접수일: 2011년 1월 14일, 게재승인일: 2011년 3월 28일 책임저자: 김태형, 부산시 서구 동대신동3가 1
602-715, 동아대학교 동아대학교병원 재활의학과
Tel: 051-240-5690, Fax: 051-254-8511 E-mail: [email protected]
동결견 환자의 관절낭 팽창술 시 도수조작의 부가적 효과
동아대학병원 재활의학과
김상범ㆍ이경우ㆍ이종화ㆍ김태형ㆍ한동욱
The Additional Effect of Manipulation af- ter Arthrographic Capsular Distension in Frozen Shoulder
Sang Beom Kim, M.D., Kyeong Woo Lee, M.D., Jong Hwa Lee, M.D., Tae Hyoung Kim, M.D. and Dong Wook Han, M.D.
Department of Physical Medicine and Rehabilitation, Dong-A University College of Medicine, Busan, Korea
Objective: To evaluate the additive effect of manipulation after arthrographic capsular distension in patients with fro- zen shoulder. Materials and Methods: Seventy three pa- tients who had clinically diagnosed as frozen shoulder were enrolled. We treated thirty nine patients (control group) with arthrographic capsular distension and thirty four patients (experimental group) were treated with manipulation therapy after arthrographic capsular distension. Arthrographic cap- sular distension was done by anterior shoulder approach technique. Manipulation was done at 5 minute after dis- tension in experimental group. The effect was evaluated by visual analogue pain scale and passive range of motion of shoulder (flexion, abduction, internal rotation and external rotation) before injection, 1 week after injection and 3 weeks after injection. Results: Visual analogue pain scale was decreased in both group. In comparison with control group, visual analogue pain scale of experimental group showed significant decrease at 1 week after injection (p
<0.05), but no difference at 3 weeks after injection in both group. Passive range of motion improved in both group.
Passive range of motion of experimental group showed sig- nificantly improved than control group in flexion, internal ro- tation and external rotation at 1 week after injection (p
<0.05), but 3 weeks later experimental group improved at only external rotation than control group (p<0.05).
Conclusion: The manipulation after arthrographic capsular distension in patients with frozen shoulder has additive ef- fect for reduction of pain and improvement of shoulder range of motion. (Clinical Pain 2011;10:50-54)
Key Words: Frozen shoulder, Arthrographic capsular distension, Manipulation
서 론
동결건은 주로 고령의 환자에서 흔히 발생되며 관절낭의 비후와 관절강의 용적의 감소로 인하여 서서히 진행되는 견관절의 통증과 관절의 가동운동범위의 제한이 발생하여, 여러 일상생활의 동작장애를 초래하게 된다.1,2) 일반적인 치료법으로 비스테로이드소염제의 경구 투여, 활액낭 스테 로이드 주사치료 외에 온열요법, 경피전기신경자극, 신장 운동 등의 물리치료가 시행되고 있다. 그러나 만성기 환자 에서는 위의 고식적인 방법에 의한 치료효과가 만족스럽지 못한 경우가 종종 있다. 이러한 경우 관절 조영술에 이은 관절낭 팽창술,3,4) 도수조작(manipulation)요법과 관절경수 술 등을 시행할 수 있다. 최근 Kim 등5)의 논문에서 관절낭 팽창술을 시행 후 수동관절운동의 도수조작을 시행하여 효 과적으로 관절낭의 파열이 됨을 보고하였다. 본 실험에서 동결견 환자에서 관절낭 팽창술 실시 후 수동적 도수조작 을 추가로 실시한 군을 실험군으로 하고, 관절 조영술을 통 한 관절낭 팽창술만을 실시한 군을 대조군으로 하여 두 군 간의 비교를 통해서 부가적인 수동적인 도수조작이 통증 감소 및 관절 가동 범위 증가에 추가적인 치료적 효과가 있는지 알아보고자 하였다.
연구대상 및 방법 1.
연구 대상
2008년 1월부터 2009년 6월까지 견관절 통증을 주소로 본원 재활의학과 외래를 통해 내원한 환자 중 이학적 검사 및 방사선 검사, 초음파 검사를 통해 동결견을 진단받은 환 자 73명을 대상으로 하였다.
