180
Original Article
Korean Circulation J 2007;37:180-182
ISSN1738-5520
ⓒ 2007, The Korean Society of Circulation CASE REPORT
Infective Endocarditis with Isolated Double Chambers of the Right Ventricle during Adulthood
Young-Hoon Kim, MD, Eui Nam Hwang, MD, Yunjin Jung, MD, Keun Lee, MD, Hoon Ki Park, MD, Chang-Bum Park, MD and Joong-Il Park, MD
Department of Internal Medicine, Seoul Veterans Hospital, Seoul, Korea ABSTRACT
Isolated double chambers of the right ventricle (DCRV) are a rare variant of congenital heart disease. We report here on a case of right-sided infective endocarditis with isolated DCRV that presented in adulthood. (Korean Circulation J 2007;37:180-182)
KEY WORDS:Endocarditis;Congenital heart defect.
Introduction
Congenital heart disease(CHD) is a major factor that predisposes people to infective endocarditis(IE). IE has a high mortality rate, up to 10%, and the incidence of IE associated with CHD in adulthood has been re- ported to be recently increasing due to the long-term survival of CHD patients.1) Therefore, more attention is gradually being paid to IE.1)2) Right-sided IE occurs in about 5-10% of the total IE cases, and the presence of uncorrected CHD is considered as the most impor- tant predisposing risk factor for patients with right- sided IE in Korea.3) We report here on a case of pul- monic valve endocarditis with isolated double chambers of the right ventricle(DCRV).
Case
A 56-years-old woman, who was diagnosed with iso- lated double-chambers of the right ventricle(DCRV) (Fig. 1) 12 months ago, was admitted for her recurrent high fever. She had been treated with only intermit- tent empirical antibiotics at a local clinic for a high fever; this fever had developed 2 months after the di- agnosis of DCRV. At the time of the diagnosis of DC- RV, this patient had refused surgical treatment. Prior
to the onset of fever, there was no history of dental procedure, tattoo, acupuncture, ear piercing or intra- venous drug abuse; there was a history of right cardiac catheterization for making the diagnosis of DCRV.
On physical examination, a systolic ejection murmur was noted at the left parasternal border. In addition to the mild cardiomegaly shown on chest radiography, an electrocardiogram showed right ventricular hypertrophy with right axis deviation, and this was suggestive of right ventricular overload. However, there were no ob- jective signs suggesting infective endocarditis.
The two-dimensional(2D) transthoracic echocardio- graphy on a right ventricular outflow view showed the large oscillating vegetation attached to the pulmonic valve with a turbulent Doppler color flow jet across a stenotic mid-right ventricle to the dilated pulmonary artery(Fig. 2), and the pressure gradient between the pulmonary artery and the right ventricle was 30 mmHg.
Enterococcus faecalis was positive from blood cultures that were drawn more than 12 hour apart. The diag- nosis of IE was made based on Duke’s Criteria. After treatment with combination antibiotics for 8 weeks, the vegetation was resolved.
Discussion
It is reported that about 10-20% of IE is associated with preexisting CHD.4)5) Although, most of the CHD patients have a high risk of IE, ventricular septal defect, patent ductus arteriosus, aortic valve abnormalities and tetralogy of Fallot are considered the common preope- rative factors for IE.1)2) However, to the best of our knowledge, IE in a DCRV patient has never been
Received:January 11, 2007 Accepted:February 16, 2007
Correspondence:Joong-Il Park, MD,Division of Cardiology, Department of Internal Medicine, Cardiac and Vascular Center, Seoul Veterans Hospital, 6-2 Dunchon-dong, Gangdong-gu, Seoul 134-791, Korea
Tel: 82-2-2225-1776, Fax: 82-2-484-8709 E-mail: [email protected]
Young-Hoon Kim, et al: Endocarditis with Double Chambers of the Right Ventricle·181
reported on. This is the first case report to demonstrate pulmonic valve IE with isolated DCRV.
