PGHN
Original Article
Outcome of Alagille Syndrome Patients Who Had Previously Received Kasai Operation during Infancy: A Single Center Study
Hwa Pyung Lee, Ben Kang, So Yoon Choi, Sanghoon Lee*, Suk-Koo Lee*, and Yon Ho Choe
Departments of Pediatrics and *Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Purpose: Infants with Alagille syndrome (AGS) are occasionally misdiagnosed as biliary atresia and subsequently undergo Kasai operation. The purpose of this study was to investigate the outcome of patients with AGS who had previously received Kasai operation during infancy.
Methods: This retrospective study was conducted at the Department of Pediatrics, Samsung Medical Center. We compared the prognosis and mortality between those who had undergone Kasai operation during infancy (Kasai group) and those who had not (non-Kasai group).
Results: Among the 15 children with AGS, five had received Kasai operation, while 10 had not. All subjects in the Kasai group revealed neonatal cholestasis, while 70% of the non-Kasai group showed neonatal cholestasis. Liver transplantation was performed in 100% (5/5) among the Kasai group, and 20.0% (2/10) among the non-Kasai group (p=0.007). Mortality was observed in 60.0% (3/5) among the Kasai group, and 10.0% (1/10) among the non-Kasai group (p=0.077).
Conclusion: Although overall mortality rate did not significantly differ between the two groups, the proportion of pa- tients receiving liver transplantation was significantly higher in the non-Kasai group. The relatively worse outcome in AGS patients who had received Kasai operation may be due to the unfavorable influences of Kasai operation on the clinical course of AGS, or maybe due to neonatal cholestasis, irrespective of the Kasai operation.
Key Words: Alagille syndrome, Kasai operation, Cholestasis, Liver transplantation
Received:February 5, 2015, Revised:July 2, 2015, Accepted:July 21, 2015
Corresponding author: Yon Ho Choe, Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea. Tel: +82-2-3410-3527, Fax: +82-2-3410-0043, E-mail: i101016@skku.edu
Copyright ⓒ 2015 by The Korean Society of Pediatric Gastroenterology, Hepatology and Nutrition
This is an openaccess article distributed under the terms of the Creative Commons Attribution NonCommercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Alagille syndrome (AGS) is a complex autosomal dominant disorder due to defects in the Notch sig-
naling pathway, and is characterized by paucity of the intrahepatic bile ducts, cholestasis, congenital heart defects, dysmorphic facies, and skeletal and eye anomalies [1]. The clinical diagnosis of AGS has
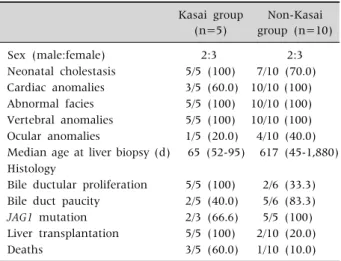
Table 1. Characteristics and Prognosis of Alagille Syndrome Patients
Kasai group (n=5)
Non-Kasai group (n=10)
Sex (male:female) 2:3 2:3
Neonatal cholestasis 5/5 (100) 7/10 (70.0) Cardiac anomalies 3/5 (60.0) 10/10 (100) Abnormal facies 5/5 (100) 10/10 (100) Vertebral anomalies 5/5 (100) 10/10 (100) Ocular anomalies 1/5 (20.0) 4/10 (40.0) Median age at liver biopsy (d) 65 (52-95) 617 (45-1,880) Histology
Bile ductular proliferation 5/5 (100) 2/6 (33.3) Bile duct paucity 2/5 (40.0) 5/6 (83.3) JAG1 mutation 2/3 (66.6) 5/5 (100) Liver transplantation 5/5 (100) 2/10 (20.0)
Deaths 3/5 (60.0) 1/10 (10.0)
Values are presented as number only, number (%), or median (range).
been based on the classic criteria established by Alagille et al. [2], which requires a minimum of 3 out of 5 major clinical features; chronic cholestasis due to bile duct paucity, congenital heart disease (most commonly peripheral pulmonary artery stenosis), vertebral anomalies (butterfly vertebrae), ocular anomalies (posterior embryotoxon), and the abnor- mal facies (recognizable dysmorphic features).
The most common initial presenting sign of AGS in infancy is conjugated hyperbilirubinemia, which can be difficult to distinguish from other causes of obstructive cholestasis, especially biliary atresia [3].
A liver biopsy, no longer mandatory if cholestasis is present, typically shows paucity of the intrahepatic bile ducts. However, in infancy ductal proliferation may occasionally be seen, usually with portal in- flammation, which may lead to a misdiagnosis of biliary atresia and subsequently receive Kasai oper- ation [4]. Kasai operation in AGS results in sig- nificant hepatic morbidity due to profound choles- tasis and is an important indication for liver trans- plantation [3].