전체 73명의 연구 대상자의 성별 분포는 대조군 여성 25 명, 남성 14명으로 총 39명이었으며, 실험군 여성 16명, 남 성 18명으로 총 34명이었으며, 각 군에서 통계학적 유의성 은 없었다(Table 1).
Table 1. General Characteristics of Patients
Characteristics Experimental group Control group Gender
Men 18 14
Women 16 25
Age (years)
<40 3 2
40∼60 14 11
60> 17 26
Lesion site (shoulder)
Left 12 16
Right 22 23
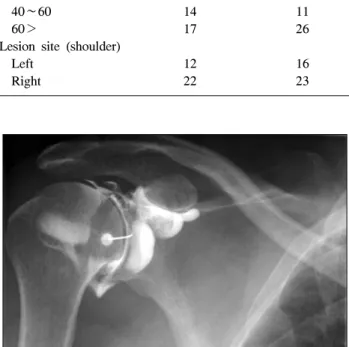
Fig. 1. Arthrography following injection of contrast material.
Both groups were received shoulder distension by anterior ap- proach shoulder radiography was taken after injection of 5 cc radiographic contrast.
Fig. 2. Manipulation after distension in experimental group.
Experimental group received shoulder manipulation (passive ROM manipulation) 5 minutes after shoulder distension.
Fig. 3. Shoulder arthrography after manipulation. The occur-
rence of capsular tear was observed after distended arthrography and passive range of motion manipulation.2.
연구 방법
1)
관절 조영술을 통한 관절낭 팽창술
: 관절낭 팽창술은Rizk 등6)이 시행한 Kaye-Schneider의 방법에 따라 환자를 X-선 튜브가 있는 투시대 위에 앙와위로 눕히고, 환자로 하 여금 환측 어깨부위를 이완시키도록 한 후 낮은 베개 등을 이용하여 건측 어깨 밑을 받혔다. 환측 견관절을 약 20o 외 회전시켜 상완와관절(glenohumeral joint)의 간격을 최대한 넓힌 상태에서, 상완와관절의 중간 및 하방 1/3 연접 부위 를 기준점으로 정하고 PovidineⓇ으로 소독하였다. 25-guage 주사기를 이용하여 1% Lidocaine으로 기준점을 국소마취 한 후, 21-gauge 11 cm spinal needle을 이용하여 X-선 투시 하에서 기준점에서 상완와관절 내를 향하여 수직방향으로 삽입하였다. 이때 주사침이 관절 내에 정확히 위치하였는 지를 판단하기 위하여 5 ml의 수용성 조영제 (UrograffinⓇ) 를 주사하여 투시기 모니터에서 관절이 초생달 모양으로
조영됨을 확인하였다(Fig. 1). 그 후 40 mg Triamcinolone, 1% Lidocane, Normal saline 그리고 Hyaluronic acid 혼합 용액 30 ml를 주입하였다. 시술 다음 날부터 모든 환자에 대하여, 3주간 Codman 운동, 손가락으로 벽을 집고 기어올 라가는 운동(finger wall climbing exercise), 어깨 신장 운동 등을 가정에서도 지속적으로 하루 1시간 이상 실시하도록 교육하였다.
2)
도수 조작
: 실험군에서는 수압 팽창술 시행 5분 후 관절낭의 파열유무와 관계없이 추가적으로 치료자가 전 관절 영역 관절운동을 수동적으로 시행하여 모든 환자에서 관절 낭의 파열을 확인하였다(Fig. 2). 관절낭의 파열 유무는 관 절낭 팽창파열술 시행 시 방사선 조영 사진으로 확인하였
Table 2. Comparison of the Effect on Visual Analogue Pain
ScaleBefore injection
1 week after injection
3 weeks after injection Experimental group 6.5±0.3 3.6±0.4 2.6±0.4
Control group 6.9±0.4 4.7±0.3 2.9±0.4
Values are mean±standard deviation.
