pISSN: 0378-6471 eISSN: 2092-9374
http://dx.doi.org/10.3341/jkos.2013.54.10.1554
= 증례보고 =
잠복 맥락막신생혈관을 동반한 나이관련황반변성에서 베바시주맙 단독치료와 광역학요법 병합치료
오종현1⋅김성우2⋅오재령2⋅권순선3⋅허 걸2
동국대학교 일산병원 안과1, 고려대학교 의과대학 안과학교실2, 고려대학교 의과대학 의학통계학교실3
목적: 잠복 맥락막신생혈관을 동반한 나이관련황반변성 환자에서 베바시주맙 단독치료와 광역학요법 병합치료의 결과를 비교하고자 하였다.
대상과 방법: 베바시주맙 단독치료(IVB군) 또는 광역학요법 병합치료(PDT+IVB군)를 받은 잠복 맥락막신생혈관을 동반한 나이관련황반 변성 환자들 중 경과관찰 기간이 12개월 이상인 경우를 대상으로 후향적으로 분석하였다. 광역학요법은 절반 에너지를 이용하였고, 두군 모두 베바시주맙 유리체강내주사를 3회 연속 시행한 후 필요한 경우에 재주사를 시행하였다. 최대교정시력, 중심황반두께, 재주 사 횟수 등을 비교하였다.
결과: IVB군은 39안이었으며 PDT+IVB군은 25안이었다. 12개월에 PDT+IVB군에서는 평균최대교정시력이 치료전보다 향상되었지만 (p=0.046) IVB 군에서는 그렇지 않았다(p=0.213). 두군 모두 평균중심황반두께가 유의하게 감소하였다(p<0.001). 평균 재주사 횟수는 IVB군은 1.6회, PDT+IVB군은 0.5회였고(p=0.001). 두군 모두 심각한 합병증은 없었다.
결론: 잠복 맥락막신생혈관을 동반한 나이관련황반변성 환자에서 광역학요법 병합치료는 시력을 향상시켰고 재주사 횟수를 감소시켰다.
<대한안과학회지 2013;54(10):1554-1560>
■Received: 2013. 1. 4. ■ Revised: 2013. 5. 14.
■Accepted: 2013. 8. 24.
■Address reprint requests to Seong-Woo Kim, MD, PhD Department of Ophthalmology, Korea University Ansan Hospital, #123 Jeokgeum-ro, Danwon-gu, Ansan 425-707, Korea Tel: 82-31-412-5160, Fax: 82-31-412-4864
E-mail: [email protected]
* This study was presented as a poster at the 10th International AMD and Retina Congress, 29-30 October 2010, Lugano, Switzerland.
* A grant from the Korean Health Technology R&D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea (A102024) supported this study.
Verteporfin을 이용한 광역학요법(photodynamic therapy) 은 몇 년 전까지 나이관련황반변성(age-related macular degeneration)에 동반된 맥락막신생혈관(choroidal neo- vascularization)의 표준치료방법이었다.1 그렇지만 현재는 항-혈관내피성장인자(vascular endothelial growth factor, VEGF)의 유리체강내주사가 표준치료방법으로서 널리 이 용되고 있다.2,3 초기 연구에서는 2년 넘게 매달 주사하는 방법을 사용하였지만2,4이는 많은 비용이 소요되고 안내염 등의 합병 가능성이 증가한다. 따라서 주사 횟수를 줄이기 위해 재주사 간격을 늘리는 방법, 필요한 경우에만 재주사 하는 방법 등이 연구되어 보고되었다.5-9또한 최근에는 광 역학요법을 항-VEGF 유리체강내주사와 병합하는 방법에
대해서도 많이 연구되고 있다.10-15그렇지만 그 결과가 다 양하게 보고되었으며 맥락막신생혈관의 형태를 구분하여 보고한 연구는 없었다.
습성 나이관련황반변성에 동반된 잠복(occult) 맥락막신 생혈관은 전형적(classic) 형태보다 더 흔하지만16이에 대 한 최적의 치료방법은 아직 확립되지 않았다. 잠복 맥락막 신생혈관의 치료에 광역학요법은 그 효과가 제한적이고17,18 항-VEGF 유리체강내주사가 보다 효과적인 것으로 알려졌
다.2,4,19,20 그렇지만 광역학요법은 여전히 효과적일 것으로
기대되고 있으며 특히 아시아인에서 그러하다.18,21게다가 절 반에너지를 이용한 광역학요법은 표준에너지를 이용한 것과 비슷한 효과를 보이며 더 안전하다고 보고되고 있다.22,23
본 연구에서는 잠복 맥락막신생혈관을 동반한 나이관련 황반변성 환자에서 절반에너지를 이용한 광역학요법과 베 바시주맙(bevacizumab) 유리체강내주사의 병합치료와 베 바시주맙 단독치료의 결과를 비교하여 광역학요법 병합치 료가 최대교정시력과 중심황반두께의 변화에 이득을 주는 지, 재주사 횟수를 감소시킬 수 있는지 알아보고자 하였다.