The aim of this study was to evaluate the clinical features and outcomes of patients with AGS who had previously received Kasai operation during in- fancy by comparison with those who had not.
MATERIALS AND METHODS
The medical records of 15 patients diagnosed with AGS and followed at the Department of Pediatrics, Samsung Medical Center (Seoul, Korea) between 1999 and 2014 were retrospectively reviewed. The di- agnosis of AGS required at least three of the five ma- jor clinical features; chronic cholestasis, congenital heart disease, “butterfly-like” vertebrae, posterior embryotoxon, and peculiar faces, or JAG1 gene mutation. Complex intracardiac disease was defined as a need for intervention or the critical condition having heart failure, hypoxemia, or hemodynamic instability [4].
Patients were divided into two groups according to whether they had received Kasai operation during infancy. Patients who had received Kasai operation
during infancy were included in the “Kasai group”, and those who had not received Kasai operation were included in the “non-Kasai group”. We com- pared the clinical features, prognosis, and mortality of the patients in the two groups. Comparison be- tween the two groups was conducted by the Fisher’s exact test using the IBM SPSS Statistics ver. 22.0 for Windows (IBM Co., Armonk, NY, USA). This study was approved by the institutional review board of Samsung Medical Center (2015-01-060-001).
RESULTS
Fifteen patients were diagnosed with AGS (Table 1).
Kasai operation had been conducted in five patients (33.3%). JAG1 gene analysis was performed in eight subjects, and gene mutations were detected in seven of them (87.5%).
All of the patients in the Kasai group had neo- natal cholestasis (100%), while seven patients in the non-Kasai group revealed neonatal cholestasis (70.0%). The five patients in the Kasai group had been initially misdiagnosed as biliary atresia. Three of the five subjects (60.0%) had received Kasai oper- ation at other hospitals. They were later referred to our hospital and diagnosed as AGS. The median age
at liver biopsy for the Kasai group was 65 days (range, 52-95 days), whereas for the non-Kasai group it was 617 days (range, 45-1,880 days).
Histologic findings on liver biopsy specimens re- vealed bile duct paucity in 2 out of 5 patients (40.0%) in the Kasai group, and in 5 out of 6 patients (83.3%) in the non-Kasai group. Bile ductule proliferation was observed in all of the subjects (100%) in the Kasai group, and in 2 out of 6 subjects (33.3%) of the non-Kasai group. Intraoperative cholangiogram was performed in two patients in the Kasai group, who had received Kasai operation at our hospital due to findings consistent with extrahepatic biliary atresia.
Medical records lacked information of the other three patients in whom Kasai operation was con- ducted at other hospitals. One patient in the non-Kasai group did not proceed to receive Kasai op- eration as findings on intraoperative cholangiogram were inconsistent with biliary atresia.
The median follow-up duration of all AGS patients was 528 days (range, 94-5,723 days). One patient (20.0%) in the Kasai group and four patients (40.0%) in the non-Kasai group had complex intracardiac diseases (33.3%). The patient in the Kasai group re- ceived balloon dilatation due to pulmonary stenosis.
Among the non-Kasai group, two patients received closure operation for patent ductus arteriosus, one patient underwent angioplasty due to stenosis of left and right pulmonary arteries, and one patient re- ceived coarctoplasty due to coarctation of the aorta.
None of the patients with complex intracardiac dis- eases died during or after cardiac interventions or surgeries. Liver transplantation was performed in 100% (5/5) among the Kasai group, and 20.0% (2/10) among the non-Kasai group (p=0.007). Mortality was observed in 60.0% (3/5) among the Kasai group, and 10.0% (1/10) among the non-Kasai group (p=0.077). All of the patients in the Kasai group eventually received liver transplantation at the me- dian ages of 12 months (range, 7-29 months). The indications for liver transplantation were refractory pruritus and xanthomas, biliary cirrhosis, somatic growth retardation and development delay. Refrac- tory pruritus and xanthoma were present in all of the
five children (100%), and biliary cirrhosis in two pa- tients (40.0%). Two patients (40.0%) revealed so- matic growth retardation and developmental delay.
Three (60.0%) died in the Kasai group. Two of the mortalities were due to acute rejection leading to liv- er failure, the 15 days after cadevouric donor liver transplantation, and 13 days after living related liver transplantation, respectively. One was due to in- tra-abdominal hemorrhage on the following day of surgery. In the non-Kasai group, two patients (20.0%) underwent liver transplantation due to refractory pruritus and xanthomas at ages of 33-month-old and 10-month-old, respectively. One (10.0%) died of mul- tiorgan failure after the seventh day of surgery. The surviving patients are currently well without serious complications.