Fig. 4. Comparisons of the mean VAS score at before treatment,
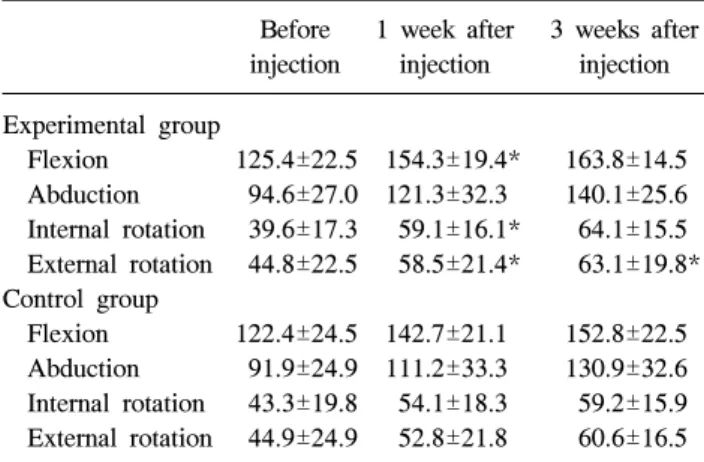
1 week after injection and 3 weeks after injection. Visual ana- logue scale of experimental group showed more decrease than 1 weeks after injection (*p<0.05), but no difference at 3 weeks after injection. VAS: visual analogue scale.Table 3. Mean Range of Motion in Before Injection, Injection
after 1 and 3 Weeks LaterBefore injection
1 week after injection
3 weeks after injection Experimental group
Flexion 125.4±22.5 154.3±19.4* 163.8±14.5 Abduction 94.6±27.0 121.3±32.3 140.1±25.6 Internal rotation 39.6±17.3 59.1±16.1* 64.1±15.5 External rotation 44.8±22.5 58.5±21.4* 63.1±19.8*
Control group
Flexion 122.4±24.5 142.7±21.1 152.8±22.5 Abduction 91.9±24.9 111.2±33.3 130.9±32.6 Internal rotation 43.3±19.8 54.1±18.3 59.2±15.9 External rotation 44.9±24.9 52.8±21.8 60.6±16.5 Values are mean±standard deviation. *Statically significant (p
<0.05) in comparison between Experimental group and control group.
고, 수동적 도수조작에 의한 관절낭의 파열유무는 수동 관 절 가동운동 후에 방사선 조영 사진으로 확인하였다(Fig. 3).
3)
효과 판정
: 치료효과 판정을 위해 시술 전과 각각의시술이 끝난 직후, 1주 후, 3주 후에 자가 설문지를 이용하 여 시각 상사 척도를 확인하였고, 검사자에 의해 견관절의 굴곡, 외전, 외회전, 내회전의 관절 가동 범위를 확인하였 다. 외전 및 굴곡 검사는 주관절을 신전시킨 상태에서 체간 의 뒤틀림 없이 해부학적 자세를 0o로 하여 운동범위를 0o 에서의 편향각도로 정하는 180o 방법을 이용하여 측정하였 고, 외회전 및 내회전 검사는 앙와위에서 견관절을 90o 외 전시키고 주관절을 90o 굴곡시킨 상태에서 180o 방법을 이 용하여 측정하였다. 이때 외전이 90o가 되지 않는 환자는 최대한의 외전상태에서 외회전과 내회전을 측정하였다.
통계분석은 윈도우용 SPSS version 15.0을 사용하였고 p<0.05를 통계적으로 유의한 수준으로 정하였다. 각 군내 에서 시술 전후, 1주 후, 2주 후의 효과 비교는 비모수적 방법인 Wilcoxon signed rank test로 분석하였고, 실험군과
대조군 간의 효과 비교는 비모수적인 방법인 Mann-Whit- ney test로 분석하였다.
결 과 1.
통증 변화
통증 변화를 나타내는 시각 상사 척도는 실험군과 대조 군 모두 치료 전에 비해 치료 후 감소한 것으로 나타났다.
두 군 간의 비교에서는 실험군이 대조군에 비해 치료 후 1주 뒤에 시각적 상사 척도가 통계학적으로 유의하게 감소 하였으나(p<0.05), 치료 후 3주 뒤에는 두 군 간에 유의한 차이를 볼 수 없었다(Table 2)(Fig. 4).
