Lipomas are common mesenchymal tumors that can be easily diagnosed based on their characteristic imag- ing findings, including the presence of an attenuation unit between -65 and -120 on computed tomography and the observation of the same signal intensity as that of subcutaneous fat on all pulse sequences of magnetic resonance (MR) imaging. Lipomas usually exhibit well- defined margins and are localized within a compart- ment of the involved structure. However, some lipomas such as intramuscular lipoma, angiolipoma, or neural fi- brolipoma may sometimes have irregular margins (1, 2).
Even these lipomas are usually localized within the compartment. The term “hernia” refers to a condition in which a part of a body organ or tissue protrudes through a weak opening in its surrounding walls. To the best of our knowledge, there has been no radiology report de-
scribing the imaging features of a herniated soft tissue lipoma.
Here, we report the MR image findings of 3 cases of herniated lipomatous tumor in the extremity.
Case Report
Case 1
A 29-year-old man presented with a protruded soft tis- sue mass in the lateral knee joint area; the mass had per- sisted for 6 years. There was no history of trauma.
Although there was no pain at the lesion site, applica- tion of compression on the tumor resulted in pain along the lateral side of the knee joint. MR images revealed a well-defined outwardly protruding fatty mass in the subcutaneous fat layer. The size of this tumor was 4.6×
1.3×2.2 cm (longitudinal diameter [L]×transverse di- ameter [T]×anteroposterior diameter [AP]). This fatty mass contained hypointense, nodular, and septal non- fatty areas that did not enhance following contrast ad- ministration. On a fat-suppressed T2-weighted image, the protruded portion of the tumor appeared hyperin- tense, whereas the other portion exhibited suppressed
Herniation of a Lipomatous Tumor in the Extremity:
A Report of 3 Cases
1Jee Young Kim, M.D.
1Department of Radiology, St. Vincent’s Hospital, The Catholic University of Korea.
Received May 14, 2007 ; Accepted July 6, 2007
Address reprint requests to : Jee Young Kim, M.D., Department of Radiology, St. Vincent’s Hospital, The Catholic University of Korea, 93-6 Chi-dong, Paldal-gu, Suwon, Gyeonggi-do 442-723, Republic of Korea.
Tel. 82-31-249-8493 Fax. 82-31-247-5713 E-mail: [email protected]
Lipomas can occur in any soft tissue, including that found in bone. Although it is known that most lipomas are restricted to the involved compartment, we found some lipomas that herniated across the compartment barrier. Here, we report 3 cases of a herniated soft tissue lipomatous tumor. Radiological findings of the herniated lipomas indicated the presence of a waist portion, and the associated findings were related to a focal ischemic change.
Index words :Lipoma Extremities Hernia
Magnetic resonance imaging (MRI)
signal intensity (Fig. 1A-F). After surgery, this tumor was pathologically diagnosed as a fibrolipoma (Fig. 1G).
Case 2
A 34-year-old woman presented with a palpable mass on the volar aspect of the right hand; the mass had per-
sisted for 8 months. Compression of the tumor resulted in pain. MR images showed a well-defined fatty mass in the subcutaneous fat layer. This mass had herniated through a defect in the palmar aponeurosis, and it mea- sured 1.7×1.8×1.2 cm (L×T×AP). It contained several small nodular non-fatty areas that were eccentrically lo-
A B C
D E F
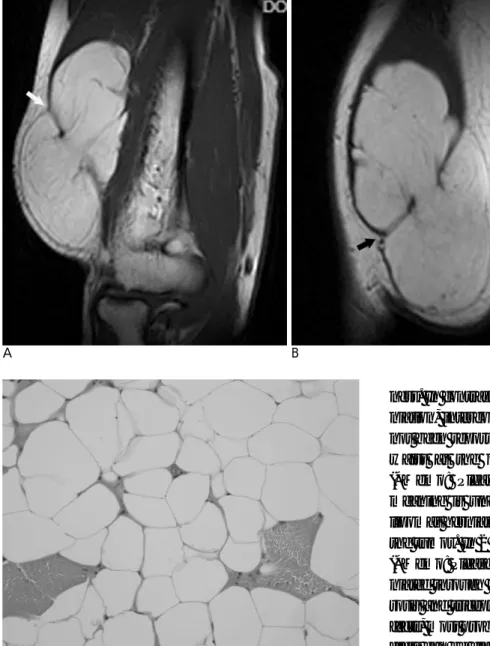
Fig. 1. A 29-year-old man with a fibrolipoma.
