속할 수 있었다.
그러나 grade IV에 해당하는 4세 남아 1명 (Fig. 1)은 수혈 및 보존적 치료에도 지속적인 출혈과 활력 징후의 불안정 으로 손상 후 3일째 지연 수술을 시행하였으며, 괴사된 부 분의 제거와 남아 있는 신 분절의 봉합을 통한 신구제술을 시행하였다. 또한 초기 요누출 소견을 보인 grade IV 환아 4명 (60%) 중 3명은 요누출로 인한 일시적 발열이 있었으 나, 보존적 치료만으로 호전되고, 손상 후 단기 전산화단층 촬영 소견에서도 요누출이 소실되어 요관 부목이나 신루설 치술 등의 중재적 시술 없이도 보존적 치료를 지속할 수 있었다. 그러나 나머지 1명의 환아는 초기에 보존적 치료를 시작하였으나 복막뒤 공간 내 요누출의 증가로 인한 발열
Fig. 2. Eight-year-old child with blunt renal trauma. (A, B) On ad- mission, computerized tomography (CT) shows perinephric extravasa- tion of contrast media from left up- per collecting system. (C) Follow-up sonography 4 weeks later presents new developed hydronephrosis and increased perinephric urinoma. (D) Diethylenetriaminepentaacetic acid (DTPA) lasix renal scan image 5 weeks after injury shows relative delay in clearance from the left kid- ney and demonstrates relatively de- creased renal function. (E) At 7 weeks after injury, ureteral stenting was done. (F) CT shows infarction of left kidney just before nephrectomy.
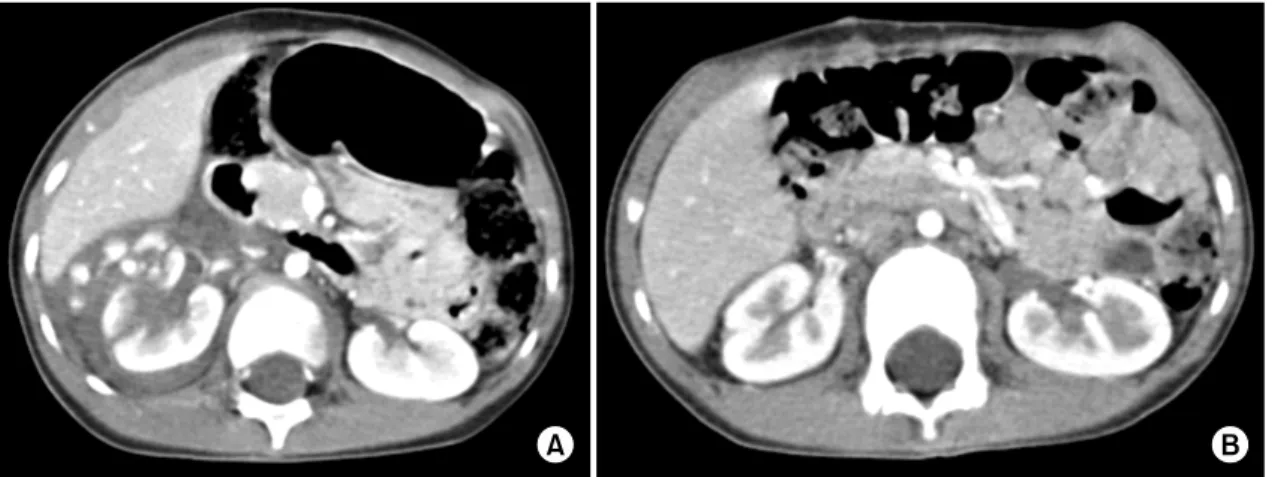
Fig. 1. Radiographic appearance of grade IV right renal injury in a 4-year-old child whose conservative treatment was failed. (A) Computerized tomography (CT) presents deep lacerations with main vascular injury of right kidney. (B) CT shows well healed kidney after 3 months from renorrhaphy.