2.
능동 관절 운동범위의 변화
능동 관절 운동범위는 두 군에서 모두 치료 전에 비해 치료 후 능동 관절 운동범위가 증가하였다. 두 군 간의 비교 에서 치료 후 1주 뒤에 실험군이 대조군에 비해 굴곡, 내회 전, 외회전에서 통계학적으로 유의하게 증가하였으나(p
<0.05), 치료 후 3주 뒤에는 외회전 에서만 실험군이 대조 군 보다 유의한 능동 관절 운동범위의 증가를 보였다(p
<0.05)(Table 3).
고 찰
본 연구는 동결견 환자에게서 통상적 치료법인 관절 조 영술을 통한 관절낭 팽창술에 더하여 부가적으로 수동적 관절 가동운동을 실시하여, 관절낭을 파열시켰을 경우 추
가적인 통증 감소 및 관절 가동 범위 증가를 확인하기 위하 여 실시하였다.
동결견은 유착성 관절낭염이라고도 불리우며 임상적으 로 흔히 볼 수 있는 질환으로 점차적으로 증가하는 동통과 관절 가동 범위의 감소가 특징인 질환이다.7) 병리학적으로 관절낭의 변화는 종창, 섬유화 및 경도의 염증성 반응을 보 이며, 견관절의 활액막은 연골에 유착되며 관절 용적이 감 소되어, 심해지면 섬유성 유착, 회전근개의 결손, 뼈의 경화 와 낭종을 초래한다. 임상적 진행에 대해서는 1∼2년에 걸 쳐 자연적으로 치유된다는 보고와, 영구적인 증상과 장애 를 가질 수 있다는 보고가 있는 등 아직 논란이 있다.8,9) 통 상적인 치료방법으로는 비스테로이드성 소염제, 진통제, 온열요법 그리고 적극적인 물리치료 등이 사용되고 있으 나, 상기된 치료법만으로는 병의 치료 경과에 큰 변화를 주 지 못하며 주로 초기에 통증을 경감시킴으로써 관절운동범 위를 증가시켜 주는데 치료 목적이 있다.10-15) 염증의 치료 를 위한 효과적인 치료법으로 스테로이드의 관절낭내 주입 이 있으며, 질환의 초기에 매우 빠른 효과를 볼 수 있다.16) Hyaluronic acid (Sodium Hyaluronate)는 활액의 주성분인 glycosaminoglycan으로서 기계적 충격의 흡수, 관절 윤활 제, 관절 연골조직의 보전 역할을 하는데 임상적으로 변형 성 슬관절증과 견관절 주위염의 관절내 주사법을 시행함으 로써 동통 감소, 항염작용, 관절 가동 범위 증가, 연골조직 변성억제, 병적 관절액을 정상화시키는 효과를 보이는 것 으로 알려져 있으며,17,18) Kim 등19)의 연구에서 스테로이드 주사 시 발생할 수 있는 부작용을 줄이고 합병증을 가지고 있는 당뇨병환자에서 사용상의 이점이 밝혀져 있어 유용한 치료법으로 많이 사용되고 있다. 또한 즉각적이고 능동적 인 치료 방법으로서 관절조영술 후 수압 팽창술이나 관절 낭 팽창파열술(distension arthrography)이 시행되고 있 다.20) 수압 팽창술에서 증상의 호전을 보이는 기전은 다음 과 같다. 첫째, 관절낭의 파열과 관절강 내 공간의 팽창으로 유착부위를 줄여 관절낭 내 압력을 감소시킨다. 둘째 스테 로이드제의 투여로 병리학적 진행 과정에 있는 염증반응을 감소시켜 치료 효과를 낸다. 또 다른 치료법으로 Polking- horn21)의 연구와 Lee 등22)은 수동관절가동운동을 통하여 동결견에서 관절 가동역의 뚜렷한 증가와 통증의 지표인 시각상사척도의 감소가 나타나 수동관절가동운동 치료법 이 효과적이고 유용성이 있음을 발표하였다. 하지만 잘못 된 도수조작 방법이나, 너무 자주 반복된 도수조작이 섬유 성 유착의 발생이나 정상조직의 파열 및 반흔조직의 형성 등으로 강직성을 증가시킬 수 있어 주의를 요한다.
