Address reprint requests to Join-Seok Bae, M.D.
Department of Neurology, Kangdong Sacred Heart Hospital 150, Seongan-ro, Gangdong-gu, Seoul 134-701 TEL: 82-2-2224-2854 FAX: 82-2-2224-2854, E-mail: [email protected]
투고일: 2014년 6월 3일, 게재확정일: 2014년 6월 3일
서 론
길랭-바레증후군(Guillain-Barré syndrome, GBS) 은 감염 후 급성의 이완성 마비가 단상성으로 발생하는 급성 면역매개성 말초신경병증이다. 전통적으로 GBS의 특징적 세 징후는 상행성 마비, 심부건 반사의 소실, 및 알부민세포해리(albuminocytologic dissociation) 로 알려져 있다.1-4 하지만 근래에 규명된 다양한 GBS 의 임상적 스펙트럼들에서 항상 이 세 징후가 나타나는
것은 아니다. 예를 들면, 10%의 GBS 환자는 심부건 반사가 정상이거나 오히려 증가된 경우도 있다.5 상행성 마비 역시 뇌신경 증상이 주인 GBS 아형들에서는 맞지 않는 개념이라 할 수 있다. 그럼에도 불구하고 기존의 GBS 진단 기준은 전통적인 개념에 머물러있다고 할 수 있다.6-8 처음에 GBS는 병리학적으로 탈수초성 말초신 경병으로 알려져 왔고 따라서 오랫동안 급성염증성탈수 초다발신경근병증(acute inflammatory demyeli- nating polyradiculoneuropathy, AIDP)이 GBS의
길랭-바레 증후군의 임상적 스펙트럼
한림대학교 의과대학 신경과학교실, 동아대학교 의과대학 신경과학교실�
배종석∙김종국�
– Abstract –
Clinical Spectrum of Guillain-Barré Syndrome
Join-Seok Bae, M.D., Jong Kuk Kim, M.D. *
Department of Neurology, Hallym University College of Medicine, Department of Neurology, Dong-A University College of Medicine
*Guillain-Barré syndrome (GBS) is an acute post-infectious, immune-mediated peripheral neuropathy pre- senting with various clinical and electrophysiological features. Over the past 20 years, the concept of this syndrome was considerably changed. The classical triad of GBS
-ascending paralysis, areflexia, and albumin-cytological dissociation
-are not always essential in current diagnosis of GBS. From a clinical view, recently GBS can be arbitrarily categorized as “typical type” (acute inflammatory demyelinating polyneuropathy, acute motor axonal neuropathy, or acute motor sensory axonal neuropathy) and “variant type” (Fisher syndrome, Bickerstaff’s brainstem encephalitis, pharyngeal-cervical-brachial type, and sen- sory or ataxic variants, etc.). Clinicians need to be familiar with typical clinical features of GBS and have full knowledge about various clinical spectrum of GBS variants. This article briefly review regarding these issues focusing on the recent literature and provide some clues for the better understanding of over- all clinical spectrums of GBS.
Key Words: Guillain-Barré syndrome (GBS), Clinical, Variant
동의어처럼 사용되었다.2,4 하지만 최초로 축삭형 GBS 존재 가능성이 제시된 후,9 1990년대에는 GBS의 새로 운 아형으로서 급성운동축삭신경병증(acute motor axonal neuropathy, AMAN)이 정의되었다. 이후 AMAN은 주로 중국, 일본 등의 동아시아 지역에서 계 속 보고되어왔는데,2,4,10-12 현재 병리적, 면역학적, 및 신 경생리학적으로 AIDP와 확연히 구분되는 질환으로 인 정 받게 되었다. 따라서 AIDP는 GBS의 한 아형일 뿐 더 이상 동의어로 사용되지 않는다.1,4,12 이와 같이 팔 다리에 주 증상을 나타내는 전형적 양상의 GBS은 병태 생리학적으로 탈수초형과 축삭형으로 구분되었다면 Fisher 증후군(Fisher syndrome, FS)으로 대표될 수 있는 GBS의 비전형적 아형들이 다양한 국소성 증후 군 형태로 계속 보고되고 있는데 임상적으로는 전형적 인 GBS에 비해 매우 이질적인 증후군으로 보이지만 면 역학적, 실험실적, 또는 병리학적 소견들은 이들이 GBS의 국소성 아형임을 시사하고 있다.13,14 본 고에서 는 AIDP, AMAN 등을 임의로 전형적 유형(typical type), FS나 기타 국소성 GBS를 변종형 유형(vari- ant type)으로 명명하여 설명하고자 한다. GBS의 현 재 개념은 지난 20여년 동안 현저히 변화되었으며 이전 에는 GBS라고 생각지 않았던 감염 후 말초신경 증후군 들 중에서 몇몇 특이한 증후군들이 일관된 임상적, 면 역학적 특성을 보이는 GBS의 아형들로 확인되고 있다.