DISCUSSION
We have compared the clinical features and out- comes between the patients with and without a his- tory of Kasai operation. The results or our study show that all of the patients with a history of Kasai oper- ation had ultimately received liver transplantation in the future. The percentage of liver transplantation was relatively higher in those who had received Kasai operation in infancy compared to those who had not (100% vs. 20.0%), leading to a relatively higher overall mortality rate (60.0% vs. 10.0%). Our study is the first in Korea to compare the outcome of AGS between patients who had previous received Kasai operation during infancy and those who had not.
According to previous studies, the presence of clin- ical features in AGS are diverse, showing a bile duct paucity of 75-100%, cholestasis of 83-100%, con- genital heart diseases of 85-98%, butterfly vertebrae of 32-87%, peculiar facies of 70-98%, ocular anoma- lies of 30-88% [2,5-10]. Compared to these previous studies, bile duct paucity was less frequently de- tected in our study, while the prevalence of vertebral and facial anomalies was relatively higher in our study. The relatively lower frequency of bile duct paucity in our study may have been due to those in
the Kasai group because liver biopsy was performed in early infant period, leading to a misdiagnosis of biliary atresia.
Bile duct paucity is not present on initial biopsy in patients with AGS in early infant period, and initial findings may actually reveal bile duct proliferation leading to a misdiagnosis of biliary atresia [4]. One study that investigated serial liver biopsies in AGS patients demonstrated that bile duct paucity is more common in older infants and children rather than those of younger age [7]. Emerick et al. [7] found that bile duct paucity was present in only 60% of 48 AGS infants under 6 months of age, while it was ob- served in 95% of 40 patients who underwent biopsy after 6 months of age. Meanwhile, Kaye et al. [3] re- ported that bile duct proliferation was more fre- quently detected in children with AGS who had re- ceived Kasai operation, while bile duct paucity was more prevalent among AGS patients who had not re- ceived Kasai operation, which correlates with the findings of our study. Explorative laparotomy with intraoperative cholangiography should be under- taken by an experienced surgeon and careful inter- pretation of an intraoperative cholangiography is necessary before proceeding with a Kasai operation.
The correlation of Kasai operation and prognosis in AGS has been investigated in several studies [3,6].
Kaye et al. [3] reported that compared to AGS chil- dren who had not received Kasai operation, those who had demonstrated a significantly higher rate of liver transplantation (47.3% vs. 13.9%) and higher mortality (31.6% vs. 2.8%) in the future. Hoffenberg et al. [6] reported that the liver transplantation rate in AGS patients who had previously undergone Kasai operation was higher than that of non-Kasai patients (75% vs. 23%).Our results are consistent with these previous reports, in which suggests that Kasai operation does not benefit but rather worsens the clinical course of AGS patients. This may be due to exposure to intestinal contents and/or ascending cholangitis via the portoenterostomy deteriorating the status of formerly abnormal bile ducts, or the procedure itself may exert direct detrimental effects on the disease [3]. Emerick et al. [7] reported that
approximately 15% of AGS patients required liver transplantation due to progressive liver diseases, cir- rhosis, and failure. The most common indications for liver transplantation in the AGS population were persistent cholestasis leading to severe pruritus and xanthomata, recurrent and poorly healing bone frac- tures, end-stage liver disease, and portal hypertension with gastrointestinal bleeding [6,7]. Liver transplan- tation is known as a good treatment option for AGS patients with progressive cholestasis and end-stage liver diseases [11]. The 5-year survival rate following transplantation has been reported to improve up to 80% [12]. Therefore, AGS patients with neonatal cholestasis may rather benefit from liver trans- plantation in the future when their disease status progresses to biliary cirrhosis and end-stage liver dis- eases, instead of Kasai operation during infancy.
Parental mosaicism of JAG1 mutations in families with AGS has been reported and may produce bile duct paucity in donor candidates [12]. It may be helpful to conduct genetic analysis for JAG1 muta- tion in donors of family members of AGS, who reveal a normal phenotype.
Neonatal cholestatic jaundice has been reported as an independent prognostic factor in AGS [13].
According to the study of Lykavieris et al. [13], mul- tivariate analysis of prognostic factors of 10 year sur- vival with native liver in AGS patients revealed that neonatal cholestatic jaundice was the only inde- pendent prognostic factor (relative risk [RR], 2.52;
95% confidence interval [CI], 1.25-5.88; p=0.012), while a history of no Kasai operation was not (RR, 0.65; 95% CI, 0.35-1.21; not significant). These re- sults suggest that the presence of neonatal choles- tasis itself may negatively affect the course in AGS, irrespective of the history of Kasai operation. The presence of complex intracardiac disease, which has been defined as a need for intervention or the critical condition having heart failure, hypoxemia, or hemo- dynamic instability has been suggested as the most significant indicator of early mortality [4,7,10].
