협착이
6
0
0
전체 글
(2) 조영술 시행 후 응급수술을 시행하였다. 수술소견에서 우. 바가 없다. 저자들은 58세 남자환자가 안정시 흉통을 호소하며,. 중대뇌동맥의 분지부위에 4 mm 크기의 동맥류가 발견. 심전도에서 가역적인 허혈이 의심되어 시행한 관상동맥. 되어 직접동맥루결찰술을 시행하였다. 이 후 전신상태 호. 조영술에서 좌회선동맥 및 우관상동맥의 관상동맥루가. 전 되던 중 수술 후 15일경부터 안정 시 하루 1~2회 가. 관찰되었으며, 좌전하행동맥에서 좌회선동맥으로의 역류. 량 30분 정도 지속되는 전흉부 통증을 호소하였다.. 로 인하여 coronary steal syndrome이 발생하여 심근. 검사실 소견:내원 당시 시행한 혈액검사에서 총 콜. 허혈 증상을 일으킨 1예를 경험하였기에 문헌고찰과 함. 레스테롤은 143 mg/dl였으며, 말초혈액검사, 혈청생화학. 께 보고한다.. 검사, 전해질검사, 뇨검사 및 흉부방사선 검사에서 이상소 견은 없었다. 수술 후 흉통 호소 시 시행한 CK/CK-. 증. 례. MB/LDH는 31/9/248 IU/L였다. 심전도:흉통을 호소하지 않았던 시기의 심전도는 정. 환 자:송○회, 남자 58세.. 상소견이었으며, 흉통 호소 시 시행한 심전도에서는 유. 주 소:지주막하 출혈로 수술 후 휴식 시 발생한 간. 도 V1-V6, I, II, aVF에서 T파 역위소견이 관찰되었다. 헐적 흉통. 과거력:고지혈증, 고혈압, 당뇨병 및 심장병의 병력 은 모두 없었다.. (Fig. 1). 흉통이 소실되면 이러한 심전도의 이상소견도 소실되었다. 관상동맥조영술 소견:관상동맥조영술에서 우관상동. 사회력:흡연력과 음주력은 모두 없었다.. 맥과 좌회선동맥의 동정맥루가 관찰되며, 우관상동맥의. 현병력:평소 건강하게 지내던 환자는 내원 1일전 갑. 원위부에서 좌심방내로 조영제가 퍼져나가는 비정상적. 자기 시작된 두통을 주소로 인근병원 방문하여 지주막. 인 혈관교통이 관찰되었다(Fig. 2). 좌전하행동맥에서 좌. 하출혈이 의심되어 정확한 진단 및 치료를 위하여 본원. 회선동맥으로의 조영제 역류가 관찰되었다(Fig. 3).. 으로 전원되었다.. MIBI 심근스캔:부하 및 휴식시 시행한 MIBI 심근. 진찰소견 및 경과(1):신장은 165 cm, 체중은 59. 스캔의 부하영상 소견에서 좌전하행동맥의 관류부위인 심. kg이었으며 내원 당시 혈압은 128/80, 맥박수는 76회,. 첨부에서 관류결손이 관찰되며 이는 휴식 영상에서 관류. 의식은 다소 저하되어 있었다. 이에 경대퇴동맥대뇌혈관. 가 회복되어 가역적인 관류결손임을 확인하였다(Fig. 4).. Fig. 1. Electrocardiogram:Panel A:shows normal ECG finding during symptom free period. Panel B:shows T wave inversions on V16, I, II and aVF during resting chest pain episode.. 825.
