A transverse radial tear of the midbody of the lateral meniscus is rare. Its treatment has been shown to be difficult espe- cially for tears that extend to the peripheral vascular zone. The literature shows that the treatment outcomes for these tears are generally unfavorable. In this technical note, we describe a modified all-inside repair technique for radial tears of the midbody of the lateral meniscus that is simple and safe. Our novel technique achieves a more accurate anatomic reduction and stronger fixation strength by using a vertically-oriented absorbable suture without additional skin inci- sion. Furthermore, our technique is cost effective in that it requires only two spinal needles and no suture hooks for the repair. We recommend this method as another treatment option for repairs of radial tears of the midbody of the lateral meniscus.
Keywords: Lateral meniscus; Mid-body radial tear; Modified all-inside repair; Spinal needle
Modified all-inside meniscal repair using spinal needles for radial tear of the midbody of the lateral meniscus:
a technical note
Jinho Cho
Department of Orthopedic Surgery, Inje University Ilsan Paik Hospital, Goyang, Korea
Copyright © 2016 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received April 29, 2016; Revised July 14, 2016; Accepted July 14, 2016
Correspondence to: Jinho Cho, Department of Orthopedic Surgery, Inje University Ilsan Paik Hospital, 170 Juhwa-ro, Ilsanseo-gu, Goyang 10380, Korea. Tel: +82-31-910-9733, Fax: +82-31-910-7967, E-mail: [email protected]
Arthroscopy and Orthopedic Sports Medicine
AOSM
INTRODUCTION
Numerous surgical techniques have been developed for meniscal repairs such as the all-inside method, the inside-out method, the outside-in method, and varia- tions of these techniques. Because each technique has different advantages and disadvantages, the choice of repair technique cannot be generalized but rather de- pends on the location and on the pattern of the meniscal injury. To achieve optimal healing in a meniscal repair, it is important to approximate the torn surfaces adequately through firm fixation. It has been shown that meniscal re- pairs using the all-inside method with either commercial fixation devices or suture hooks provide good coaptation and strong holding power through a vertically oriented suture. Vertically oriented sutures promote healing of the tear site [1,2].
Most transverse radial tears of the middle horn of the lateral meniscus are simple transverse tears, which can
be seen through radiographic imaging as a single cut on a sagittal or an axial magnetic resonance imaging (MRI) scan (Fig. 1). In this study, we demonstrate a novel al- ternative method for meniscal repairs that bypasses the need to make a skin incision, yields a more accurate ana- tomic reduction, and provides stronger fixation through vertically oriented absorbable sutures, which are tied on the superior and the inferior facets of the meniscus. This all-inside meniscal repair can be performed with only spinal needles. And we created two standard portals (the anterolateral portal and the anteromedial portal) without any additional portals or skin incision, which adds fur- ther cosmetic benefit.
TECHNIQUE
A 16-year-old female patient was hospitalized for an injury in her right knee after slipping down the stairs.
She complained of a moderate onset of pain upon walk-
ing and of direct tenderness around the lateral joint. We performed an arthroscopic meniscal repair using two 18-gauge spinal needles, a suture retriever, and two types of suture material—an absorbable No. 2 PDS (Ethicon, Somerville, NJ, USA) and a No. 0 Maxon (Covidien, Man- sfield, MA, USA) suture material. The patient was placed into position for standard knee arthroscopy. Standard arthroscopic portals, the anterolateral portal and the anteromedial portal, were used without any additional
portals. The right knee was placed into a ‘‘figure of 4’’ po- sition. The diagnostic arthroscopy revealed a radial tear of the midbody of the lateral meniscus involving the red–
red zone and the red–white zone of the lateral meniscus (Fig. 1C).
Using a motorized shaver, we first performed gentle debridement at the tear site and at the surrounding capsule. Then, we pierced two 18-gauge spinal needles through the skin into the capsular portion of the central
A B C
Fig. 1. A sagittal T2-weighted magnetic resonance imaging (MRI) scan (A), an axial MRI scan (B), and an arthroscopic image (C) show a radial tear (arrows) of the midbody of the lateral meniscus of the right knee.
A B
C D
Fig. 2. (A) A gross photograph showing an 18-gauge spinal needle loaded with No. 2 PDS (Ethicon) and another loaded with No. 0 Maxon suture (Covidien) ma- terial. The needles are inserted from the skin near the tear site. The offends of the strings are pulled out via the anterome- dial portal with a grasper. (B) A gross pho- tograph showing the No. 0 Maxon suture, in a pre-knot position, holding the No. 2 PDS at the outside of the anteromedial portal. (C) An arthroscopic image show- ing the knot of the No. 0 Maxon, which was tied by pulling from the lateral skin, around the No. 2 PDS. (D) An arthroscop- ic image shows that both ends of the PDS suture are oriented in a vertical orienta- tion at the skin of the meniscal tear site.
tear site. The spinal needles were inserted near the tear so that they pass the femoral side of meniscus and exit from the tibial surface of the midbody of the lateral meniscus.
