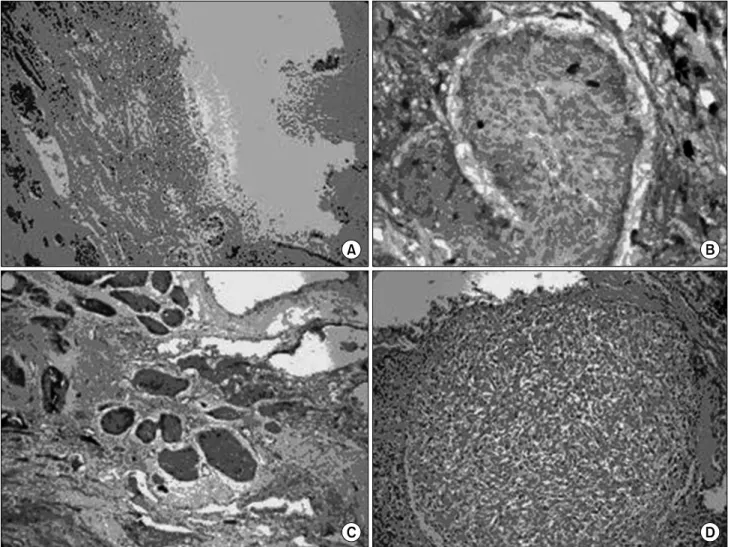
Conjunction of a Fungus Ball and a Pulmonary Tumourlet in a Bronchiectatic Cavity
4
0
0
전체 글
(2)
(3)
(4)
수치
관련 문서
Forces exerted by a flowing fluid on a pipe bend, enlargement, or contraction in a pipeline may be computed by a application of the impulse-momentum principle...
A and E, In control group, a small amount of new bone was observed at the margin of bone defect (40×); B and F, In experimental group 1, a large amount of new bone was formed
[r]
Urban freeway plays a key role in the urban transportation system and also takes a lot of share in the urban traffic generated in the big city. However,
Since every classical or virtual knot is equivalent to the unknot via a sequence of the extended Reidmeister moves together with the forbidden moves, illustrated in Section 2,
This book contains hundreds of complete, working examples illustrating many common Java programming tasks using the core, enterprise, and foun- dation classes APIs.. Java Examples
The index is calculated with the latest 5-year auction data of 400 selected Classic, Modern, and Contemporary Chinese painting artists from major auction houses..
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
