Abstract : Rheumatoid arthritis (RA) is a chronic inflammatory disease of unknown cause. It is characterized by polyarthritis. Currently, treatments for RA include the use of non-steroidal anti- inflammatory drugs (NSAIDs), steroid, disease-modifying antirheumatic drugs (DMARDs), corticos- teroid, and so on. New treatment options for RA have been actively developed. In this study, we determined pharmacological advantages of using omega n-3 polyunsaturated fatty acids (PUFAs) as adjunctive therapy in RA based on articles demonstrating the role of omega n-3 in the prevention and treatment of RA.
Omega n-3 PUFAs can partially suppress a number of inflammatory reactions such as leukocyte chemotaxis and adhesion molecule expression. Mechanisms fundamental to the anti-inflammatory actions of omega n-3 PUFAs involve changing the compositions of cell membrane's phospholipid fatty acids. Omega n-3 PUFAs with inflammation control action may also result in the reduction of pain in rheumatoid arthritis. The benefit of n-3 PUFAs in RA has also been suggested in some clini- cal studies. In conclusion, omega n-3 PUFAs might be useful as an adjuvant therapy for the treat- ment of RA.
[Key words] Rheumatoid arthritis, Omega n-3 polyunsaturated fatty acids, Anti-inflammation effect, Pain control
류마티스관절염 치료에서 오메가-3 다가불포화지방산의 역할
조의상, 최경희 � 순천대학교 약학대학 약학과
Potential Role of Omega n-3 Polyunsaturated Fatty Acids and Its Use in Rheumatoid Arthritis
Eui sang Jo, Kyung Hee Choi �
College of Pharmacy, Sunchon National University, 255 Jungangno, Suncheon, Jeonnam 57922, South Korea
투고일자 2016.8.10; 심사완료일자 2016.8.25; 게재확정일자 2016.9.22
�교신저자 최경희 Tel:061-750-3763 E-mail:[email protected]
Review Article
서론
류마티스관절염(Rheumatoid arthritis, RA)은 정확 한 원인이 밝혀지지 않은 만성 염증성 질환으로 관절 여러 부위에 발생하는 자가면역 질환의 일종이다. 1),2) 관 절 병변에서 활성화된 호중구는 염증성 프로스타글란 딘 E2 (prostaglandin E2, PGE2) 또는 단백분해효소 를 방출시킬 수 있고, 윤활막 세포에서 방출되는 인터 루킨(interleukin, IL), 종양괴사인자(tumor necrosis factor, TNF)와 같은 시토카인(cytokine)은 연골세포, 파골세포 등에 작용하여 뼈와 연골의 파괴를 일으킬 수
있다. 1)-3) 관절뿐만 아니라 관절 외의 폐, 심장, 신장 등
에도 영향을 끼쳐, 폐섬유화증, 혈관염, 빈혈 등의 전신 증상이 발생하기도 하며, 대부분의 환자에서 피로감, 식욕부진, 전신 쇠약감 등의 전구 증상을 시작으로 관 절의 조조강직, 통증, 종창 등의 증상을 보이고, 질병의 활성도에 따라 타관절 및 관절 외로 확대되는 양상을
보인다. 2),3)
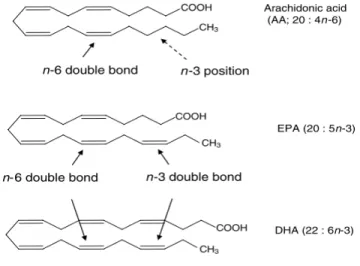
오메가-3(omega n-3 polyunsaturated fatty acids, n-3 PUFAs, ω -3 PUFAs)는 구조적으로 고도 불포화지방산(polyunsaturated fatty acids, PUFAs) 인 물질로 지방산(fatty acid, FA) 아실기 말단에 있는 메틸기로부터 세 번째 탄소에 이중결합이 존재하는 구 조를 통칭한다(Fig. 1). 4) 오메가-3는 α -linolenic acid
(18:3n-3)로 명명되며, 이는 n-6 지방산의 linoleic acid (18:2n-6)로부터 합성된다. 이 과정에서 Δ-15 탈포화효소에 의해 불포화 반응이 일어나는데, 이 때 주목할 점으로 인간에게는 이 효소가 존재하지 않는다 는 사실이다(Fig. 2). 5),6) 따라서 인간의 경우 오메가-3 지방산의 합성이 불가능하므로 오메가-3가 풍부한 생 선 등의 섭취를 통해 외부에서 필요한 영양소를 공급받 게 된다.
