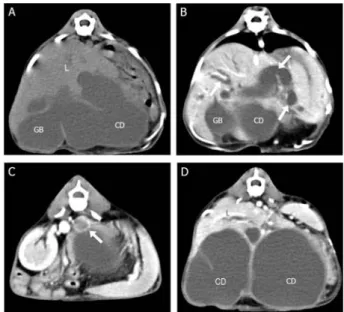
Imaging diagnosis of extrahepatic biliary tract obstruction with acquired portosystemic shunt in a cat
4
0
0
전체 글
(2)
(3)
(4)
수치
관련 문서
In the efficiency review of the Trombe wall system through the experiment, if the Trombe wall was applied in the building structure, the Trombe wall had the
In contrast, Chiropractic has shown better result than sports massage in the range of motion of the shoulder joint, Thoracic Scapular rhythm test, and the
6. Acute biliary pancreatitis: the roles of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography.. endoscopic ultrasonography in the
The index is calculated with the latest 5-year auction data of 400 selected Classic, Modern, and Contemporary Chinese painting artists from major auction houses..
After first field tests, we expect electric passenger drones or eVTOL aircraft (short for electric vertical take-off and landing) to start providing commercial mobility
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
Preoperative evaluation of pelvic lateral lymph node of patients with lower rectal cancer: comparison study of MR imaging and CT in 53 patients?.
• In itself, this decline poses little danger however it renders the aging kidney more vulnerable to acquired insults (volume depletion, nephrotoxins, contrast dye). •