대상과 방법
본 연구는 2007년 6월에서 2009년 8월까지 본원 안과에 서 잠복 맥락막신생혈관을 동반한 나이관련황반변성으로
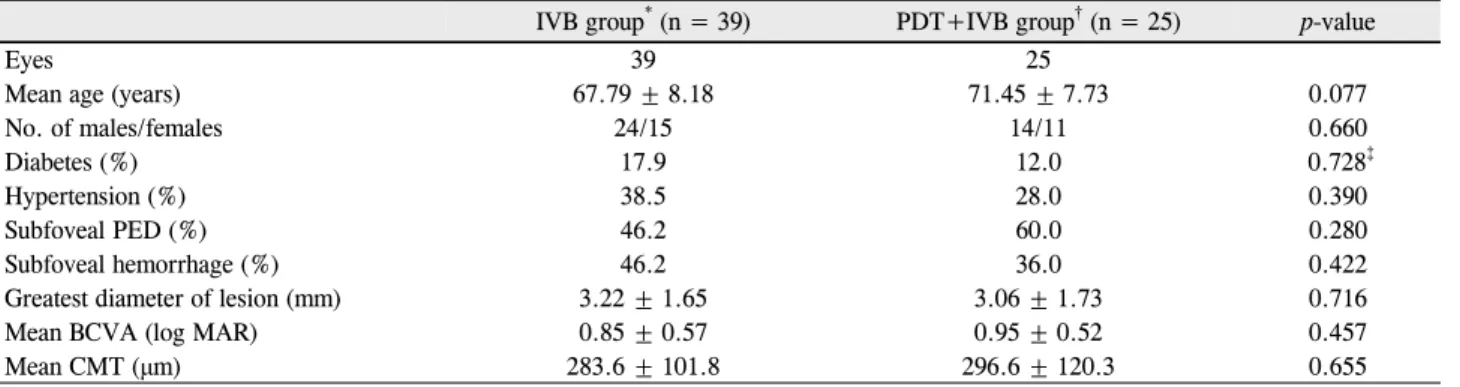
Table 1. Baseline characteristics of the patients
IVB group* (n = 39) PDT+IVB group† (n = 25) p-value
Eyes 39 25
Mean age (years) 67.79 ± 8.18 71.45 ± 7.73 0.077
No. of males/females 24/15 14/11 0.660
Diabetes (%) 17.9 12.0 0.728‡
Hypertension (%) 38.5 28.0 0.390
Subfoveal PED (%) 46.2 60.0 0.280
Subfoveal hemorrhage (%) 46.2 36.0 0.422
Greatest diameter of lesion (mm) 3.22 ± 1.65 3.06 ± 1.73 0.716
Mean BCVA (log MAR) 0.85 ± 0.57 0.95 ± 0.52 0.457
Mean CMT (μm) 283.6 ± 101.8 296.6 ± 120.3 0.655
Values are presented as mean ± SD.
PED = pigment epithelial detachment; BCVA = best-corrected visual acuity; CMT = central macular thickness.
*Patients who underwent intravitreal bevacizumab monotherapy; †Patients who underwent combined therapy with half-fluence rate verteporfin photodynamic therapy; ‡Fisher's exact test.
진단받고 베바시주맙 유리체강내주사 단독치료(IVB군) 또 는 광역학요법 병합치료(PDT+IVB군)를 받은 환자들 중 12개월 이상 경과관찰이 가능하였던 환자를 대상으로 후 향적으로 분석하였다. 형광안저촬영검사(fluorescein an- giography)로 잠복(occult) 맥락막신생혈관(choroidal ne- ovascularization)을 진단하였으며 나이가 50세 미만이거나 전형적(classic) 맥락막신생혈관이 존재하거나 이전에 다 른 치료를 받은 경우, 다른 망막질환을 동반하는 경우는 제 외하였다.