이에 본 저자는 GBS의 다양한 임상적 스펙트럼에 초점 을 맞추어 이 분야의 최근 경향 및 연구동향을 간략히 기술하고자 한다.
본 론
1) 전형적 유형(typical type) GBS의 개념변화: 축 삭형 GBS
특히, 지난 20여 년 동안 면역매개성 말초신경병 분 야의 가장 주목할만한 발전이 축삭형 GBS의 병태생리 에서 이루어졌는데, 그 중 대표적인 것이 AMAN의 면 역학적 병태생리에서 항-강글리오시드 항체(anti-gan- glioside antibody)의 역할에 관한 것들이다. 현재 AMAN 의 면역학적 표적이 축삭막의 다양한 강글리오 시드(ganglioside)임이 밝혀져 있다. 즉, 인간 강글리 오시드의 Campylobacter jejuni lipo-oligosaccha- ride(LOS)에 대한 분자모방(molecular mimicry)이 항-강글리오시드 항체에 의한 면역학적 병태생리기전의 유발인자임이 규명된 것이다. 이는 현재까지도 면역학 적 표적이 규명되지 않고 있는 AIDP에 비해 AMAN 의 병태생리가 오히려 더 잘 알려져 있음을 말한다. 흥 미롭게도 전체 GBS의 국가별 발생율은 유사한데 비해15 축삭형/탈수초형 아형의 발생빈도는 그 차이가 심한데,
AIDP가 구미국가에서 흔한 GBS의 아형이라면 AMAN은 아시아, 특히 동아시아에서 흔한 것으로 밝
혀졌다.16,17 이의 주요 원인은 완전히 규명되지는 않았
지만 크게 C. jejuni 감염의 각 지역별 역학적 특성의 차이와18 인종과 연관된 숙주인자들을 고려할 수 있
다.19,20 여기서 주목해야 할 점들은 축삭형 GBS의 개념
이 정립되기 전의 연구나 구미에서 수행된 연구의 결과 는 한국의 GBS에 그대로 적용할 수 없다는 점이다. 이 분야의 자세한 고찰은 본 고의 주제와 거리가 있으므로 최근 문헌들의 소개로 대신한다.21,22
2) 변종형 유형(variant type) GBS의 개념변화: 역 사적 고찰
1938년에 이미 Guillain은 GBS의 다양한 임상양상 을 관찰하고 크게 4가지의 침범패턴으로 첫째는 팔, 다 리만을 침범한 경우, 둘째는 팔, 다리와 뇌신경을 침범 한 경우, 셋째는 뇌신경에 국한된 경우, 넷째는 다발성 신경뿌리병과 의식변화를 보이는 경우를 제시하였다.23 여기서 셋째 증후군은 Fisher syndrome (FS), 넷째 증후군은 Bickerstaff brainstem encephalitis (BBE)의 임상양상을 기술했을 가능성이 있다. 1951년 에 Bickerstaff과 Cloake는“Mesencephalitis and rhombencephalitis”이라는 제목의 논문에서 감염력이 있은 후 안구마비, 실조증, 및 의식장애가 있다가 완전 히 회복된 환자를 처음 기술하고 환자군을 고찰하였
다.24,25 1956년에 Miller Fisher는 “An unusual
variant of acute idiopathic polyneuritis(syn- drome of ophthalmoplegia, ataxia and areflex- ia)”라는 제목의 증례를 보고하였다.26 Bickerstaff과 Fisher의 보고는 안구마비와 실조증이 함께 있다는 측 면에서 매우 유사하였으며 두 저자 모두 감염후의 면역 학적인 기전이 이 질환의 병태생리에 관여할 것으로 추 정하였지만 이 질환이 GBS와는 별개의 질환으로 판단 하였다. 1962년 Richter는 “The ataxic form of polyradiculoneuritis(Landry-Guillain-Barré syn- drome)”라는 제목의 부검 예를 보고하였는데 안구마비 가 거의 없는 상태에서 존재한 실조증을 임상양상으로 기술하였다.27 1986년에 Ropper는 급속하게 진행하는 구인두근육의 위약과 경부 및 어깨 근육의 마비를 보이 면서 하지의 운동기능과 사지의 감각기능이 보전되는 botulism 유사성 증후군을 보고하였다.14 그는 또한 다 른 비전형적인 감염후 마비 증후군을 보고하였는데 심 부건반사가 소실되면서 하반신 불완전마비에 국한된 형 태의 증후군과14,28 급성 진행성 안면양측마비와 facial 사지의 저림으로 발현한 증후군 등이 있다.28 상기 일련 의 증후군들은 알부민세포해리와 신경전도 이상이 존재 함으로 인해 GBS의 국소아형으로 여겨지게 되었고
“pharyngeal-cervical-brachial weakness (PCB)”,
“lumbar polyradiculopathy, lumbar plexopathy, or paraparetic variant” 및 “bifacial weakness with paresthesias or facial diplegia with pares- thesias”등의 이름으로 명명되었다.