그러므로, 정상인의 경우에도 영양학적인 관점에서 오메가-3의 공급이 필요하게 된다. 이 중 대표적인 오 메가-3 성분인 eicosapentaenoic acid (EPA)와 docosahexaenoic acid (DHA)에 대해, 영국 정부에서 는 EPA/DHA 복합성분으로 하루 0.45 g을 섭취하도록 권고하고 있으며, 식량농업기구(Food and Agriculture Organization of the United Nations, FAO)/세계보 건기구(World Health Organization, WHO)에서도 EPA/DHA 복합성분으로 하루 0.25 g의 섭취를 권고 하고 있다. 5),7),8)
오메가-3의 항염증 효과에 대해서는 세포배양연구, 동물실험, 건강한 성인 대상 임상시험을 통해 입증이 되어 왔다. 5),6)
본 글에서는 문헌 검색을 통하여 그 동안 밝혀진 오메 가-3의 작용기전을 기반으로, 류마티스관절염 치료에 적용될 수 있는 이론적인 배경을 살펴보고, 류마티스관
Fig. 1 Basis for n-3 and n-6 fatty acid designation 4)
DHA, docosahesaenoic acid; EPA, eicosapentaenoic acid
4)절염의 질병 단계에 따른 오메가-3 추가 사용에 관한 임상시험 결과를 확인해 보고자 한다.
본론
1. 류마티스관절염의 치료지침
류마티스관절염의 치료에는 비스테로이드성 소염제, 스테로이드, 항류마티스약제, 생물학적제제 등이 사용
된다. 2),9)
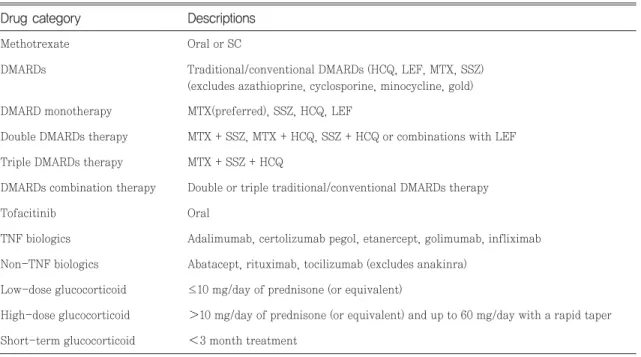
2015 미국 류마티스 학회(American College of Rheumatology, ACR) 가이드라인에서는 발병 기간이 6개월 미만인 조기 류마티스관절염(early RA)과 6개 월 이상의 확정 류마티스관절염(established RA) 치료 제로 합성 항류마티스 약제(Disease-modifying antirheumatic drugs, DMARDs), 생물학적 DMARDs, tofacitinib과 글루코코르티코 스테로이드 의 사용 등을 제시하고 있다(Table 1). 9)
발병기간 6개월 미만의 조기 류마티스관절염의 치료 지침은 질병 활성도에 따라 나뉘어지는데, 초기에는 methotrexate (MTX)를 우선으로 하는 DMARD 단독 요법이 권고되나 DMARD 단독요법에도 질병 활성도 가 중등도 이상으로 높은 경우에는 DMARDs 다제요 법 또는 TNF 억제제(+/- MTX) 또는 non-TNF bio- logic DMARDs(+/- MTX)의 사용을 강력히 권고하고 있으며 이후에도 질병 활성도가 중등도 이상이면 저용 량의 글루코코르티코이드를 추가하거나 3개월 이내의 단기간 글루코코르티코이드를 사용하도록 제한적으로 권고하고 있다. 9) 발병기간 6개월 이상의 확정 류마티 스관절염 환자의 경우에도 조기 류마티스관절염 환자 와 마찬가지로, 질병 활성도에 따라 약물을 추천하되 질병 활성도가 중등도 이상일 경우 DMARDs 다제요 법 또는 TNF 억제제(+/- MTX) 또는 non-TNF bio- logic DMARDs(+/- MTX) 외에도 tofacitinib(+/- MTX)를 선택할 수 있도록 강력히 권고하고 있다. 이외 에도 질병 활성도가 계속해서 중등도 이상일 경우, 다 Fig. 2 The conversion of plant essential n-6 and n-3 PUFAs to other unsaturated derivatives 5)
DHA, docosahesaenoic acid; EPA, eicosapentaenoic acid
5)른 종류의 TNF 억제제, non-TNF biologic DMARD 제제 또는 tofacitinib 사용과 저용량의 글루코코르티 코이드 또는 3개월 미만의 단기간 글루코코르티코이드 의 추가 사용이 제한적으로 권고되며 관해에 도달했을 경우라 할지라도 약물 감량은 가능하지만, 약물 치료는 지속하도록 강력하게 권고하고 있다. 9)