(3) Fig. 2. Coronary angiography:Panel A:Left coronary angiogram shows LCX arteriovenous fistula. Panel B:Right angiogram shows RCA fistula to left atrium, arrows indicate fistulae.. 수술소견:개심술을 시행하여 좌회선동맥의 동정맥. 상동맥누관을 형성한 환자에서 운동부하검사에서 심근 허혈을 보이면서 심근스캔에서 부하시 전벽부위에 가역. 루 개구부를 결찰하였다. 경 과(2):수술 후 환자는 흉통없이 지주막하 출혈로 인한 신경학적 결손에 대한 재활 치료 후 퇴원하였다.. 적인 관류결손을 관찰하였으며 coronary steal syndrome에 의해 누관의 원위부로 가는 혈류가 감소하여 심 근허혈이 유발되었다고 보고하였다.. 고. 찰. 본 증례에서는 협착 또는 죽상경화성 관상동맥 질환이 없는 2개의 주요 심외막동맥 사이에서 coronary steal. 일반적인 의미에서의 coronary steal은 소동맥의 혈. 이 발생한 경우로 이러한 경우 관류를 결정하게 되는 혈. 관확장시 혈류가 동측측부 심근으로 관류됨에 따라 협. 류에 대한 저항은 대부분 소동맥에 의한 것으로 볼 수. 착 등의 병변이 있는 관상동맥 관류의 저하를 가지고 오. 있다. 본 증례에 있어 좌전하행동맥의 원위부에는 소동. 는 상황을 의미한다. 대표적인 예로 심근스캔시 부하를. 맥이 존재하여 혈류저항이 있으나, 좌회선동맥의 원위부. 위하여 혈관확장제인 dipyridamole 주입시 협착 등의. 에는 정상적인 혈류저항을 일으키는 소동맥이 없고 혈류. 병변이 없는 부위의 저항혈관인 소동맥이 확장됨에 따라. 에 대하여 저항을 일으킬 수 있는 근육층이 없는 동정. 약물 주입 이전에 이미 소동맥 혈관확장이 일어나 있는. 맥루가 관찰되어 혈류가 과도하게 증가되었다. 이 경우. 병변부위에 유발되는 관류결손을 생각할 수 있다.6)7) Co-. 의 역류소견을 분석해 보면, 소동맥의 저항이 높은 수축. ronary steal syndrome이 주로 문헌에 보고되는 경우. 기에는 좌전하행동맥으로부터 이러한 저항이 없는 좌회. 는 coronary-subclavian steal syndrome 또는 cor-. 선동맥으로 혈류저항의 차이에 따라서 혈류가 역류됨에. onary pulmonary steal syndrome과 같이 협착 등의 병. 따라 좌전하행동맥의 관류부위에 coronary steal이 발. 8-11). 변이 있는 혈관 사이에서 steal이 발생하는 경우이며. 생하였다. 이완기에서도 비록 소동맥의 저항이 상대적으. 협착이 없는 coronay artery 내에서 steal이 발생한 경. 로 저하되나 지속적인 저항의 차이에 따라서 역류가 지. 우는 세계적으로 드문 경우라 할 수 있다. Gradus 등12). 속되고 있다고 볼 수 있겠다.. 은 관상동맥질환이 없으면서 아전가지에서 좌심실로 관 826. 관상동맥루는 관상동맥이 심방, 심실 및 정맥과 교통 Korean Circulation J 2001; 31(8):824-829.
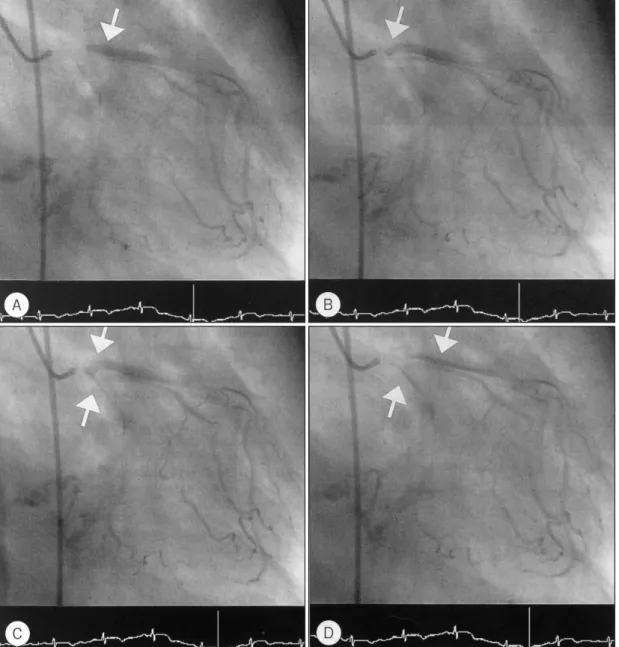
(4) 하는 비교적 드문 질환이기는 하지만 관상동맥 기형 중. 양성, 죽상경화성 심질환이 선행되는 후천적이 발병이 보. 혈역학적으로 중요한 의미를 가지는 가장 흔한 관동맥. 고되고 있다.13)14) 선천성 관상동맥루는 그 기시부에 따. 기형이다. 약 절반의 환자에 있어서는 무증상이나, 나머. 라 우관상동맥 및 그 분지에서 약 50%, 나머지 50%는. 지 절반에 있어서는 혈역학적인 변화를 일으켜 심부전,. 좌관상동맥 및 다발성 기시부를 가지고 있음이 보고되. 심내막염, 심근허혈, 파열, 심근경색 등의 심각한 합병증. 고 있으며 이들의 누관은 유출은 우심실로 41%,우심. 을 초래할 수 있다. 관상동맥조영술이 보편화되면서 관. 방으로 26%, 폐동맥으로 17%, 좌심실로 3%, 상대정맥. 상동맥루의 발견 빈도와 증례보고가 국내에서도 증가하. 으로 1%로 보고되고 있다.15) 본 증례에서 관찰된 누관. 는 추세이고. 대부분 선천적으로 발병되지만 외상성, 종. 은 유출부가 좌심방으로 관찰되고 있어 이 또한 드문. Fig. 3. Left coronary angiography:ECG indicates that Panel A, B, C, D is sequencial, arrows indicate retrograde flow from LAD to LCX.. 827.