3) 변종형 유형(variant type) GBS: 국소성 GBS 아형
앞서 언급한 바와 같이 선행하는 감염력, 심부건 반 사 소실, 원위부 저림, 알부민세포해리의 존재와 신경 전도 이상 등의 소견은 상기 증후군들이 GBS의 국소성 아형일 가능성을 시사하고 있다. 또한 FS 또는 PCB 환자의 일정부분에서는 전통적인 사지의 운동기능을 심 하게 침범하는 전형적 유형의 GBS가 발생하는 경우도 보고되고 있다.29,30 역으로 GBS 환자가 회복기에 PCB 형태의 임상소견을 보였다는 보고도 있다.31 즉, 이러한 GBS와 중첩증후군으로 나타나는 점도 FS와 PCB가 GBS의 국소성 아형임을 뒷받침한다.
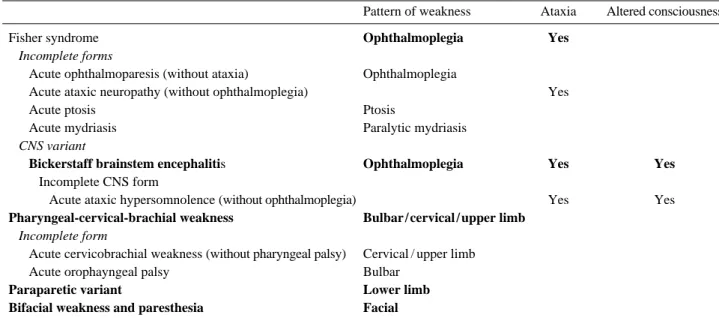
Table 1은 지금까지 보고된 GBS의 국소성 아형을 정리한 것이다. FS는 세부적으로 구분하면 기존의 주 요 증상의 존재 여부에 따라서 불완전형들(incomplete forms, acute ophthalmoparesis; acute ataxic neuropathy; acute ptosis and acute mydriasis) 과 중추신경계 침범형(CNS variant, BBE; and its incomplete form, acute ataxic hypersomno- lence)으로 분류하였다. PCB 아형 역시 불완전형으로 서 acute cervicobrachial weakness와 acute oropharyngeal palsy가 있다. Massachusetts Gen- eral Hospital에서 250여명의 GBS 또는 GBS 아형을
전향적으로 분석한 연구는 FS (5%)이 가장 흔한 국소 성 아형이고 PCB (3%)아형이 그 다음으로 흔한 것으 로 보고하였다.32 Paraparetic GBS아형 bifacial weakness with paresthesias 아형은 매우 드물었다 (<1%). Paraparetic GBS 아형은 매우 드물고 양측 의 좌골신경통 같은 다리 통증이 초기에 현저하고 하지 의 위약이 발생하며 심부건반사는 하지에서만 감소하기 때문에 허리 신경뿌리에 국소화됨을 추정한다.14,28 대칭 성의 근위약과 근력의 회복, 알부민세포해리의 존재는 이 증후군이 GBS의 아형임을 시사하는 면이고 물론 이 의 진단을 위해서는 다른 원인의 허리 신경뿌리병을 철 저히 배제해야 한다. 급성 감각 또는 자율신경병이 GBS와 유사한 패턴으로 감염 후 자가면역성으로 발생 할 수 있음이 보고되었다.33-36 이들 아형이 존재한다면 세섬유신경병이 GBS의 아형 형태로 발현할 수 있음을 증명하는 것이다. 하지만 이 군의 신경병은 발현 양상 에 따라서 알부민세포해리나 기타 GBS를 시사하는 특 징들이 부재하는 경우가 있어서 GBS의 아형으로 보는 것은 무리가 있다. 하지만 순수 감각성 GBS 또는 급성 감각 실조성 GBS로29,34 묘사되는 acute sensory large-fiber neuropathy36는 FS와 동일한 면역학적 소견을 보이므로 FS의 불완전형 또는“acute ataxic neuropathy”로서 GBS의 아형으로 고려할 수 있다.37
임상 스펙트럼-혈청학적 연관성(clinic-serolog- ical relationship)
축삭형 GBS의 병태생리 규명에 따라서 특정 강글리 오시드와 말초신경병과의 인과관계는 몇몇의 선구적인 연구들에 의해 입증되었다.38,39 이후 2001년 Yuki 등은 소의 뇌에서 유래한 강글리오시드 복합물 또는 분리된
Table 1. Clinical features of regional variants of Guillain-Barré syndrome
Pattern of weakness Ataxia Altered consciousness
Fisher syndrome Ophthalmoplegia Yes
Incomplete forms
Acute ophthalmoparesis (without ataxia) Ophthalmoplegia
Acute ataxic neuropathy (without ophthalmoplegia) Yes
Acute ptosis Ptosis
Acute mydriasis Paralytic mydriasis
CNS variant