2. 오메가-3의 항염증작용
오메가-3에서 관찰되는 항염증 효과는 다음과 같은 면역 조절체계와의 관련성에서 찾을 수 있다. 오메가- 3 작용은 먼저 염증부위에서 방출되는 화학물질에 반 응하여 백혈구가 염증활성화 부위로 이동하는 과정인 백혈구의 주화성과 유사한 성향을 가지는 것으로 설명
된다. 10),11) 이때 오메가-3 등을 유인하는 물질을 화학
유인물질(chemo-attractants)이라 명명하며, 그 예 로 아라키돈산(arachidonic acid, AA)에서 파생된 류 코트리엔 B4 (leukotriene B4, LTB4)가 포함된
다. 5),10),11) EPA/DHA의 일일 투여량이 각각 1.3, 4.0,
9.0 g인 세 군으로 구분하여 실험을 진행했을 때, 세 군 모두 호중구의 주화성을 감소시켰다는 Schmidt 등 의 연구 외에, 건강한 사람을 대상으로 EPA/DHA를 매일 3~15 g까지 다양한 용량으로 투여한 여러 임상실 험에서도 유사한 결과를 얻었으며, 그 기전이 명확하진 않으나 화학주성인자와 관련된 수용체에 대한 길항작 용 또는 발현감소에 영향을 미칠 것으로 예측되었 다. 5),10)-12)
오메가-3는 프로스타글란딘(prostaglandins, PGs), 트롬복산(thromboxane, TX), 류코트리엔(leuko- trienes, LTs)과 같은 아이코사노이드(eicosanoid)의 생산을 감소시키는 효과가 있다. 아이코사노이드의 전 구체인 AA은 염증성 자극에 의해 활성화된 포스포리 파아제 A2 (phospholipase A2)에 의해 막인지질로부 터 방출된다. 이것은 시콜로옥시게나아제(cyclo-oxy- genase, COX), 리폭시지네이스(lipoxygenase, LOX), 시토크롬 P450 (cytochrome P450, CYP 450)의 기 질로 작용하여 COX에 의해 PGs와 TX을, LOX에 의 해 LTs를, CYP450에 의해 hydroxyeicosate- Drug category Descriptions
Table 1. Drug categories for the 2015 ACR recommendations (RA treatment) 9)
Methotrexate Oral or SC
DMARDs Traditional/conventional DMARDs (HCQ, LEF, MTX, SSZ) (excludes azathioprine, cyclosporine, minocycline, gold) DMARD monotherapy MTX(preferred), SSZ, HCQ, LEF
Double DMARDs therapy MTX + SSZ, MTX + HCQ, SSZ + HCQ or combinations with LEF Triple DMARDs therapy MTX + SSZ + HCQ
DMARDs combination therapy Double or triple traditional/conventional DMARDs therapy
Tofacitinib Oral
TNF biologics Adalimumab, certolizumab pegol, etanercept, golimumab, infliximab Non-TNF biologics Abatacept, rituximab, tocilizumab (excludes anakinra)
Low-dose glucocorticoid ≤10 mg/day of prednisone (or equivalent)
High-dose glucocorticoid 10 mg/day of prednisone (or equivalent) and up to 60 mg/day with a rapid taper Short-term glucocorticoid 3 month treatment
ACR, American college of rheumatology; RA, rheumatoid arthritis; SC, subcutaneous injection; DMARDs, modifying antirheumatic drugs; HCQ, hydroxy-