(5) Fig. 4. Stress/rest MIBI myocardial SPECT:stress image shows perfusion defect at apical wall, LAD territory, resting image shows normal perfusion at apical wall, LAD territory, so it means that perfusion defect is reversible at apical wall, LAD territory.. 경우라 할 수 있다. 선천성 관상동맥루의 치료는 증상. 심전도에서 심근허혈이 의심되어 시행한 관상동맥 조영. 이 있거나 합병증이 생긴 경우, 단락의 양이 많아 혈역. 술에서 좌회선동맥 및 우관상동맥의 관상동맥루가 관찰. 학적으로 문제가 되는 경우에는 수술적 치료를 권한다.. 되고, 좌전하행동맥에서 좌회선동맥으로의 역류에 의한. 증상이 없거나 단락의 양이 적은 경우에 예후가 좋은. coronary steal syndrome이 발생하였다. 부하 / 휴식. 것으로 알려저 있어 최근에는 단락의 양이 매우 적은 경. MIBI 심근스캔에서 가역적인 관류결손이 관찰되어 수술. 우를 제외하고는 나이가 들수록 합병증의 빈도가 높아. 을 시행하였으며 이 후 흉통없이 퇴원한 1예를 경험하. 지고 수술 후 합병증도 많아지므로 증상이 없더라도 조. 였기에 문헌고찰과 함께 보고한다.. 16). 기 외과적 치료를 권하고 있는 있다.. 수술에 대신하여 도관을 통한 색전술이 시도되고 있으. 중심 단어:Coronary steal syndrome・관상동맥루.. 며,17-19) 국내에서도 coil을 이용한 경피적 경도관 색전 술을 시행하여 성공적으로 치료한 예가 보고되고 있다.20). REFERENCES 1) Seiler C, Fleisch M, Meier B. Direct intracoronary evid-. 수술적 방법으로는 단일 혈관이 좌심실로 누관을 형성 한 예에서 외과적인 교정을 시행한 예들이 있으며, 좌우. 2). 단락으로 혈역학적 과부하, 세균성 심내막염, coronary steal syndrome 등이 유발되어 이에 대한 수술적 교정 을 한 예가 보고되고 있다.21) 저자들이 경험한 본 예에. 3). 서는 휴식 시 간헐적인 통증을 나타내며, 심전도에서 가 역적인 심근허혈을 시사하고, 부하/휴식 MIBI 심근스캔. 4). 에서 좌전하행동맥 관류부위에 가역적인 관류장애가 있 어 coronary steal syndrome에 의한 심근허혈로 생각. 5). 되어 교정이 필요한 경우로 수술을 시행하였다.. 요. 약. 저자들은 58세 남자환자가 휴식시 흉통을 호소하며, 828. 6). 7). ence of collateral steal in humans. Circulation 1997;96: 4261-7. Braunwald E, Zipes DP, Libby P. Heart disease: A textbook of cardiovascular medicine. 6th ed. W.B.Sanders; 2001. p.404-5. Kim SY, Park HS, Park SJ, Park KW, Suh JK, Kwon J, et al. A case of acquired coronary artery fistula to the left ventricle after acute myocardial infartion. Korean Circulation J 2000;30:221-6. Shin GJ, Lee WK, Chung NS, Shim WH. A case of coronary artery-pulmonary artery fistula associated with angina pectoris. Korean Circulation J 1985;15:545-9. Park SJ, Cho SY, Lee WK, Chung NS, Shim WH. A case of bilateral coronary artery-pulmonary artery fistula. Korean Circulation J 1986;16:555-8. Lette J, Tatum JL, Fraser S, Miller DD, Waters DD, Heller G, et al. Safety of dipyridamole testing in 73,806 patient: The multicencter dipyridamole safety study. J Nucl Cardiol 1995;2:3-17. Braunwald E, Zipes DP, Libby P. Heart disease: A tex-. Korean Circulation J 2001; 31(8):824-829.