Von Royen과 Pavlov23)와, 최근 Kim 등5)의 논문에서 수 압 팽창술과 수동관절가동운동을 하여 완전한 관절낭의 파 열을 확인한 경우에도 관절범위 회복에 도움이 있음이 밝
혀졌으나 그 연구의 대상 수가 적은 단점이 있었다.
본 연구에서는 동결견 환자에서 수압 팽창술만을 실시한 군과 수압 팽창술과 더불어 수동관절가동운동의 도수조작 을 부가하여 완전한 관절낭의 파열을 확인한 군에서 도수 조작을 통한 관절낭의 파열이 어느 정도의 부가적인 치료 효과가 있는지를 확인하려 하였다.
견관절 팽창 파열술 후 관절 가동범위의 호전에 대하여 Park과 Hwang24)의 연구에서 굴곡, 내회전에 의미가 있게 증가하였다고 보고되었고, Choi 등4)의 연구에서는 굴곡, 외전, 외회전에서 의미가 있다고 보고되었다. 본 연구에서 도 시술 후 관절 가동 범위의 증가를 확인하였으며, 시술 후 1주 후에는 실험군에서 굴곡, 내회전, 외회전에서 대조 군에 비해 통계학적인 의미가 있게 증가하였다. 그러나 3주 후에는 실험군이 대조군에 비하여 외회전에서만 관절 운동 범위의 유의한 증가를 볼 수 있었다. 이는 Lee 등22)의 연구 에서 동결견의 특성인 관절 주위 근육 유착과 견관절 주변 의 연부조직 유착이 치료 초기에 완화되면서 관절가동역이 눈에 띄게 증가되지만, 이 치료만으로는 심부 구조 유착의 완전한 이완은 더 이상 기대할 수 없으므로 치료 후기에 관절 가동역의 변화가 덜 두드러지게 나타나는 것으로 생 각된다.
시각적 상사 척도에서는 시술 후 대조군에 비해 실험군 에서 시술 후 1주 후에 통계학적으로 유의하게 감소하였고 (p<0.05), 3주 후에는 두 군 간에 유의한 차이가 없었으나, 동결견 환자의 가장 큰 호소는 통증이라는 것을 고려하면 도수조작을 통한 관절낭의 파열이 초기 통증완화 및 관절 가동역 개선에 추가적인 도움이 있어 도수조작의 의미가 있는 것으로 사료된다.
본 실험의 단점으로 장기간의 관찰에 의한 결과가 없어 이에 관한 연구가 더 필요한 실정이며, 집에서의 추가적인 운동에 대한 개인적인 차이로 인하여 능동적 관절 가동 범 위의 차이와 시각상사 척도의 차이에 대하여 고려하지 못 한 점이 있으며 앞으로 이에 대한 연구가 더 필요할 것으로 사료된다.
결 론
동결견 환자에서 수압 팽창술만을 실시한 대조군과 수압 팽창술과 부가적인 도수 조작을 통한 관절낭 파열을 실시 한 실험군 모두 시술 후 통증 및 견관절 운동범위의 호전에 효과가 있었다. 대조군에 비해 실험군에서 단기적으로 통 증 및 견관절 운동범위의 호전에 유의할 만한 효과가 있었 다. 이후 두 군간의 3주간의 경과 관찰에서는 통증의 정도 는 두 군간의 유의할 만한 차이가 관찰되지 않았으나, 견관 절의 외회전 운동범위에 대하여 실험군이 대조군에 비하여
호전이 있어 관절낭 팽창술 후 부가적인 도수 조작이 동결 견 환자의 치료에 의미가 있는 치료법으로 사료된다.
참 고 문 헌
1. Anthon HA. Frozen shoulder. Can Fam Physician 1993;39:
1173-8.
2. Murnaghan JP. Adhesive capsulitis of the shoulder: current concepts and treatment. Orthopedics 1998;11:153-8.
3. Park SK, Nam MH, Yune SH. Hydraulic management of frozen shoulder. J Korean Acad Rehabil Med 1992;16:
147-53.