Bickerstaff brainstem encephalitis Ophthalmoplegia Yes Yes
Incomplete CNS form
Acute ataxic hypersomnolence (without ophthalmoplegia) Yes Yes
Pharyngeal-cervical-brachial weakness Bulbar / cervical / upper limb Incomplete form
Acute cervicobrachial weakness (without pharyngeal palsy) Cervical / upper limb
Acute orophayngeal palsy Bulbar
Paraparetic variant Lower limb
Bifacial weakness and paresthesia Facial
Source: courtesy of Dr. Ben Wakerley, John Radcliffe Hospital, Oxford, UK (table from manuscript in preparation)
강글리오시드 GM1을 토끼에 주입하여 AMAN의 동물 모델을 만듦으로써 강글리오시드와 AMAN의 발생관계 를 증명하였다.40 AMAN 동물모델은 IgG 항GM1 항 체를 생성했고 임상적으로 단상성의 이완성 사지위약을 보였다. 병리학적으로 말초신경은 임파구의 침윤이나 탈수초 소견이 없는 현저한 왈러변성을 보였다. 또한 AMAN 환자의 부검 소견과 매우 유사하게 동물모델의 랑비에르 결절에서 IgG 부착과 periaxonal space의 대식세포의 침윤소견이 마미나 복측 신경근 조직에서 관찰되었다.41 또 다른 시도로 C. jejuni LOS의 면역접 종 시에도 AMAN과 유사한 말초신경병증이 발생하는 것이 확인되었다.42 항-GM1, -GM1b, -GD1a, and - GalNAc-GD1a와 같은 항체들은 아시아국가에서 발생 하는 GBS에서 빈번하게 양성으로 나타나며 현재 AMAN의 대표적 표지자로 받아들여지고 있다.43 근래 에는 이 항체들은 전기생리학적 패턴을 결정하는 중요 한 인자로도 확인되었다.11,44-46 또한 GBS의 전형적인 임상양상이 아닌 국소적 뇌신경병증, 실조증이나 부분 적 안구운동장애 등의 비전형적 증상들도 특정 항체의 존재와 연관하여 부분적으로 설명할 수 있음이 보고되
고 있다(Table 2).13,47-51
국내 연구결과
국내에서 GBS의 임상 스펙트럼에 관한 다기관 연구 는 유일한데 이에 의하면 국내 GBS 환자의 50%에 한 가지 이상의 항-강글리오시드 항체가 양성으로 검출되 어서 기존의 보고들과 같이 축삭형 GBS가 다른 동아시 아국가처럼 국내에도 많을 것임을 시사하였다.52 특히 IgG GQ1b 또는 IgG GT1a 항체가 상대적으로 많이 검출되었으며 각 항체별로 기존에 보고된 임상스펙트럼 과 유사한 결과를 국내의 GBS환자에서도 확인할 수 있 었다. 이 연구는 반복적 신경전도검사를 시행하지 않았 기 때문에 GBS아형 분류 시에 항-강글리오시드 항체 양성 GBS 환자에서도 반수이상(68%)에서 AIDP로 분 류되었다. 하지만 항-강글리오시드 항체 양성 GBS 환 자들은 위장관계 선행감염, 감각신경 증상의 부재, 적 은 빈도의 뇌신경증상 등과 같은 AMAN의 임상양상에 부합하는 특징들을 보였다.44 따라서 이 연구는 국내 GBS의 면역학적/임상적 특징을 기술한 외에도 단일 신 경전도결과에 의한 GBS의 탈수초형 또는 축삭형으로의
Table 2. Antibodies versus clinical spectrums in Guillain-Barré Syndrome
Clinical Presentation Target Antigen Localization in Humans Localization in Animals
Acute inflammatory Unknown
demyelinating polyneuropathy (AIDP)
Acute motor axonal GM1, GD1a, Myelinated axons in Axolemma at
neuropathy (AMAN) GalNac-GD1a, GM1b both motor and node/paranode/myelin