Table 5. Complication of the initial conservative treatment
Complications No. of patients
Transfusion
Hypotension due to persistent hemorrhage Transient fever
Fever due to persistent urine leakage Death
6
1 (delayed renorrhaphy) 3
1 (delayed nephrectomy) 0
Total 11 (26.8%)
이 지속되며, 수신증이 발생하여 요관부목 삽입술의 시술 을 시행하였음에도 불구하고 활력징후가 불안정해지고, 복 부 통증 및 신경색으로 인하여 손상 후 8주째 지연 신적출 술을 시행하였다 (Fig. 2). 결국 초기 보존적 치료를 시행하 기로 결정한 41명 중 2명의 환아에서 신봉합술의 신구제술 과 신적출술의 지연 수술이 필요하였고, 전체적으로 보았 을 때 40명 (97.6%)의 대부분의 환자에서 보존적 치료의 지 속 및 지연적 신구제술을 통하여 신장의 보존이 가능하였 다 (Table 4). 보존적 치료의 초기 합병증이 발생한 환아는 11명 (26.8%)으로 6명 (grade III: 2명, grade IV: 4명)에서 수 혈이 필요할 정도의 경한 출혈과, 활력징후를 악화시킬 정 도의 지속적인 출혈 (grade IV: 1명) 및 일시적인 발열, 그리 고 요 누출로 인한 지속적인 발열 (grade IV: 1명)이 있었다 (Table 5). 특히 grade IV 10명 중 8명 (80%)에서 초기 보존적 치료만으로 증상이 호전되고 큰 합병증 없이 퇴원 가능하 였다.
Grade V에 해당하는 4명의 환아는 내원 당시 모두 불안 정한 활력 징후와 동반된 타 장기 손상으로, 조기 수술을 시행하였으며, 3명은 조기 신적출술을 시행하였고 (Fig. 3), 1명은 조기 신적출술을 시행하였으나 타 장기 손상으로 인 한 혈흉과 동반된 패혈증으로 결국 사망하였다.
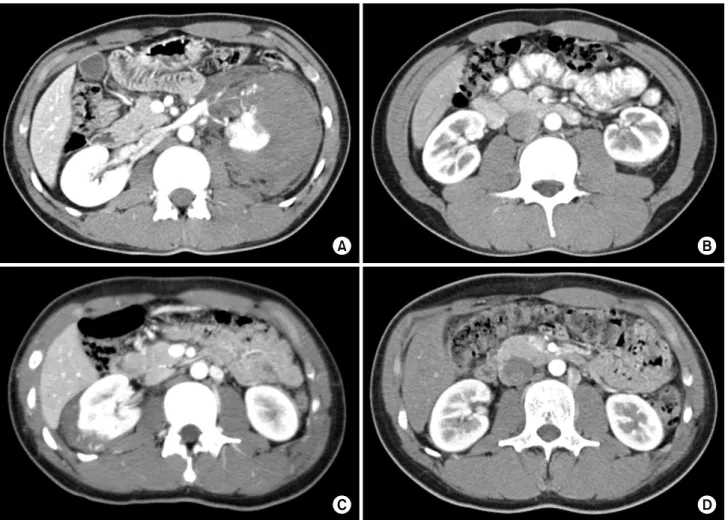
신손상의 호전 정도는 3-6개월 후 grade II, III의 일부 환 아와 지연 신절제술을 시행한 환아를 제외한 grade IV의 모
든 환아에서 전산화단층촬영을 추적 검사하여 확인하였다.
호전의 정도를 정량적으로 정확하게 파악할 수는 없었지 만, grade II와 III 환아에서는 4주 이내 대부분의 혈종의 크 기와 신실질 열상이 호전되는 양상을 보였고, grade IV의 환아는 혈종의 감소 정도가 grade II, III 손상에 비해 더 오 래 지속되었지만 3개월 이내 대부분의 혈종이 흡수되고 신 실질 열상이 호전되는 양상을 보였다 (Fig. 4). 그러나 본 연 구에서는 요누출이 지속되거나 신주위 농양소견을 보이는 경우는 없었다.
본 연구에서는 1년 이상 추적 관찰이 가능하였던 주로 grade III 이상의 15명 환아 모두에서 수신증, 결석 형성, 고 혈압, 신주위 농양 등의 지연 합병증이 발생한 경우는 없었 다.
고 찰
신장은 복부뿐 아니라 비뇨생식계에서도 가장 호발하는 손상 부위이다. 대부분 흉부, 척추, 골반 및 복강 내 장기 손상과 동반되며 [6], 특히 소아의 경우는 성인과 달리, 미 숙하고 약한 흉강과 근육, 적은 신주위 지방, 낮은 신장의 위치로 인해 손상의 이환율이 높고 [7], 손상의 원인이 추락 사고에 의한 경우가 많아 중증 신손상의 빈도가 높다 [8].