A, B. Coronal spin-echo T1-weighted MR images show a well- defined fatty mass with hypointense, nodular, and septal non- fatty areas (arrow) in the subcutaneous fat layer. This mass pro- truded outward (arrow).
C, D. Axial spin-echo T2-weighted images show an ovoid fatty mass (arrow) in the subcutaneous fat layer; the mass protruded outward (arrow).
E. Coronal fast-spin-echo T2-weighted image with fat suppres- sion shows the hyperintense protruded portion of the tumor (ar- row).
F. Coronal post-contrast T1-weighted image shows no signifi- cant enhancement in the tumor (arrow).
G. Photomicrograph of the histological specimen (original mag-
cated. The non-fatty areas appeared hypointense on T1- weighted images, hyperintense on T2-weighted images, and well enhanced on contrast-enhanced images. A gadolinium-enhanced T1-weighted image with fat sup- pression showed faint enhancement in the herniated and the waist portions of the tumor (Fig. 2A-D). This tumor was definitively diagnosed as an angiolipoma af-
ter surgery (Fig. 2E).
Case 3
A 54-year-old man presented with a large palpable mass in the arm; the mass had persisted for 30 years.
Recently, he experienced numbness in the hand.
Clinical examination revealed hypoesthesia in the hand,
A B
C D
E
Fig. 2. A 34-year-old woman with an angiolipoma.
A. Coronal spin-echo T1-weighted MR image shows an ovoid fatty mass with hypointense, nodular, non-fatty areas (arrow) in the subcutaneous fat layer.
B. Axial spin-echo T2-weighted image shows focal herniation of the fatty mass through the palmar aponeurosis defect (arrow).
C, D. Axial post-contrast T1-weighted images with fat suppres- sion show nodular enhancement (arrow) of the non-fatty areas.
There is faint focal enhancement in the herniated portion of the tumor (arrow).
E. Photomicrograph of the histological specimen (original mag- nification, ×40; H & E stain) shows scattered capillary vessels in the adipose tissue.
excluding the thumb. MR images showed an intramus- cular fatty mass that had herniated to the subcutaneous fat layer through a defect in the muscular fascia (Fig. 3A, B). The size of this mass was 9.5×5.4×4.6 cm (L×T×
AP). This tumor contained non-fatty areas comprising only thin, smooth, and hypointense septa. After surgery, the mass was diagnosed as an intramuscular lipoma (Fig. 3C).
Discussion
Muscle herniation is common in the musculoskeletal
ness. In contrast to the commonly occurring muscle her- niation, intercompartmental herniation of a lipoma has not been reported. All our cases described above had a waist at the opening site of herniation.[Editor 1]
(*Memo: Please rewrite this sentence because the meaning is unclear in the present construction.) The lipomas herniated irrespective of the size and location of the tumor. In 2 of our patients (Cases 2 and 3)[Editor 2], (*Memo: Please check the change.) the lipomas had her- niated through the fascial defects in the palmar aponeu- rosis and triceps. We believe that pre-existing fascial de- fects, most probably, led to these herniations. Fascial de- fects can be classified as traumatic or constitutional (7).
Traumatic defects can be direct or indirect, resulting from a blow to the contracted muscle. Constitutional de- fects are either congenital or secondary to vigorous exer- cise that leads to muscle hypertrophy and elevated intra- compartmental pressure.
In Case 1, the lipoma had herniated to the skin;
(*Memo: This information should preferably be provid- ed in the respective case description.) this occurred probably due to the weakness of the supporting connec- tive tissue of the subcutaneous fat layer.
According to other reports, signal intensity and en- hancement patterns of non-fatty areas of lipomas have been used to identify component tissues such as vessels, fibrous tissue, muscles, and focal fat necrosis on MR im-
A B
Fig. 3. A 54-year-old man with an in- tramuscular lipoma.
A, B. Coronal (A) and sagittal (B) spin- echo T1-weighted MR images show a lobulated fatty mass that has herniated to the subcutaneous fat layer through the fascia defect (arrow) in the triceps muscle.