4. Choi ES, Kim JS, Lee YS, Shim BS, Ko YJ, Park SH.
Arthrographic findings of frozen shoulder and therapeutic effect of distension arthrography. J Korean Acad Rehabil Med 2001;25:278-83.
5. Kim JS, Kwon JY, Lee WI, Kim JM. The additional effect of tear after passive exercise during distension arthrogra- phy in patients with frozen shoulder. J Korean Acad Rehabil Med 2008;32:324-6.
6. Rizk TE, Gavant ML, Pinals RS. Treatment of adhesive capsulitis (Frozen shoulder) with arthrographic capsular dis- tension and rupture. Arch Phys Med Rehabil 1994;75:
803-7.
7. Neiaser JS. Adhesive capsulitis and the stiff and painful shoulder. Orthop Clin North Am 1980;11:327-31.
8. Ekelund AL, Rydell N. Combination treatment for adhesive capsulitis of the shoulder. Clin Orthop 1992;282:105-9.
9. Grubbs N. Frozen shoulder syndrome: a review of liter- ature. J Orthop Sports Phys Ther 1993;18:479-87.
10. Gavant ML, Rizk TE. Distention arthrography in the treat- ment of adhesive capsulitis of the shoulder. J Vasc Interv Radiol 1994;5:305-8.
11. Rizk TE, Gavant ML. Treatment of adhesive capsulitis (frozen shoulder) with arthrographic capsular distension and rupture. Arch Phys Med Rehabil 1983;64:803-7.
12. Sharma RK, Bajekal RA. Frozen shoulder syndrome; a comparison hydraulic distension and manipulation. Interna- tional Orthop (SICOT) 1993;17:275-8.
13. De Jong BA, Dahmen R, Hogemwg JA. Intraarticular tri- amcinolone- acetonide Injection in patients with capsulitis
of the shoulder. a comparative study of two dose regimens.
Clin Rehabil 1998;12:211-5.
14. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clinical study with an eval- uation of three treatment regimens. Ann Rheum Dis 1984;
43:353-60.
15. Dacre JE, Beeney N, Scott DL. Injections and physio- therapy for the painful stiff shoulder. Ann Rheum Dis 1989;
48:322-5.
16. Rizk TE, Pinals RS, Talaiver A. Corticosteroid injection in adhesive capsulitis: investigation of their value and site.
Arch Phys Med Rehabil 1991;72:20-2.
17. Yoshimi T, Kikuchi T. Effects of high-molecular-weight sodium hyaluronate on experimental osteoarthrosis induced by the resection of rabbit anterior cruciate ligament. Clin Orthop 1994;298:296-304.
18. Blaine T, Moskowitz R, Udell J, et al. Treatment of persis- tent shoulder pain with sodium hyaluronate: a randomized, controlled trial. A multicenter study. J Bone Joint Surg Am 2008;90:970-9.
19. Kim HW, Kim HS, Ahn KH. The effect of intraarthicular injection of hyaluronic acid and steroid in adhesive capsu- litis of shoulder. J Korean Acad Rehabil Med 1999;22:
117-23.
20. Vad VB, Sakalkale D, Warren RF. The role of capsular dis- tention in adhesive capsulitis. Arch phys Med Rehabil 2003;84:1290-2.
21. Polkinghorn BS. Chiropractic treatment of frozen shoulder syndrome (adhesive capsulitis) utilizing mechanical force, manually assisted short lever adjusting procedures. J Mani- pulative Physiol Ther 1995;158:105-15.
22. Lee KM, Lee KL, Han KS. Usefulness of manual medicine therapy in adhesive capsulitis of shoulder. J Korean Acad Rehabil Med 2000;24:784-92.
23. van Royen BJ, Pavlov PW. Treatment of frozen shoulder by distension and manipulation under local anaesthesia. Int Orthop 1996;20:207-10.
24. Park GY, Hwang SE. Comparison of intraarticular steroid injection with and without capsular distension in adhesive capsulitis of the shoulder. J Korean Acad Rehabil Med 2000;24:278-83.