chloroquine; LEF, leflunomide; MTX, methotrexate; SSZ, sulfasalazine; TNF, tumor necrosis factor
ARA, arachidonic acid; COX, cyclo-oxygenase; CYP450, cytochrome P450 enzymes; DHET, dihydroxyeicosatrienoic acid; HETE, hydroxyeicosatetraenoic acid; HPETE, hydroperoxyeicosatetraenoic acid; EET, epoxyeicosatrienoic acid; LOX, lipoxygenase; LT, leukotriene; PE, phosphatidyl ethanolamine; PG, prostaglandin; TX, thromboxane
traenoic acid, epoxyeicosatrienoic acid를 생산하게
된다. 5),10),13),14) 이렇게 생산된 아이코사노이드는 G 단백
질 연결 수용체(G protein-coupled receptor, GPCR) 와 같은 특정 수용체를 통해 염증의 조절에 주요한 매 개자 역할을 하는 것으로 알려져 있다(Fig. 3). 5)
실제 한 동물 연구에서 EPA 또는 DHA에 의해 AA에 서 파생된 PGE2와 같은 아이코사노이드의 생산이 감 소된다는 보고가 있었다. 15) 동물 대상으로 진행된 다른 연구에서는 오메가-3의 섭취가 항염증 작용을 나타내 는 것을 보여주었고, 오메가-3가 관절염의 시작을 지 연시키고, 관절염의 정도를 완화시키며, 관절의 병리적 상태를 개선시킨다는 결론을 얻었다. 16),17) 이는 혈중 오 메가-3 농도와 류마티스관절염의 위험률 증가와의 관 계성 확인을 위해 진행한 국내 연구에서도 유사한 결과 로 나타났다. 국내 여성을 대상으로 이루어진 이 연구 에서 생물학적 제제를 제외한 치료 약제를 안정적으로 복용 중인 류마티스관절염 환자군과 건강한 대조군 각 각 100명의 적혈구 내 각종 지방산의 농도를 측정한 결 과 α -linolenic acid, EPA의 적혈구내 농도가 류마티
스관절염과 유의적으로 음의 상관관계를 보이는 것으 로 나타났다. 18) 또한 류마티스관절염 환자의 적혈구내 DHA 농도가 높은 경우 PGE2의 농도가 유의적으로 감소한다는 부가적인 결론도 얻었다. 18) Jiang 등이 수 행한 체계적 문헌 고찰 및 메타분석 연구에서는 염증반 응에 관여하는 물질인 PGE2, TXB2, LTB4의 변화를 확인한 결과, 오메가-3의 복용은 심혈관 질환 고위험 군에서 TXB2 농도를 감소시킨다는 결과와 함께, LTB4가 감소된 환자군의 경우 류마티스관절염 환자가 큰 비중을 차지한다는 분석 결과를 얻었다. 19)
이와 같이 건강한 성인뿐 아니라 류마티스관절염 등 만성 염증성 질환 환자에게도 고용량의 EPA/DHA 섭 취에 의해 PGE2, LTs의 생산이 감소된다는 연구결과 등을 고려할 때 오메가-3는 염증과정에서 한가지 이상 의 여러 단계에 관여할 수 있고, 염증의 진행 및 활성을 억제시키는 것으로 보여진다. 6),17)-19)
이러한 작용기전에 관한 또 다른 근거로서 EPA는
COX, LOX, CYP450의 기질로 작용하지만, AA에서
파생된 아이코사노이드와 구조적으로 다른 매개자를
Fig. 3 The brief pathways of eicosanoid synthesis from arachidonic acid 5)
생산하는 과정으로 설명할 수 있다(Fig. 4). 5) 단, Wada 등의 연구에서 이것의 기능적인 측면은 전형적인 아이 코사노이드 수용체에 대한 낮은 친화력으로 EPA에서 파생된 것은 생물학적 활성이 약하다고 설명하고 있 다. 20)
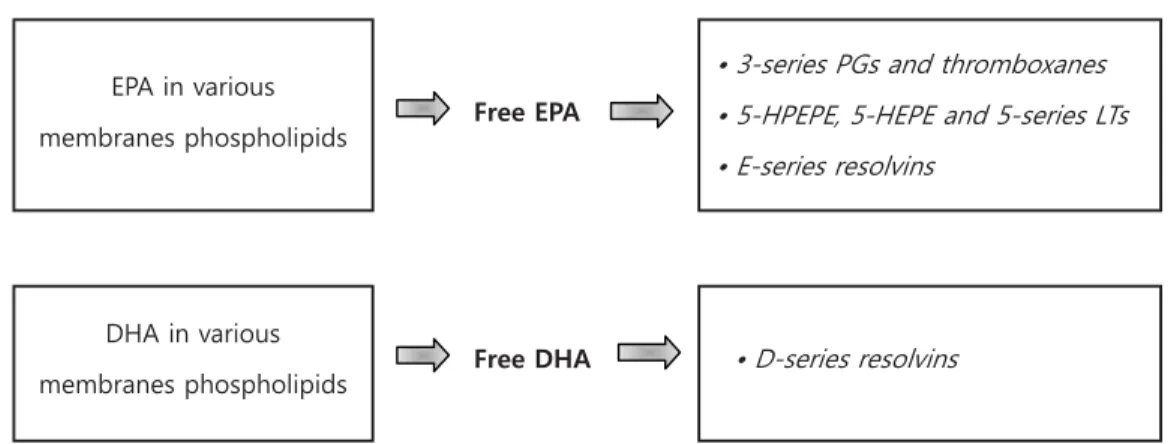