(6) 8). 9) 10) 11) 12). 13). 14). tbook of cardiovascular medicin. 6th ed. W.B.Sanders; 2001. p.287, 1099. Viecili PR, Pamplona D, Cesena FH, da Luz PL. Unstable angina due to communication between the coronary artery and the right pulmonary artery in patient with Takayasu’s arteritis. Arq Bras Cardiol 1997;69:129-32. Najm HK, Gill IS, FitzGibbon GM, Keon WJ. Coronarypulmonary steal syndrome. Ann Thorac Surg 1996;62: 264-5. Kawasuji M, Tekemura H, Sakakibara N, Matsui O, Watanabe Y. Coronary steal caused by a right gastroepiploic artery graft. Ann Thorac Surg 1994;57:1645-7. Gaya J, Del Rio Prego A, Guilleuma J, Vela P, Arribas A, Lopez Parra JJ, et al. Coronary steal syndrome. Cardiovasc Surg 1993;1:186-9. Gradaus F, Peter AJ, Schoebel FC, Gradaus D, Leschke coronary steal syndM, Strauer BE. Angina pectoris in “ rome”caused by a coronary fistula in the left ventricle. Dtsch Med Wochenschr 1998;123:1030-4. Gildein HP, Kleinert S, Layangool T, Wilkinson JL. Acquired coronary artery fistula in children after ventricular septal myectomy of the right or left ventricular outflow tract. Am Heart J 1995;130:1124-6. Nawa S, Tamesue K, Yamamoto H. Fistula formation from neovascularity developing in malignant histiocytoma of the heart. Br J Radiol 1997;70:1066-7.. 15) Levin DC, Fellows KE, Abrams HL. Hemodynamically 16) 17). 18). 19). 20). 21). significant primary anomalies of the coronary arteries, Angiographic aspects. Circulation 1978;58:25-34. Sakakibara S, Yokoyama M, Takao A, Nogoi M, Gomi H. Coronary arteriovenous fistula: Nine operated cases. Am Heart J 1966;72:307-14. Mavroudis C, Backer CL, Rocchini AP, Muster AJ, Gevitz M. Coronary artery fistulars in infants and children. A surgical review and discussion of coil embolization. Ann Thorac Surg 1997;63:1235-42. Nguyen NH, Reeves F, Therasse E, Latour Y, Genest J Jr. Percutaneous transluminal angioplasty in coronaryinternal thoracic-subclavian steal syndrome. Can J Cardiol 1997;13:285-9. Voges E, Schild H, Thelen M. Therapy of coronary steal syndrome by percutaneous transluminal angioplasty. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 1995; 163:269-70. Cho JS, Kim DS, Suh JK, Jang YS, Kim HS, Lee DY. A case of percutaneous transcatheter coil embolization for congenital coronary arteriovenous fistula. Korean Circulation J 1997;27:927-32. Effler DB, Sheldon WC, Turner JJ, Groves LK. Coronary arteriovenous fistula: Diagnosis and surgical management. Report of 15 cases. Surgery 1967;61:41-50.. 829.
(7)
수치
관련 문서
Coronary angiography and intravascular ultrasound revealed multiple thrombotic occlusion of the mid left anterior descending artery, mid left circumflex artery and obtuse
Coronary angiogram revealed total occlusion with large thrombus of distal left anterior descending artery, distal left circumflex artery and 1st diagonal artery... Fourth
A diagnostic coronary angiogram revealed total occlusion in the proximal left ante- rior descending artery (LAD) with collaterals from the right coronary artery and left
A coronary angiogram was performed, which demonstrated 95% stenosis of the middle left anterior descending coronary artery (LAD), 95% stenosis of the prox- imal left circumflex
Coronary angiogram showed severe stenosis in mid portion of left descending coronary artery (A), proximal portion of left circumflex coronary artery (B), and proximal portion of
Image quali- ty of the eight coronary segments [left main coronary artery (LM), proximal and middle segments of left anteri- or descending artery (p-LAD, m-LAD) and left
(A) Left coronary angiogram shows total occlusion of the left anterior descending artery and the left circumflex artery, (B) Right coronary angiogram shows critical diffuse stenosis
coronary artery-pulmonary artery fistula originating from Left Anterior Descending artery: A case report and literature review.. Acquired coronary artery-pul monary