본 연구에서는 교통사고에 의한 경우가 11명으로 가장 많 았으며, 남녀 비에서는 본 연구에서와 마찬가지로 남아에 서 빈도가 높다. 그러나 실제로 성인보다 발생률이 높은지 에 대한 논쟁의 여지도 있다. 신손상은 대체로 둔상성과 관 통성 손상으로 분류되고, 전자는 소아 신손상의 90% 이상 의 원인에 해당한다 [9]. 대부분의 둔상성 신손상은 타박상 이며 적극적인 치료를 필요로 하지 않고 [10,11], 관통성 손 상은 성인보다 매우 드물며, 본 연구의 경우도 모두 둔상성 손상에 해당하였다.
소아는 성인 신손상 환자의 컴퓨터단층촬영과 비교하였
Fig. 4. The durations of improvement was longer in the higher grade injury comparing the lower grade one in follow-up images. (A, B) Parenchymal lacerations and amount of hematoma were resolved in 3 months after grade IV injury. (C, D) Perirenal hematoma was resolved completely in 4 weeks after grade III injury.
Fig. 3. Computerized tomography (CT) scan showing a grade V traumatic injury of left kidney each other. (A) 14-year-old boy, (B) 6-year-girl, transverse section image showing the shattered renal parenchyma of mid pole kidney. Early nephrectomy was required in all patients.
이는 소아 신손상의 경우 혈뇨의 유무만으로 방사선 검사 의 필요성을 판단해서는 안됨을 보고한 것이며, 이번 연구 에서는 60.0%에서 육안적 혈뇨의 증상이 있었다. 또한 2004 년 Santucci 등은 육안적 혈뇨에만 의지하지 않고, 혈류역학 적 상태, 감속성 손상기전, 타장기의 동반 손상 유무을 고려 하는 방사선적 평가의 적응증을 제시하기도 하였는데, 소 아의 경우에는 신손상의 의심되면 반드시 방사선학적 검사 를 시행할 것을 주장하고 있다 [14].
소아 신손상의 치료는 크게 보존적 치료와 조기 수술적 치료가 있으며, 여러 연구를 보았을 때 신적출술의 빈도가 보존적 치료 시보다 조기 수술적 치료 시에 더 높았다 [15,16]. 이는 제로타 근막의 탐포네이드 효과가 출혈을 방 지하는 것으로 생각되며, 수술적 치료 시 제로타근막이 파 열되면서 신적출술을 필요로 하는 확률이 높아지는 것으로 예상된다. 최근에는 혈류역학적 안정성, 방사선적 정확한 단계, 그리고 동반된 타장기 손상에 근거하여 수술적 치료 를 고려한다고 보고하고 있으나, 아직 명확한 치료방침에 대한 논쟁이 있어 본 연구의 목적과 부합된다고 할 수 있다.
신손상에 의한 혈류역학적 불안정 시, 박동성의 후복막 혈종의 증가, 혈관 경색술에도 불구하고 지속적인 출혈 시 에는 수술적 치료의 절대적 적응증이 되며, 방사선적 검사 에서 손상의 정도가 모호한 경우, 타장기 손상을 동반한 grade III 이상의 손상 시에도 개복술을 고려할 수 있다고 하였다 [17,18]. 이때 시험적 개복술이나 신봉합술의 구제적 수술이 선호되나, 다장기 손상이나 구제술이 불가능한 경 우 신적출술을 시행한다. 1983년 Cass와 Luxenberg는 grade IV, V의 중등도 손상에서 초기 보존적 치료에 실패하여 신 적출술을 시행한 경우와 조기 수술한 경우를 비교하였고, 다발성 손상을 동반한 신손상 환자의 73%에서 결국 수술적 치료가 필요함을 보고하여, 조기 수술적 치료가 이환율, 재 원 일수, 고혈압 등의 합병증을 줄인다고 하였다 [19]. 최근 에는 Santucci 등이 비록 소아에게만 국한된 경우는 아니지 만 the American Association for the Surgery of Trauma Organ
에도 하부요관이 온전한 경우 보존적 치료의 금기가 될 수 없고, 혈관 조영술 및 내시경적 혹은 경피적 시술을 시도 할 수 있다고 보고하였다 [22,23]. 이러한 결과로 Heyns 등 과 그 외 여러 연구자들은 grade III, IV에 국한된 손상 환자 에서 94%가 수술적 치료를 피할 수 있었다고 보고하였고 [17,18,21,24], 국내에서는 Joung 등이 초기 보존적 치료를 시작하였던 환자의 94.6%가 추가적 시술없이 치료의 성공 이 가능하였다고 보고하였다 [25]. 최근 Buckley와 Mc- Aninch는 327명의 둔상성 소아 신손상의 결과에서 98.2%의 보존적 치료 성공률을 보고하였고, 이는 86.7%에서 수술적 치료를 요하지 않았던 본원의 경우와도 비슷한 결과이다 [6]. 또한 Altman 등은 grade V에서도 보존적 치료의 가능성 을 제시하기도 하였다 [26].