sensory nerves, node of motor nerve, dorsal of Ranvier, abaxonal root ganglia, motor Schwann cell surfaces* nerve terminals
GD1a Motor myelinated fibers Motor nerve terminal
in ventral root cross section*
GalNAc-GD1a Close to nodes of Axon, motor nerve
Ranvier: nodal and terminal paranodal axolemma
GM1b (distal weakness) Undetermined Undetermined
Acute motor and GM1, GM1b, GD1a Undetermined Undetermined
sensory axonal neuropathy (AMSAN)
Fisher syndrome GQ1b Paranodal myelin of Large neurons in DRG
ocular motor nerves, and motor nerve part of DRG neurons terminals
Sensory ataxic GBS GD1b Large Neurons in DRG, Large neurons in DRG,
paranodal myelin paranodal myelin
Bulbar palsy, GT1a Undetermined Undetermined
pharyngealcervical- brachial variant GBS
Acute Pandysautonomia Unknown
Source: Modified from Kaida K, Ariga T, Yu RK.59*Proposed
분류는 빈번한 오류를 보일 수 있다는 점을 제시하였
다.53,54 이러한 점들은 국외에서도 자주 지적되어 왔으
며 따라서 GBS의 새로운 전기생리학적 진단기준의 필 요성으로 공감대를 이루고 있다.
감별진단
GBS의 국소성 아형들은 임상소견만으로 진단하기가 모호한 경우가 있으며 특히 FS의 경우에는 뇌간 경색 과 같은 중추신경계질환과의 감별이 중요하다. 같은 맥 락으로 임상소견이 비전형적일수록 또는 불완전할 수로 감별진단의 어려움은 커지는데 안구증상, 구증상과 연 관된 PCB 등의 아형들은 중증근무력증, botulism, 또
는 뇌간경색과의 감별이 중요하다(Table 3).55
결 론
이상에서 살펴본 바와 같이 현재의 개념에서 GBS의 임상적 스펙트럼은 매우 다양하며 말초신경계뿐만 아니 라 중추신경계의 다른 질환과도 유사하게 나타날 수 있 다. 하지만 현재까지 이러한 점들을 충분히 반영한 적 정한 GBS의 임상적/전기진단의학적 새 진단 기준은 나 오고 있지 않다. 따라서 임상가들은 이러한 점을 인지 하고 GBS의 진단에 오류가 없도록 하여야 한다. 20여 년 전에 American Academy of Neurology에서는 만성염증성탈수초다발신경병(chronic inflammatory demyelinating polyneuropathy, CIDP)의 엄격한 진단기준을 제정한 바 있으며 당시 이 기준의 민감도는 46% 특이도는 100% 였다.56 다른 질환과 마찬가지로 CIDP 역시 초기 민감한 진단과 치료의 도입이 중요하 므로 진단기준은 좀 더 민감도를 높이면서 비전형적인 CIDP 환자도 포함 가능하도록 개정되었다(96% and 81% respectively).57 이런 관점에 보았을 때, GBS 역시 이 전에 전통적인 관점에서 만들어진 진단 기준보 다는 다양한 임상 스펙트럼에 대한 민감한 진단이 가능 한 새로운 진단기준의 수립이 절실하다. 현재의 진단 기준에58 의해서는 비전형적인 아형들을 초기에 적정하 게 진단하기가 어려우며 오진으로 인한 치료의 지연 또 는 불필요한 치료의 도입이 발생 할 수 있다. 향후 연 구들은 다양한 GBS 아형들의 진단 민감도를 높이는 방 향으로 진행될 가능성이 많고 이를 통해서 임상가들은 각 아형들의 치료반응도나 예후를 예측할 수 있을 것이 다. 특히 항-강글리오시드 항체 양성 GBS 환자에서의 임상-혈청학적 연관성 분석은 임상적뿐만 아니라 대표 적인 면역매개성 말초신경병인 GBS의 면역학적 병태생 리를 규명하는 기초의학적인 면에서도 큰 도움이 될 것 으로 기대할 수 있다.