또 다른 항염증 작용 기전으로 EPA와 DHA의 섭취 에 의해 resolvin 합성이 증가하고, DHA에 의해 pro- tectin의 생산이 증가한다는 점을 들 수 있다. 이때 resolvin과 protectin의 생물학적 효과는 항염증작용 과 관련되는데, 이는 동물실험을 통해 resolvin E1, D1, protectin D1은 백혈구의 세포막이동을 억제하고, resolvin D1은 IL-1β 의 생산을 억제하며, protectin D1은 TNF α 와 IL-1β 의 생산을 억제하는 것으로 밝혀 졌다. 5),21)-24)
그 외에도, 오메가-3는 단핵구, 대식세포, 림프구, 내 피세포 표면의 부착 분자 발현을 감소시킨다는 연구 결 과와 함께, EPA와 DHA가 T세포의 증식과 IL-2의 생 산억제에 관여한다고 예상하고 있다. 5)
3. 오메가-3의 통증 억제 작용
오메가-3의 작용기전 중 염증성 시토카인과 아이코 사노이드의 생산을 억제하는 항염증성 활성은 25) 병태 생리학적으로 통증 억제효과와의 상관성을 설명할 수 있다. 그 기전을 살펴보면 염증에 의해 야기되는 중추 감작이 조절됨에 따라 MAP 인산화 효소(mitogen-
activated protein kinase)의 활성이 저해되고 신경성 통증 또는 신경 전달의 경로를 억제하는 효과를 가져오 는 것으로 추정한다. 26) 또한 오메가-3의 일종인 α - linolenic acid가 신경성 통증의 발달에 관여하는 인자 인 리소포스파티드산(lysophosphatidic acid)의 생산 을 억제한다는 보고는 오메가-3와 통증 억제 효과와의 관계를 설명하고 있다. 27),28)
DHA의 경우 용량의존적으로 진통 효과가 있음이 밝 혀졌다. 29) DHA의 물리적, 약학적 기능은 아라키돈산 캐스캐이드의 억제를 통한 항염증효과, 나트륨통로 (sodium channels)의 억제, 염증 발현과 관련된 transient receptor potential vanilloid 1 (TRPV1) 작용 및 칼슘통로 억제 등을 포함한다. 30),31) DHA는 아 편유사제 수용체에 대한 직접작용은 없지만, 내인성 아 편유사제 펩타이드인 β -endorphin의 방출과 관련한 간접적인 작용이 있는 것으로도 추측되고 있으며 이러 한 통증 억제관련 작용 기전을 통해 EPA와 DHA에 의 해 활성화된 G protein-coupled receptor 40 (GPR40), G protein-coupled receptor 120 (GPR120)과 같은 수용체들이 β -endorphin과 같은 아 편유사체 펩타이드의 분비를 조절하여 통증조절에 기 여하는 것으로 추정되기도 한다. 27),32)
DHA와 EPA로부터 파생된 epoxy docosapen- taenoic acid (EpDPE)와 epoxy eicosatetraenoic acid (EpETE) 역시 염증성 통증을 감소시키는 효과가
있다. 27),33) Schwab 등의 연구에서는 염증의 회복과정
Fig. 4 Overview of the lipid mediator synthesis from EPA and DHA 5)
EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid
5)을 활성화시키는 물질로 제시되고 있는 resolvin E1과 protectin D1 성분이, Xu 등의 동물 실험을 통해 염증 성 통증 또한 억제하는 것으로 밝혀지기도 했다. 34),35) 여 기에서는 resolvin 수용체인 chemR23이 활성화되면 서 세포외 신호조절인산화효소(extracellular signal- regulated kinase)의 발현을 억제하고, N-methyl- D-aspartate에 의한 뉴런 자극을 억제한다는 작용 기 전이 제안되고 있다. 35)
4. 류마티스관절염 환자에게 사용된 임상연구
오메가-3를 실제 류마티스관절염 환자에게 사용한 임 상연구 사례는 지속적으로 발표되고 있다(Table 2, 3).