보존적 치료 시에는 침상 안정, 활력 징후와 요 배출량의 근접관찰, 주기적인 복부 신체검사 및 헤모글로빈 검사를 시행해야 하며, 필요한 경우는 수혈을 시행할 수 있다 [17,18]. 관통성 손상의 경우에는 상처의 오염을 방지하기 위하여, 둔상성 손상의 경우에는, 다량의 후복막혈종 혹은 요누출이 있는 경우, 합병증 방지를 위하여 항생제 치료를 고려할 수 있다 [6,18,24,27]. Wessells 등은 보존적 치료를 시행한 모든 grade IV, V와 비 활력 분절을 동반한 grade III 환자는 손상 2-3일 후, 그리고 혈류역학적으로 불안정해지 거나, 수혈과 혈관 경색술에도 불구하고 지속적인 헤모글 로빈 감소 시에 전산화단층촬영 재시행의 필요성을 주장하 였고, 보행은 육안적 혈뇨가 소실되면 가능하고, 격렬한 운 동은 최소 6주 동안 피해야 한다고 하였다 [24].
신손상 후 발생하는 고혈압은 신동맥 폐쇄, 동정맥 기형 및 혈종의 신실질의 압박으로 인한 신허혈이 가장 큰 원인 이며, 손상 후 신기능이 20% 미만으로 감소되고 전체 신장 의 반흔형성의 소견이 보이면 신적출술을 고려할 수 있다.
본 연구에서 이러한 합병증이 발생한 환아는 없었다.
결 론
저자들은 신손상의 정도가 grade I부터 III까지는 활력징 후가 안정되어 초기에 보존적 치료가 가능하였다. Grade IV 의 경우에도 지속적인 요 누출을 동반한 심한 발열이 나는 경우를 제외한다면, 초기에 보존적 치료가 시도가 가능하 여 신손상의 보존적 치료 접근이 신장 보존과 합병증의 최 소화 측면에서 안전하고 타당한 치료법으로 생각한다. 하 지만 활력징후가 안정적일지라도 지속적인 출혈 소견이 보 이며, 요누출로 인한 증상이 호전되지 않는다면 적극적으 로 전산화단층촬영과 같은 검사를 시행하고 빨리 개복 수 술을 고려하는 것이 나을 것으로 생각한다. Grade V의 경우 에는 초기에 보존적 치료를 고려하기보다는 처음부터 적극 적으로 조기 수술을 고려하는 것이 환자의 예후에 좋을 것 으로 판단되고, 타장기의 손상이 심하게 동반되었다면 적 극적으로 타과와의 협진 수술을 시행하는 것이 환자의 예 후에 도움이 될 것으로 생각한다.
REFERENCES
1. American Academy of Pediatrics Section on Orthopaedics, American Academy of Pediatrics Committee on Pediatric Emergency Medicine, American Academy of Pediatrics Sec- tion on Critical Care, American Academy of Pediatrics Section on Surgery, American Academy of Pediatrics Section on Transport Medicine, American Academy of Pediatrics Co- mmittee on Pediatric Emergency Medicine, et al. Management of pediatric trauma. Pediatrics 2008;121:849-54.
2. Kim DH, Lee SH, Lee SB, Ryu MH, Lee DJ. Clinical analysis of pediatric death patients visiting emergency center. Korean J Pediatr 2004;47:12-7.