However, we were unable to observe this subgroup of poor outcome due to cardiac origin in our study.
There are several limitations of this study. First,
there is the possibility that patients in the Kasai group reflect a subgroup of AGS patients with neo- natal cholestatic jaundice predestinated to progress to an end-stage liver disease, regardless of the Kasai operation they had received. The presence of neo- natal cholestatic jaundice itself may have led to un- favorable courses in the Kasai group. In the neonatal period, AGS patients are likely to not present with all clinical features of AGS. This may lead to the mis- diagnosis of biliary atresia instead of AGS. The diffi- culty of diagnosing AGS at early infancy lies in the variable expression of clinical features at this period.
Moreover, genetic analysis itself is insufficient for determining the diagnosis as JAG1 mutation gene analysis is incapable of diagnosing all cases of AGS.
Second, there are limitations in concluding that Kasai operation during infancy leads to a harmful clinical course in AGS patients, due to the small number of subjects in our study. Further large-scale prospective studies are required in the future.
In summary, our study shows the future outcomes of AGS patients who had received Kasai operation during infancy. The results of our study highlight the importance of differentiating AGS from other causes of neonatal cholestasis, especially biliary atresia, as inappropriate surgical intervention may worsen the outcome. Thorough medical investigation with par- ticular consideration of AGS is essential for the pe- diatrician to identify subclinical features in patients with conjugated hyperbilirubinemia in the early in- fantile period.
REFERENCES
1. Vajro P, Ferrante L, Paolella G. Alagille syndrome: an overview. Clin Res Hepatol Gastroenterol 2012;36:
275-7.
2. Alagille D, Estrada A, Hadchouel M, Gautier M, Odièvre M, Dommergues JP. Syndromic paucity of in-
terlobular bile ducts (Alagille syndrome or arterio- hepatic dysplasia): review of 80 cases. J Pediatr 1987;
110:195-200.
3. Kaye AJ, Rand EB, Munoz PS, Spinner NB, Flake AW, Kamath BM. Effect of Kasai procedure on hepatic out- come in Alagille syndrome. J Pediatr Gastroenterol Nutr 2010;51:319-21.
4. Turnpenny PD, Ellard S. Alagille syndrome: patho- genesis, diagnosis and management. Eur J Hum Genet 2012;20:251-7.
5. Deprettere A, Portmann B, Mowat AP. Syndromic paucity of the intrahepatic bile ducts: diagnostic diffi- culty; severe morbidity throughout early childhood. J Pediatr Gastroenterol Nutr 1987;6:865-71.
6. Hoffenberg EJ, Narkewicz MR, Sondheimer JM, Smith DJ, Silverman A, Sokol RJ. Outcome of syndromic pauc- ity of interlobular bile ducts (Alagille syndrome) with onset of cholestasis in infancy. J Pediatr 1995;127:
220-4.
7. Emerick KM, Rand EB, Goldmuntz E, Krantz ID, Spinner NB, Piccoli DA. Features of Alagille syndrome in 92 patients: frequency and relation to prognosis.
Hepatology 1999;29:822-9.
8. Quiros-Tejeira RE, Ament ME, Heyman MB, Martin MG, Rosenthal P, Hall TR, et al. Variable morbidity in alagille syndrome: a review of 43 cases. J Pediatr Gastroenterol Nutr 1999;29:431-7.
9. Subramaniam P, Knisely A, Portmann B, Qureshi SA, Aclimandos WA, Karani JB, et al. Diagnosis of Alagille syndrome-25 years of experience at King's College Hospital. J Pediatr Gastroenterol Nutr 2011;52:84-9.
10. Ahn KJ, Bae EJ, Yoon JK, Kim GB, Kwon BS, Moon JS, et al. Alagille syndrome and a JAG1 mutation: 41 cases of experience at a single center. Korean J Pediatr 2014.
[Epub ahead of print]
11. Ganschow R, Grabhorn E, Helmke K, Rogiers X, Burdelski M. Liver transplantation in children with Alagille syndrome. Transplant Proc 2001;33:3608-9.
12. Kasahara M, Kiuchi T, Inomata Y, Uryuhara K, Sakamoto S, Ito T, et al. Living-related liver transplan- tation for Alagille syndrome. Transplantation 2003;75:
2147-50.
13. Lykavieris P, Hadchouel M, Chardot C, Bernard O.
Outcome of liver disease in children with Alagille syn- drome: a study of 163 patients. Gut 2001;49:431-5.
![[ 갑상선암 ]](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)