접수일
: 2014년
11월
10일
,게재승인일
: 2015년
1월
5일 책임저자
:이상헌
,서울시 성북구 인촌로
73
136-705,고려대학교 안암병원 재활의학과
Tel: 02-920-6471, Fax: 02-929-9951 E-mail: [email protected]
급성 요추 추간판성 통증 환자에서 추간판내 스테로이드 주입술의 치료적 효과
예비연구
분당제생병원 재활의학과, 고려대학교 안암병원 재활의학과
1윤형석ㆍ김주섭ㆍ이상헌1
Therapeutic Effects of the Intradiscal Steroid Injection in Acute Lumbar Discogenic Pain
A Preliminary Study Hyeong Suk Yun, M.D., Joo Sup Kim, M.D., Ph.D.
and Sang Heon Lee, M.D., Ph.D.
1Department of Physical Medicine and Rehabilitation, Bundang Jesaeng General Hospital, Seongnam,
1Department of Physi- cal Medicine and Rehabilitation, Korea University College of Medicine, Seoul, Korea
Objective: The therapeutic effects of the intradiscal steroid injection in patients with lumbar discogenic pain have been controversial so far. The purpose of this study is to de- termine the therapeutic effects of the intradiscal steroid in- jection in acute phase of lumbar discogenic pain. Method:
From June 2006 to July 2009, among the patients admitted for acute severe low back pain, ten patients (4 males, 6 females) were diagnosed with lumbar discogenic pain using by lumbar magnetic resonance image (MRI) and the pain-provocative discography was carried out at the inter- vertebral disc revealed to posterior annular high intensity zone on MRI. All patients were injected steroid into the painful disc, and the pain intensity (Visual analogue scale, VAS), measure of disability (Oswestry disability index, ODI;
Roland-Morris disability questionnaire, RMD) before, 1 week and 3 months after the injection were evaluated. Results:
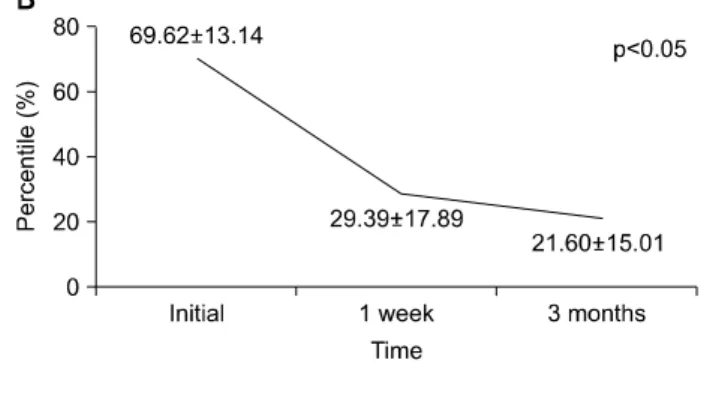
The VAS fell from 8.4±1.0 to 1.8±1.5 at 3 months post- procedure. At 3 months, the ODI fell from 69.6±13.1 to 21.6±15.0% and the RM from 18.7±2.3 to 4.2±4.8 points.
There were significant improvements after the intradiscal steroid injection compared with pre-procedure in all of the measures (p<0.01). Conclusion: The intradiscal steroid injection in acute lumbar discogenic pain was significantly effective in early pain relief, and might be expected to reduce
chronic low back pain from segmental instability and secon- dary inflammation. (Clinical Pain 2015;14:16-20)
Key Words: Discogenic pain, Steroid injection, Discography, Core muscle
INTRODUCTION
The intervertebral disc is a common source of chronic low back pain.
1,2Discogenic back pain is thought to be the result of disc itself rather than of nerve root irritation caused by prolapsed disc,
2and stems from radial tears of the annulus fibrosus extending from the nucleus to the out- er third of the annulus which, in turn, may expose the nerve endings to enzymes and degradation products.
1History, physical examination and radiological imaging have low sensitivity and specificity in diagnosing dis- cogenic low back pain,
3and it is well known that dis- cography is the criterion standard to confirm whether a par- ticular disc is the source of pain or not.
4,5Treatment for discogenic back pain is typically con- servative and since discography is rather an invasive proce- dure, the patients who are suffering from discogenic back pain generally do not undergo discography unless the pain persists over 6 months.