C. Photomicrograph of the histological specimen (original magnification, × 400; H & E stain) shows adipose tissue that has infiltrated in the skeletal mus- cle, suggesting an intramuscular lipo- ma.
C
fined change in signal intensity in the waist and herniat- ed portions of the tumors. We speculate that this finding suggests either an edematous change due to the is- chemia resulting from pressure in the waist portion of the tumor or focal fat necrosis induced by ischemia of a long duration, which was not observed in the 2 cases.[Editor 5] (*Memo: If the reference is to Cases 1 and 2, please revise the phrase as “in the 2 cases.
Further, please check the changes made in the entire sentence.) In these 2 patients who complained of pain when the tumor was compressed, the pain may be relat- ed to the edematous change. In Case 3, numbness may not be directly related to tumor herniation, but may be related to nerve compression by the enlarged tumor. It is well known that non-fatty areas such as septa play an important role in differentiating between classic lipoma and well-differentiated liposarcoma (8-10). In our cas- es, it was easy to differentiate the lipomas from liposar- coma because the image findings of the non-fatty areas of the lipomas were distinctly different from those of a liposarcoma.
In conclusion, lipoma occasionally herniates through a fascial defect or loosened supporting connective tissues in the subcutaneous fat layer. This phenomenon may occur due to a congenital defect or traumatic change.
Herniation leads to the development of a waist portion in the lipoma and occasionally decreases the blood flow due to compression, leading to a focal ischemic change.
Although this ischemic change in the lipoma appears as an abnormal signal change on MR imaging, the imaging
finding is clearly different from that associated with a li- posarcoma.
References
1. Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. Benign musculoskeletal lipomatous lesions.
Radiographics 2004;24:1433-1466
2. Matsumoto K, Hukuda S, Ishizawa M, Chano T, Okabe H. MRI findings in intramuscular lipomas. Skeletal Radiol 1999;28:145-152 3. Kendi TK, Altinok D, Erdal HH, Kara S. Imaging in the diagnosis
of symptomatic forearm muscle herniation. Skeletal Radiol 2003;32:364-366
4. Beggs I. Sonography of muscle hernias. AJR Am J Roentgenol 2003;180:395-399
5. Zeiss J, Ebraheim NA, Woldenberg LS. Magnetic resonance imag- ing in the diagnosis of anterior tibialis muscle herniation. Clin Orthop Relat Res 1989;244:249-253
6. Mellado JM, Perez del Palomar L. Muscle hernias of the lower leg:
MRI findings. Skeletal Radiol 1999;28:465-469
7. Bates DG. Dynamic ultrasound findings of bilateral anterior tib- ialis muscle herniation in a pediatric patient. Pediatr Radiol 2001;31:753-755
8. Hosono M, Kobayashi H, Fujimoto R, Kotoura Y, Tsuboyama T, Matsusue Y, et al. Septum-like structures in lipoma and liposarco- ma: MR imaging and pathologic correlation. Skeletal Radiol 1997;26:150-154
9. Kransdorf MJ, Bancroft LW, Peterson JJ, Murphey MD, Foster WC, Temple HT. Imaging of fatty tumors: distinction of lipoma and well-differentiated liposarcoma. Radiology 2002;224:99-104 10. Ohguri T, Aoki T, Hisaoka M, Watanabe H, Nakamura K,
Hashimoto H, et al. Differential diagnosis of benign peripheral lipoma from well-differentiated liposarcoma on MR imaging: is comparison of margins and internal characteristics useful? AJR Am J Roentgenol 2003;180:1689-94
대한영상의학회지 2007;57:175-179
사지에 발생한 지방종 헤르니아: 증례 보고1
1가톨릭대학교 의과대학 성빈센트병원 영상의학과
김 지 영
지방종은 흔한 양성 종양중 하나로 발생시 조직내 국한되어 있는 것이 일반적인 소견이다. 이제까지 지방종이 주 변 방어장벽을 뚫고 탈출한 사례가 보고된 바가 없으며, 이에 본 저자는 주변 격막을 뚫고 헤르니아를 가져온지방 종 3예를 경험하였기에 보고하고자 한다.