Then the No. 2 PDS suture material was fed through one of the spinal needles, and the No. 0 Maxon suture mate- rial also was fed through the other needle. The suture ma- terials were pulled out from the anteromedial portal with a suture retriever or a grasper, and this was performed as carefully as possible so as not to cut the suture material with the beveled tip of the needle (Fig. 2A). We prepared the Maxon into a knot around the PDS suture at the out- side of the anteromedial portal (Fig. 2B). Then, the ends of the Maxon were pulled from the lateral skin. It being pulled into the joint the both strand of the PDS (Fig. 2C).
Arthroscopically, we confirmed that both strands of the PDS suture were vertically crossing the tear site (Fig. 2D).
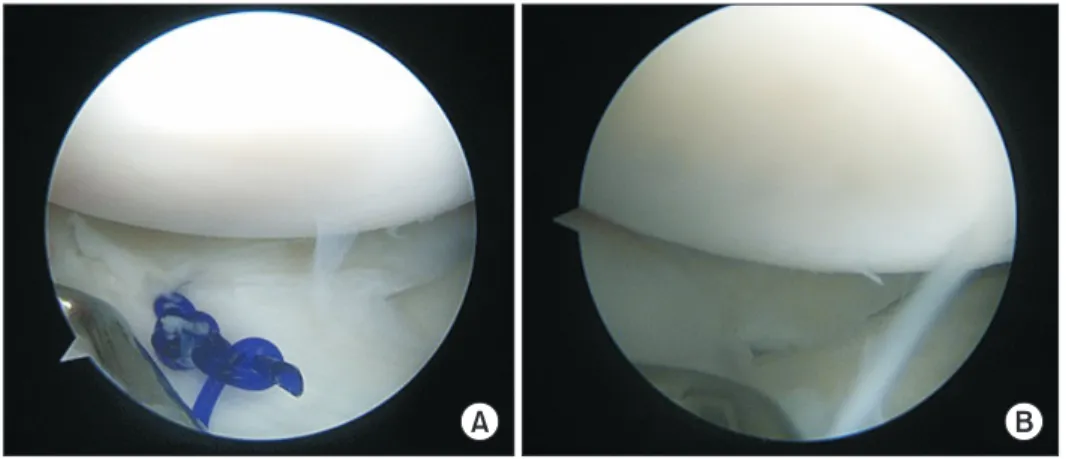
After which we pulled out both ends of the PDS suture via the anteromedial portal with a suture retriever, by doing so bringing the suture into a vertical mattress stitch ready to be tied. This procedure was repeated when a more sta- ble meniscal repair was needed. In an arthroscopically- guided manner, we tied the two PDS suture ends together into an SMC knot so that the meniscus could be reduced through exertion of adequate tension (Fig. 3A). After the knot was tied, we confirmed that there was adequate tension through the anteromedial portal. This modified all-inside method allows us to orient the suture in a verti- cal fashion; this provides not only an adequate contact between the tear surfaces but also firm fixation. We per- formed a second-look arthroscopy after six postoperative months, and the results of the second-look arthroscopy revealed that the lateral meniscus midbody had healed completely across the red–red zone, the red–white zone, and the white–white zone of the meniscus (Fig. 3B).
Postoperative management
Postoperatively, the patient was applied a cylinder leg splint for two weeks in a fully extended position and a limited-motion brace to control motion thereafter. The patient was on non–weight-bearing crutches for 4 to 6 weeks. We asked the patient to perform quadriceps mus- cle exercises as well as straight leg raise exercises several times daily, and after the 1st postoperative month she was begun on active motions up to 90o, which was gradu- ally increased to flexion degrees up to 150o. Full flexion and squatting were only allowed after three postopera- tive months. The patient returned to exercise after the six months of surgery.
DISCUSSION
Conventionally, radial tears of the meniscus have been treated through partial meniscectomy, during which unstable fragments that may cause mechanical symp- toms are removed. But this treatment method has been associated with significantly reduced biomechanical function in these zones and premature osteoarthritic changes. These complications have highlighted the need to improve treatment methods for repairs of radial tears of the meniscus. Different techniques for radial tears of the meniscus have been described in the literature such as the outside-in repair technique [3], the inside-out repair technique [4], and the all-inside repair technique [5]. Tears that extend to the red–red zone of the meniscus often heal effectively because of the extensive vascular- ization around this region [6]. On the other hand, where there is substantially less vascularization, such as the red–
white zone or the middle third of the meniscus, tears are less amenable to healing in spite of treatment. Despite the fact healing is not favorable in these regions, Barber-
A B
Fig. 3. (A) An arthroscopic view of the ends of the PDS suture tied as a vertical SMC knot tie, which exert adequate ten- sion on the reduced meniscus. (B) An arthroscopic image from second-look arthroscopy shows complete healing and repair of the tear.
Westin and Noyes [7], in their systematic review, have reported that 83% of tears in the red–white zone were considered clinically healed after repair.