6If the discogenic back pain is not treated properly in ear- ly stage, such as in case of acute, severe discogenic back pain not responding to the conservative treatment, the noci- ceptive fibers continue to grow into the intervertebral disc and secondary inflammation from annular tear mediated by nerve growth factor (NGF) or other cytokines may facili- tate disc degeneration,
7,8eventually leading to chronic low back pain.
When the discogenic back pain becomes chronic, dy-
namic trunk stability and appropriate feedforward activa-
Table 1. Patient Characteristics
Gender
Male:female 4:6
Age (year)
Mean±SD 39.8±9.9
Range 24 to 53
Duration of symptoms (day)
Mean±SD 9.4±9.3
Range 1 to 31
Level of symptomatic disc (cases)
L4/5 7
L5/S1 3
SD: Standard deviation.
tion modulated by the central nervous system could be compromised
9and this can be an additional factor which inhibits the patients with discogenic back pain from doing proper exercises. So it is worthwhile to consider that early intervention using steroid injection in the patients with dis- cogenic back pain in the acute stage can provide positive ef- fect in terms of reducing secondary inflammation and giving the opportunity of stabilizing dynamic trunk musculature.
The objective of this study is to determine the ther- apeutic effects of the intradiscal steroid injection in acute phase of discogenic back pain and to investigate the func- tional outcome of the patient who underwent the intradiscal steroid injection therapy.
MATERIALS AND METHODS
A total of 10 patients who were diagnosed to acute dis- cogenic back pain were enrolled in a consecutive manner from 2006 to 2009. Acute discogenic back pain was de- fined as axial low back pain of a deep, aching or throbbing feature with or without concomitant referred pain on one or both lower extremities which had not lasted over a month from its onset.
Magnetic resonance imaging (MRI) and provocation dis- cography were undertaken for these patients. Before under- going discography, informed consent was obtained from each patient and the patients were excluded if they met the following contraindications of discography in accordance with the criteria of International Spine Intervention Society:
1) the patient is unable or unwilling to consent to the pro- cedure, 2) inability to assess patient response to the proce- dure, 3) the patient has evidence of an untreated localized infection in the procedural field, and 4) known bleeding diathesis or current use of anticoagulants.
All patients were given antibiotics for prophylaxis 30 minutes before the procedure and after sterility was con- firmed, 23 gauge needles were placed into the symptomatic disc and at least one adjacent control disc using postero- lateral approach under fluoroscopic guidance of a C-arm image intensifier (OEC
Ⓡ9800 Plus; GE OEC Medical System, Inc., Salt Lake City, USA) while the patients were lying in prone position. After the needles were placed in the center of nucleus pulposus, a dye (Omnipaque; GE Healthcare, Shanghai, China) was injected using the auto- mated pressure-controlled discography (APCD) system.
A positive disc was defined under the criteria of International Spine Intervention Society: 1) stimulation of the target disc reproduces concordant pain, 2) that pain is
≥7 on a visual analogue scale (VAS, range 0 to 10), 3) that pain is reproduced at a pressure of less than 50 psi above opening pressure, and 4) stimulation of adjacent discs does not reproduce pain. Once a positive disc was confirmed, 1 ml containing 40 mg of triamcinolone was in- jected through the symptomatic disc.
All patients were followed up prospectively for assessing the changes of pain and function using a questionnaire that included VAS, Oswestry disability index (ODI, range 0 to 100) and Roland-Morris disability questionnaire (RMD, range 0 to 24). These 3 outcome measures were assessed before the procedure, 1 week and 3 months after the proce- dure, respectively.
Wilcoxon signed rank tests before and at each follow-up period were used in all analysis and a p-value of less than 0.05 was considered statistical significant (SPSS statistical software 18.0, SPSS Inc., Chicago, USA).
RESULTS
A total of 10 cases of acute discogenic low back pain confirmed by provocation discography were enrolled. All cases were less than 1 month from their onset. Levels of symptomatic disc were L4/5 in 7 cases and L5/S1 in 3 cases. The demographic characteristics were summarized in Table 1.
All of the VAS, ODI and RMD scales revealed sig-
nificant improvements after intradiscal steroid injection
Fig. 1. The figure demonstrates statistical improvements