REFERENCES
1. Yuki N, Hartung HP. Guillain-Barré syndrome. N Engl J Med 2012:366:2294-2304
2. Hughes RAC, Cornblath DR. Guillain-Barré syndrome.
Lancet 2005:366:1653-1666
3. Kuwabara S. Guillain-Barré syndrome. Curr Neurol Neu- rosci Rep 2007:7:57-62
4. Vucic S, Kiernan MC, Cornblath DR. Guillain-Barré syn- drome: an update. J Clin Neurosci 2009:16:733-741 5. Yuki N, Kokubun N, Kuwabara S, et al. Guillain-Barré
syndrome associated with normal or exaggerated tendon reflexes. Journal of neurology 2012:259:1181-1190 Table 3. Differential diagnosis for Guillain-Barré syndrome
and its variants
Guillain-Barré syndrome Acute spinal cord disease Tick paralysis
West Nile poliomyelitis Neoplastic meningitis Myasthenia gravis
Toxins (e.g. neurotoxic shellfish poisoning) Thiamine deficiency
Critical illness neuropathy Acute hypophosphatemia
Polymyopathy following use of high dose corticosteroids Prolonged use of neuromuscular blocking drugs Fisher syndrome
Myasthenia gravis Botulism
Diphtheria Tick paralysis
Basilar artery occlusion
Bickerstaff brainstem encephalitis Wernicke’s encephalopathy Brainstem encephalitis Basilar artery occlusion
Pharyngeal-cervical-brachial weakness Myasthenia gravis
Botulism
Basilar artery occlusion Paraparetic variant
Diabetes Neoplastic Cytomegalovirus Sarcoidosis Lyme disease
Lesions of the cauda equina Bifacial weakness with paresthesias
Lyme disease Sarcoidosis
Source: courtesy of Dr. Ben Wakerley, John Radcliffe Hospi- tal, Oxford, UK (table from manuscript in preparation)
6. Asbury AK, Cornblath DR. Assessment of current diag- nostic criteria for Guillain-Barré syndrome. Annals of neu- rology 1990:27 Suppl:S21-24
7. Sejvar JJ, Kohl KS, Gidudu J, et al. Guillain-Barré syn- drome and Fisher syndrome: case definitions and guide- lines for collection, analysis, and presentation of immu- nization safety data. Vaccine 2011:29:599-612
8. van der Meché FGA, van Doorn PA, Meulstee J, Jen- nekens FG. Diagnostic and classification criteria for the Guillain-Barré syndrome. European neurology 2001:45:
133-139
9. Feasby TE, Gilbert JJ, Brown WF, et al. An acute axonal form of Guillain-Barré polyneuropathy. Brain 1986:109:
1115-1126
10. Ho TW, Mishu B, Li CY, et al. Guillain-Barré syndrome in northern China. relationship to Campylobacter jejuni infection and anti-glycolipid antibodies. Brain 1995:118:
597-605
11. Kuwabara S, Yuki N, Koga M, et al. IgG anti-GM1 anti- body is associated with reversible conduction failure and axonal degeneration in Guillain-Barré syndrome. Ann Neurol 1998:44:202-208
12. Yuki N. Guillain-Barré syndrome and anti-ganglioside antibodies: a clinician-scientist's journey. Proc Jpn Acad Ser B Phys Biol Sci 2012:88:299-326
13. Lee SH, Lim GH, Kim JS, et al. Acute ophthalmoplegia (without ataxia) associated with anti-GQ1b antibody. Neu- rology 2008:71:426-429
14. Ropper AH. Unusual clinical variants and signs in Guil- lain-Barre syndrome. Archives of neurology 1986:43:
1150-1152
15. McGrogan A, Madle GC, Seaman HE, de Vries CS. The epidemiology of Guillain-Barré syndrome worldwide: a systematic literature review. Neuroepidemiology 2009:32:
150-163
16. Rees JH, Gregson NA, Hughes RA. Anti-ganglioside GM1 antibodies in Guillain-Barré syndrome and their relationship to Campylobacter jejuni infection. Ann Neu- rol 1995:38:809-816
17. Omejec G, Podnar S. Retrospective analysis of Slovenian patients with Guillain-Barré syndrome. J Peripher Nerv Syst 2012:17:217-219
18. Blaser MJ, Taylor DN, Feldman RA. Epidemiology of Campylobacter jejuni infections. Epidemiol Rev 1983:5:
157-176
19. Geleijns K, Brouwer BA, Jacobs BC, Houwing-Duister- maat JJ, van Duijn CM, van Doorn PA. The occurrence of Guillain-Barré syndrome within families. Neurology 2004:
63:1747-1750
20. Saunders M, Rake M. Familial Guillain-Barré syndrome.
Lancet 1965:2:1106-1107
21. Bae JS, Yuki N, Kuwabara S, et al. Guillain-Barre syn- drome in Asia. Journal of neurology, neurosurgery, and psychiatry 2013
22. Kuwabara S, Yuki N. Axonal Guillain-Barre syndrome:
concepts and controversies. Lancet neurology 2013:12:
1180-1188
23. Guillain G. Les polyradiculonévrites avec dissociation alumbinocytologique et á evolution favorable. (Syndrome de Guillain et Barré.). J belge Neurol Psychiat 1938:323-329 24. Bickerstaff ER, Cloake PC. Mesencephalitis and rhomben-
cephalitis. Br Med J 1951;ii:4723:77-81
25. Bickerstaff ER. Brain-stem encephalitis: further observa- tions on a grave syndrome with benign prognosis. Br Med J 1957:1384-1387
26. Fisher M. An unusual variant of acute idiopathic polyneu- ritis (syndrome of ophthalmoplegia, ataxia and areflexia).
N Engl J Med 1956:255:57-65
27. Richter RB. The ataxic form of polyradiculoneuritis (Landry-Guillain-Barré syndrome): clinical and pathologic observations. J Neuropathol Exp Neurol 1962:21:171-184 28. Ropper AH. Further regional variants of acute immune
polyneuropathy: bifacial weakness or sixth nerve paresis with paresthesias, lumbar polyradiculopathy, and ataxia with pharyngeal-cervical-brachial weakness. Archives of neurology 1994:51:671-675
29. Jibiki T, Shimizu N, Terashima I, Yuki N. [Guillain-Barre syndrome associated with anti-GQ1b antibody--nosologi- cal relationship between Fisher's syndrome and Guillain- Barre syndrome]. Rinsho shinkeigaku = Clinical neurolo- gy 1994:34:381-384
30. Okuda B, Koga M, Katsuta T, Okamoto K, Yuki N. Ful- minant Guillain-Barre syndrome after Campylobacter jeju- ni enteritis and monospecific anti-GT1a IgG antibody.
Intern Med 2002:41:889-891
31. Miura Y, Susuki K, Yuki N, Ayabe M, Shoji H. Guillain- Barré syndrome presenting pharyngeal-cervical-brachial weakness in the recovery phase. European neurology 2002:48:53-54
32. Ropper AH. The Guillain-Barré syndrome. N Engl J Med 1992:326:1130-1136
33. Koike H, Atsuta N, Adachi H, et al. Clinicopathological features of acute autonomic and sensory neuropathy.
Brain: a journal of neurology 2010:133:2881-2896.
34. Koike H, Hashimoto R, Tomita M, et al. The spectrum of clinicopathological features in pure autonomic neuropathy.
Journal of neurology 2012:259:2067-2075
35. Ohyama K, Yasui K, Hasegawa Y, Morozumi S, Koike H, Sobue G. Differential recovery in cardiac and vasomotor sympathetic functional markers in a patient with acute autonomic sensory and motor neuropathy. Intern Med 2013:52:497-502
36. Uncini A, Yuki N. Sensory Guillain-Barré syndrome and related disorders: an attempt at systematization. Muscle &
nerve 2012:45:464-470
37. Ito M, Matsuno K, Sakumoto Y, Hirata K, Yuki N. Ataxic Guillain-Barré syndrome and acute sensory ataxic neu- ropathy form a continuous spectrum. Journal of neurology, neurosurgery, and psychiatry 2011:82:294-299
38. Kusunoki S, Shimizu J, Chiba A, Ugawa Y, Hitoshi S, Kanazawa I. Experimental sensory neuropathy induced by sensitization with ganglioside GD1b. Annals of neurology 1996:39:424-431
39. Nagai Y, Momoi T, Saito M, Mitsuzawa E, Ohtani S.
Ganglioside syndrome, a new autoimmune neurologic dis- order, experimentally induced with brain gangliosides.