We have shown that our novel technique described in this report is an effective way to repair radial tears ex- tending to the peripheral vascular zone of the midbody of the lateral meniscus. A key finding of our study is that repairs for such tears can be simple, easy, and effective.
This modified all-inside technique makes vertical absorb- able sutures without needing additional skin incisions.
Further, the incidence of neurovascular complications can be reduced, cosmetically-appealing results can be attained, and by using bioabsorbable devices the com- plications associated with the use of absorbable suture materials can be reduced. We found that most tears of the meniscus are simple transverse radial tears, which present as a single cut on sagittal or on axial MRI scans.
Patients may be symptomatic for a lateral meniscal tear if tenderness or discomfort is felt on the lateral side of the knee joint. In which case, the physician should make a careful observation during MRI examination.
Anatomically accurate repairs are important because non-anatomical placement of the meniscus horn has been reported to significantly alter meniscal function [8].
Several treatment methods have been employed for the anatomical repair of these tears such as the outside-in technique, the inside-out technique, the all-inside tech- nique, and techniques that use artificial devices. The out- side-in meniscal repair was recommended for the repairs of radial tears of the middle horn of the lateral meniscus.
But true vertical sutures are not feasible through this type of repair, and additional skin incisions of about 1 to 2 cm or longer are required. In their study that described the results of five radial tears of the lateral meniscus af- ter outside-in repairs, van Trommel et al. [3] reported three cases of complete healing and two cases of partial healing. Interestingly, they promoted healing through fibrin clotting. Unlike the outside-in repair, the inside- out meniscal repair technique uses two monofilament, non-absorbable 2-0 suture materials. And complications such as irritation of the articular cartilage or foreign body reaction can occur because the sutures are not taken out even after healing. Further, horizontal sutures close the tear site, which is not as strong as vertical sutures.
When Noyes and Barber-Westin [4] used the inside-out technique to repair radial tears involving the avascular zone, they reported that four patients who received the treatment complained of postoperative pain. Through second-look arthroscopy, they confirmed partial healing of the meniscus in one of the patients. Next, the all-inside suture technique uses a suture hook, and the relative ad- vantage of this technique over the classic inside-out tech- nique is that it allows for vertical sutures using absorbable suture material, such as the PDS. Previously, Choi et al.
[5] repaired radial tears involving the vascular zone of the lateral meniscus with a 45o suture hook (Linvatec, Largo, FL, USA) loaded with No. 1 PDS suture material. But when the joint space is too narrow, handling of the suture hook may become difficult and the resultant forceful handling of suture hook can lead to unnecessary damage of the articular cartilage. Other techniques for meniscal repairs include those that use artificial devices like FasT- Fix (Smith & Nephew, Andover, MA, USA). Although the techniques using devices like FasT-Fix are useful for the repair of posterior horn tears, the anatomy of the device means that it cannot be easily directed to tears within the midbody of the meniscus.
To address such disadvantages associated with preex- isting repair techniques, we devised a novel, modified all- inside technique for mesnical repair. We found that the treatment outcomes for radial tears of the midbody of the lateral meniscus through our novel modified technique were satisfactory, but this was dependent on the pres- ence of concomitant injuries. For the objective assess- ment of meniscal healing, we performed second-look arthroscopy or MRI evaluation between six months and two years postoperatively. And meniscectomy was not required in any cases.
In conclusion, we propose our modified all-inside su- ture technique, which not only cost effective and easy to perform but also requires only spinal needles and no suture hooks, as another candidate for treatment options for meniscal tears.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Ahn JH, Wang JH, Oh I. Modified inside-out technique for menis- cal repair. Arthroscopy 2004;20 Suppl 2:178-82.
2. Cho JH. Arthroscopic all-inside repair of anterior horn tears of the lateral meniscus using a spinal needle. Knee Surg Sports Trau- matol Arthrosc 2008;16:683-6.
3. van Trommel MF, Simonian PT, Potter HG, Wickiewicz TL. Ar- throscopic meniscal repair with fibrin clot of complete radial tears of the lateral meniscus in the avascular zone. Arthroscopy 1998;14:360-5.
4. Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscus tears extending into the avascular zone with or without anterior cruciate ligament reconstruction in patients 40 years of age and older. Arthroscopy 2000;16:822-9.
5. Choi NH, Kim TH, Son KM, Victoroff BN. Meniscal repair for radial tears of the midbody of the lateral meniscus. Am J Sports Med 2010;38:2472-6.
6. Arnoczky SP, Warren RF. The microvasculature of the meniscus and its response to injury. An experimental study in the dog. Am J Sports Med 1983;11:131-41.
7. Barber-Westin SD, Noyes FR. Clinical healing rates of meniscus repairs of tears in the central-third (red-white) zone. Arthroscopy 2014;30:134-46.
8. Stärke C, Kopf S, Gröbel KH, Becker R. The effect of a nonana- tomic repair of the meniscal horn attachment on meniscal ten- sion: a biomechanical study. Arthroscopy 2010;26:358-65.