DCRV is a congenital cardiac anomaly in which the right ventricle is divided into two chambers, a proximal high-pressure(anatomically lower) chamber and a distal low-pressure(anatomically higher) chamber, by anom- alous muscles or fibrous tissues in the right ventricular cavity.6)7) The isolated DCRV is an exceptionally rare
condition. It is most commonly associated with a membranous type ventricular septal defect(VSD),8) and most cases of DCRV are diagnosed and treated during childhood. By contrast, an initial presentation during adulthood has rarely been reported on.7)9)
Many cases of right sided IE are related to intravenous drug addiction in the western countries. In Korea, the most important risk factor for right sided IE is known
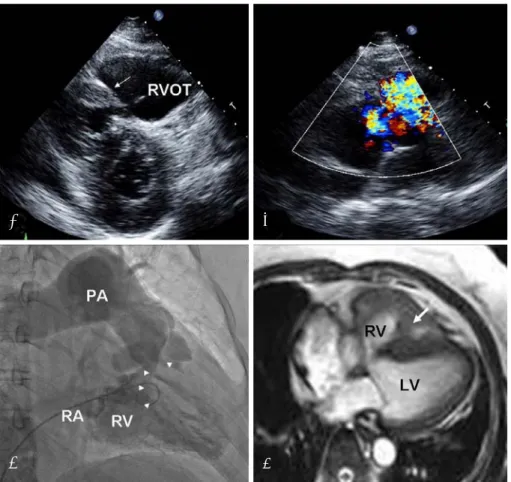
Fig. 1. The two dimensional (2D) echocardiography, right ventriculogram and MR imaging of the isolated double-chambers of the right ventricle. A and B: two dimensional (2D) echocardiography shows a turbulent Doppler color flow jet through a stenotic mid-right ventricle with an anomalous muscle bundle (arrow). C: right ventriculogram demonstrating a severely hypertrophied muscle bundle (arrowheads), resulting in division of the right ventricle into two chambers, and a dilated pulmonary artery with normal infundibular contraction. D: 2D cine MR imaging showing the anomalous muscle bundle (arrow). LV: left ventricle, RA: right atrium, RV: right ventricle, RVOT: right ventricular outflow tract, PA: pulmonary artery.
C D
B A
Fig. 2. 2D echocardiography of infective endocarditis. A and B: 2D echocardiogram shows the oscillating vegetation attached to the pulmonic valve in the dilated pulmonary artery. C: turbulent Doppler color flow jet through the pulmonic valve.
C B
A
182·Korean Circulation J 2007;37:180-182
to be uncorrected CHD.3) In our present case, DCRV might be the risk factor for right sided IE on the pul- monic valve.
IE is considered to be one of the important compli- cations in the adult population suffering with con- genital heart disease. Chronic hypoxia, previous car- diovascular operation, repair with foreign material, cardiac interventional procedures and dental proce- dures have been suggested to be predisposing factors for IE in these patients.10) However, the predisposing factors for IE are difficult to identify in the large ma- jority of patients with known CHD. Moreover, most of these CHD patients have not undergone regular medical check-ups.1)11) The previous cardiac catheterization might be the predisposing risk factor for our IE patient, who had known CHD. This present case exemplifies the im- portance of physicians being aware of this disease and the appropriate treatment for those patients with un- derlying CHD to prevent complications.
REFERENCES
1) Noh JI. Infective endocarditis in congenital heart disease pa- tients: it’s time to pay more attention. Korean Circ J 2006;36:
252-4.
2) Kim SH, Huh J, Kang IS, et al. Infective endocarditis in ado- lescents and adults with congenital heart disease. Korean Circ J 2006;36:318-23.
3) Park CB, Kim JJ, Song JK, et al. Right-sided infective endo- carditis in Korea. Korean Circ J 2005;35:633-8.
4) Hoffman JI, Kaplan S, Liberthson RR. Prevalence of congenital heart disease. Am Heart J 2004;147:425-39.
5) Lefevre M, Guerin P. Enodocarditis and congenital heart disease in the adult. Arch Mal Coeur Vaiss 2002;95:1056-64.
6) Nagashima M, Tomino T, Satoh H, Nakata T, Ohtani T, Saito H.
Double-chambered right ventricle in adulthood. Asian Cardiovasc Thorac Ann 2005;13:127-30.
7) Hoffman P, Wojcik AW, Rozanski J, et al. The role of echocar- diography in diagnosing double chambered right ventricle in adults. Heart 2004;90:789-93.
8) Cil E, Saraclar M, Ozkutlu S, et al. Double-chambered right ventricle: experience with 52 cases. Int J Cardiol 1995;50:19-29.
9) Park JI, Kim YH, Lee K, Park HK, Park CB. Isolated double- chambered right ventricle presenting in adulthood. Int J Cardiol 2006. [Epub ahead of print]
10) Knirsch W, Haas NA, Uhlemann F, Dietz K, Lange PE. Clinical course and complications of infective endocarditis in patients growing up with congenital heart disease. Int J Cardiol 2005;
101:285-91.
11) Li W, Somerville J. Infective endocarditis in the grown-up con- genital heart (GUCH) population. Eur Heart J 1998;19:166-73.