Neuroscience letters 1976:2:107-111
40. Yuki N, Yamada M, Koga M, et al. Animal model of axonal Guillain-Barré syndrome induced by sensitization with GM1 ganglioside. Ann Neurol 2001:49:712-720 41. Susuki K, Nishimoto Y, Yamada M, et al. Acute motor
axonal neuropathy rabbit model: immune attack on nerve root axons. Ann Neurol 2003:54:383-388
42. Yuki N, Susuki K, Koga M, et al. Carbohydrate mimicry between human ganglioside GM1 and Campylobacter jejuni lipooligosaccharide causes Guillain-Barré syn- drome. Proc Natl Acad Sci U S A 2004:101:11404-11409 43. Yuki N. Ganglioside mimicry and peripheral nerve dis-
ease. Muscle Nerve 2007:35:691-711
44. Sekiguchi Y, Uncini A, Yuki N, et al. Antiganglioside antibodies are associated with axonal Guillain-Barre syn- drome: a Japanese-Italian collaborative study. Journal of neurology, neurosurgery, and psychiatry 2012:83:23-28 45. Ogawara K, Kuwabara S, Mori M, Hattori T, Koga M,
Yuki N. Axonal Guillain-Barre syndrome: relation to anti- ganglioside antibodies and Campylobacter jejuni infection in Japan. Ann Neurol 2000:48:624-631
46. Kim JK, Kim DS, Kusunoki S, Kim SJ, Yoo BG. Acute pure motor demyelinating neuropathy with hyperreflexia and anti-GalNAc-GD1a antibodies. Clinical neurology and neurosurgery;114:1345-1347
47. Kusunoki S, Chiba A, Kon K, et al. N-acetylgalac- tosaminyl GD1a is a target molecule for serum antibody in Guillain-Barré syndrome. Ann Neurol 1994:35:570-576
48. Miyazaki T, Kusunoki S, Kaida K, Shiina M, Kanazawa I.
Guillain-Barré syndrome associated with IgG monospecif- ic to ganglioside GD1b. Neurology 2001:56:1227-1229 49. Nagashima T, Koga M, Odaka M, Hirata K, Yuki N. Clin-
ical correlates of serum anti-GT1a IgG antibodies. J Neu- rol Sci 2004:219:139-145
50. Kim SY, Kim JK, Suh CK. Polycranial neuropathy and sensory ataxia with IgG anti-GD1a antibody as a variant of Guillain-Barre syndrome. J Clin Neurosci 2013:20:473- 475
51. Bae JS, Kim JK, Kim SH, Kim OK. Bilateral internal oph- thalmoplegia as an initial sole manifestation of Miller Fisher syndrome. J Clin Neurosci 2009:16:963-964 52. Kim JK, Bae JS, Kim D-S, et al. Prevalence of Anti-Gan-
glioside Antibodies and Their Clinical Correlates with Guillain-Barré Syndrome in Korea: A Nationwide Multi- center Study. Journal of clinical neurology 2014:10:94- 100
53. Uncini A, Kuwabara S. Electrodiagnostic criteria for Guil- lain-Barré syndrome: a critical revision and the need for an update. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology 2012:123:1487-1495
54. Uncini A, Manzoli C, Notturno F, Capasso M. Pitfalls in electrodiagnosis of Guillain-Barré syndrome subtypes.
Journal of neurology, neurosurgery, and psychiatry 2010:81:1157-1163
55. Wakerley BR, Yuki N. Pharyngeal-cervical-brachial vari- ant of Guillain-Barré syndrome. Journal of neurology, neurosurgery, and psychiatry 2014:85:339-344
56. Research criteria for diagnosis of chronic inflammatory demyelinating polyneuropathy (CIDP). Report from an Ad Hoc Subcommittee of the American Academy of Neurolo- gy AIDS Task Force. Neurology 1991:41:617-618 57. European Federation of Neurological Societies/Peripheral
Nerve Society Guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy:
report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society-- First Revision. Journal of the peripheral nervous system : JPNS 2010:15:1-9
58. Asbury AK, Arnason BG, Adams RD. The inflammatory lesion in idiopathic polyneuritis. Its role in pathogenesis.
Medicine (Baltimore) 1969:48:173-215
59. Kaida K, Ariga T, Yu RK. Antiganglioside antibodies and their pathophysiological effects on Guillain-Barre syn- drome and related disorders--a review. Glycobiology 2009:19:676-692