Cleland 등은 발병 1년 이내의 조기 류마티스관절염 환자 중 오메가-3 제제를 3년간 복용한 환자군을 오메 가-3 제제를 복용하지 않은 대조군과 비교했을 때 류 마티스관절염 환자에서 혈중 n-6 지방산과 AA의 감 소, EPA와 DHA의 증가가 관찰되었고, 치료에 있어서 는 NSAID의 사용이 감소되고(75% vs 37%) 관해률이 높았다(72% vs 31%)는 연구결과를 발표하여 조기 류 마티스관절염 환자의 오메가-3 제제 장기 사용에 대한 가능성을 제시했다. 36)
Cleland, L.G., et al., 2006
36)
Open labeled clinical study
� n=31 Fish oil (n=18) vs
No fish oil (n=13)
� 3 years
� 4 to 4.5 g/day
� The plasma concentration of AA was lower in fish oil administered group.
� NSAIDs usage was 75% and 37% reduc- tion from baseline in fish oil adminis- tered group and the control group, respectively.
� At 3 years, the more frequent remission occurs in fish oil administered group (72% vs 31%, p= 0.05).
Reference Study design Subjects Duration & Dose of EPA/DHA
Clinical outcome with EPA/DHA vs Placebo Table 2. Effect of n-3 PUFAs in clinical trials of rheumatoid arthritis (RA) patients
Park, Y., et al., 2013
39)
Double-blind, placebo- controlled, parallel-design multicenter study in Korea
� n=81
n-3 PUFA (n=41) vs placebo (high-oleic-acid sunflower oil, n=40)
� 16 weeks
� EPA 2.090 g + DHA 1.165 g
� n-3 PUFA supplement group had no significant effects in clinical outcomes and NSAID requirements
� RA patient more than 55kg were sig- nificantly reduced NSAID requirements (p=0.043) and LTB4 concentration (p=0.021).
Proudman, S.M., et al., 2015
40)
Randomized, double-blind controlled trial within algorithm-based drug use
� n=139
Fish oil group (n=86) vs
control group (n=53)
� 52 weeks
� 5.5 g/day vs. 0.4 g/day
� The fish oil group was significantly reduced the failure rate of triple DMARD therapy (HRadj = 0.24, 95% CI 0.10 to 0.54, p=0.0006) and increased the rate of ACR remission (HRadj = 2.09, 95% CI 1.02 to 4.30, p=0.04).