3. Livne PM, Gonzales ET Jr. Genitourinary trauma in children.
Urol Clin North Am 1985;12:53-65.
4. Wessel LM, Scholz S, Jester I, Arnold R, Lorenz C, Hosie S, et al. Management of kidney injuries in children with blunt abdominal trauma. J Pediatr Surg 2000;35:1326-30.
5. Moore EE, Shackford SR, Pachter HL, McAninch JW, Brow- ner BD, Champion HR, et al. Organ injury scaling: spleen, liver, and kidney. J Truma 1989;29:1664-6.
6. Buckley JC, McAninch JW. Pediatric renal injuries: mana- gement guidelines from a 25-year experience. J Urol 2004;
172:687-90.
7. Brown SL, Elder JS, Spirnak JP. Are pediatric patients more susceptible to major renal injury from blunt trauma? A comparative study. J Urol 1998;160:138-40.
8. Lee JH, Yoon SJ, Lee JB. Comparison of blunt renal injury between children and adults: effect of the causes on severity
of renal injury. Korean J Urol 2005;46:32-6.
9. Sahin H, Akay AF, Yilmaz G, Tacyildiz IH, Bircan MK.
Retrospective analysis of 135 renal trauma cases. Int J Urol 2004;11:332-6.
10. Miller KS, McAninch JW. Radiographic assessment of renal trauma: our 15-year experience. J Urol 1995;154:352-5.
11. Morse TS. Renal injuries. Pediatr Clin North Am 1975;22:
379-91.
12. Chopra P, St-Vil D, Yazbeck S. Blunt renal trauma-blessing in disguise? J Pediatr Surg 2002;37:779-82.
13. Morey AF, Bruce JE, McAninch JW. Efficacy of radiographic imaging in pediatric blunt renal trauma. J Urol 1996;156:
2014-8.
14. Santucci RA, Langenburg SE, Zachareas MJ. Traumatic hema- turia in children can be evaluated as in adults. J Urol 2004;
171:822-5.
15. Hammer CC, Santucci RA. Effect of an institutional policy of nonoperative treatment of grade I to IV renal injuries. J Urol 2003;169:1751-3.
16. Keller MS, Eric Coln C, Garza JJ, Sartorelli KH, Christine Green M, Weber TR. Functional outcome of nonoperatively managed renal injuries in children. J Trauma 2004;57:108-10.
17. Heyns CF. Renal trauma: indications for imaging and surgical exploration. BJU Int 2004;93:1165-70.
18. Santucci RA, Wessells H, Bartsch G, Descotes J, Heyns CF, McAninch JW, et al. Evaluation and management of renal injuries: consensus statement of the renal trauma subco- mmittee. BJU Int 2004;93:937-54.
19. Cass AS, Luxenberg M. Conservative or immediate surgical management of blunt renal injuries. J Urol 1983;130:11-6.
20. Santucci RA, McAninch JW, Safir M, Mario LA, Service S, Segal MR. Validation of the American Association for the Surgery of Trauma organ injury severity scale for the kidney.
J Trauma 2001;50:195-200.
21. Husmann DA, Gilling PJ, Perry MO, Morris JS, Boone TB.
Major renal lacerations with a devitalized fragment following blunt abdominal trauma: a comparison between nonoperative (expectant) versus surgical management. J Urol 1993;150:
1774-7.
22. Russell RS, Gomelsky A, McMahon DR, Andrews D, Nasra- llah PF. Management of grade IV renal injury in children. J Urol 2001;166:1049-50.
23. Rogers CG, Knight V, MacUra KJ, Ziegfeld S, Paidas CN, Mathews RI. High-grade renal injuries in children-is conser- vative management possible? Urology 2004;64:574-9.
24. Wessells H, McAninch JW, Meyer A, Bruce J. Criteria for nonoperative treatment of significant penetrating renal lace- rations. J Urol 1997;157:24-7.
25. Joung JY, Park SC, Kim JB, Kim HK, Park JY, Cheon SH, et al. Comparison of operative versus conservative manage- ment in pediatric renal trauma. Korean J Urol 2005;46:124-30.
26. Altman AL, Haas C, Dinchman KH, Spirnak JP. Selective