* Adjustment factors
: smoking history, shared epitope, baseline anti-cyclic citrullinated peptide
PUFA, polyunsaturated fatty acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; AA, arachidonic acid; NSAID, non-steroidal anti-inflammato-
ry drug; LTB4, leukotriene B4; DMARD=modifying antirheumatic drug; MTX=methotrexate; TNF=tumor necrosis factor; ACR; American College of
Rheumatology
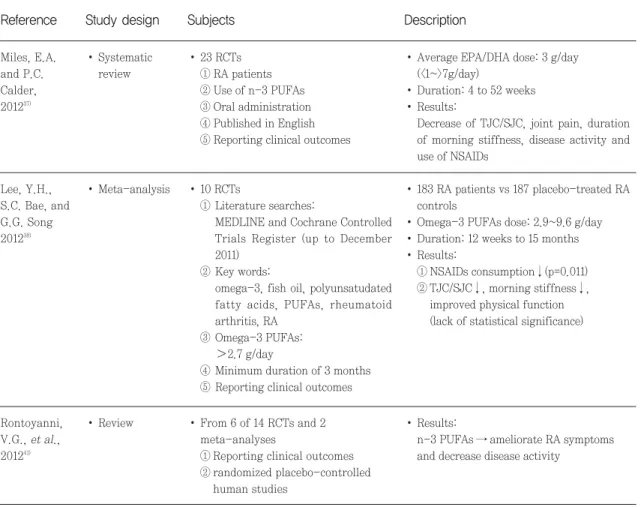
Miles 등이 진행한 체계적 문헌고찰에서는 류마티스 관절염 환자를 대상으로 진행된 오메가-3를 경구 섭취 와 관련된 23개의 무작위대조 임상시험(randomized controlled trials, RCTs)을 분석했다. 4주에서 52주 에 걸친 기간 동안 EPA/DHA은 총 평균 3 g/day (<1~>7 g/day)의 용량 범위로 투여되었다. 임상적 결 과로는 압통관절수(tender joint count, TJC), 부종관 절수(swollen joint count, SJC), 관절통증, 조조강직 의 기간, 질병활성도 및 NSAID의 사용의 감소가 관찰 되었으나 전체적으로는 오메가-3가 류마티스관절염 치료에 있어 약간의 임상적 효과(modest clinical
effects)가 있는 것으로 결론짓고 있으며 이는 오메가- 3의 투여량이나 연구기간, 그리고 대상환자의 연령 등 의 다양성으로 인한 영향으로 예상하고 있다. 37)
Lee 등은 최소 3개월 이상 2.7 g/day 이상의 오메 가-3를 투여받은 류마티스관절염 환자의 임상 효과에 대해서 평가하고자 10개의 RCTs를 대상으로 오메가- 3 투여군 183명과 대조군 187명에 대한 메타분석을 실 시하였다. 38) 그 결과 오메가-3 투여량은 2.9~9.6 g/day, 투여기간은 12주에서 15개월이었으며, 2개의 연구 결과를 통해 NSAID의 사용량이 유의적으로 감소 했음이 확인되었고(p=0.011), 그 외 TJC/SJC, 조조강
Miles, E.A.and P.C.
Calder, 2012
37)
� Systematic review
� 23 RCTs
① RA patients
② Use of n-3 PUFAs
③ Oral administration
④ Published in English
⑤ Reporting clinical outcomes
� Average EPA/DHA dose: 3 g/day (<1~>7g/day)
� Duration: 4 to 52 weeks
� Results:
Decrease of TJC/SJC, joint pain, duration of morning stiffness, disease activity and use of NSAIDs
Lee, Y.H., S.C. Bae, and G.G. Song 2012
38)
� Meta-analysis � 10 RCTs
① Literature searches:
MEDLINE and Cochrane Controlled Trials Register (up to December 2011)
② Key words:
omega-3, fish oil, polyunsatudated fatty acids, PUFAs, rheumatoid arthritis, RA
③ Omega-3 PUFAs:
2.7 g/day
④ Minimum duration of 3 months
⑤ Reporting clinical outcomes
� 183 RA patients vs 187 placebo-treated RA controls
� Omega-3 PUFAs dose: 2.9~9.6 g/day
� Duration: 12 weeks to 15 months
� Results:
① NSAIDs consumption↓(p=0.011)
② TJC/SJC↓, morning stiffness↓, improved physical function (lack of statistical significance)
Reference Study design Subjects Description
Table 3. Effect of n-3 PUFAs in systematic review or meta-analysis of rheumatoid arthritis (RA) patients
Rontoyanni, V.G., et al., 2012
41)
� Review � From 6 of 14 RCTs and 2 meta-analyses
① Reporting clinical outcomes
② randomized placebo-controlled human studies
� Results:
n-3 PUFAs → ameliorate RA symptoms and decrease disease activity