광역학요법은 절반 에너지를 이용하였다. 체표면적당(m2) 6 mg의 verteporfin (Visudyne; Novartis Ophthalmics, Basel, Switzerland)을 3 ml/min의 속도로 10분에 걸쳐서 정맥주사를 하고, 5분이 경과한 후에 689 nm 파장의 비온 열 다이오드레이저인 Opal Photoactivator (Coherent, Santa Clara, CA, USA)를 이용하여 83초 동안 300 mW/cm2의 세 기로 조사하여 25 J/cm2의에너지를 전달하였다. 형광안저 촬영사진을 이용하여 형광 누출과 이상혈관을 포함한 병변 부위의 최대병변직경을 측정하였고 레이저조사범위는 이보 다 1,000 μm 크게 하였다.
PDT+IVB군에서는 광역학요법을 시행한 후 2-3일째부 터 4-6주 간격으로 베바시주맙 유리체강내주사를 3회 연 속 시행하였다. 한편 IVB군에서는 베바시주맙 유리체강내 주사만 4-6주 간격으로 3회 연속 시행하였다. 베바시주맙 유리체강내주사는 무균적 방법으로 1.25 mg/0.05 ml의 베 바시주맙을 30게이지 주사바늘로 각막윤부로부터 3.0-3.5 mm 떨어진 섬모체평면부를 통해 유리체강내로 주입하였 다. 3번째 베바시주맙 유리체강내주사 후 첫 두 달 동안은 매달 경과관찰하였다. 이후에도 병변이 안정적이면 4개월 동안 2달 간격으로 경과관찰하였고, 이후 3개월마다 경과 관찰하였다. 재치료를 받은 경우에는 경과관찰 간격을 다시
1개월로 줄인 뒤 앞서 기술한대로 늘렸다.
경과관찰 중 빛간섭단층촬영검사(optical coherence to- mography, OCT; Stratus OCT, Carl Zeiss Meditec, Dublin, CA, USA)에서 새로운 망막내액 또는 망막하액, 망 막색소상피박리가 관찰되거나 중심황반두께가 100 μm이 상 증가한 경우, 중심황반두께 증가와 함께 시력저하가 있 는 경우, 망막색소상피박리의 높이 또는 직경의 증가가 관 찰되는 경우, 안저검사에서 새로운 망막출혈이 발생한 경 우, 형광안저촬영검사에서 활동성 맥락막신생혈관 소견이 관찰되는 경우 등에서 재치료로서 베바시주맙 유리체강내 주사를 시행하였다.9장액 망막색소상피박리의 존재 자체는 재치료 고려대상이 아니었으며 광역학요법은 추가하여 시 행하지 않았다.
치료의 방법은 진료 의사에 따라 달랐다. 그렇지만 경과 관찰 기간과 재치료의 판단은 동일한 기준에서 이루어졌다.
치료 전, 치료시작 후 3, 6, 12개월의 최대교정시력(snellen), 중심황반두께를 조사하였다. 중심황반두께는 OCT에서 중 심부 1 mm영역의 두께로 정의하였다. 또한 환자의 나이, 성 별, 당뇨 또는 고혈압 유무, 치료전 병변의 크기, 재치료율, 재주사 횟수 등을 조사하였다. 부작용 발생에 대해서도 조사 하였다. 통계분석은 SPSS software version 12.0 (SPSS Inc., Chicago, IL, USA)으로 t-test와 chi-square test 또 는 Fisher's exact test를 사용하였고 p-value가 0.05보다 작은 경우를 유의한 것으로 간주하였다.
결 과
연구기간 동안 총 107안이 잠복 맥락막신생혈관을 동반 한 나이관련황반변성으로 진단받았고, 이중 65안은 베바시 주맙 유리체강내주사 단독치료, 42안은 광역학요법 병합치
Table 2. Changes in best-corrected visual acuity during the 12-month follow-up period
n (eyes) IVB group* n (eyes) PDT+IVB group† p-value
Baseline (log MAR) 39 0.85 ± 0.57 25 0.95 ± 0.52 0.457
3 months (log MAR) 38 0.75 ± 0.51 22 0.71 ± 0.54 0.794
6 months (log MAR) 34 0.67 ± 0.47 21 0.73 ± 0.57 0.665
9 months (log MAR) 36 0.75 ± 0.49 17 0.77 ± 0.48 0.870
12 months (log MAR) 39 0.77 ± 0.56 25 0.79 ± 0.60 0.918
*Patients who underwent intravitreal bevacizumab monotherapy; †Patients who underwent combined therapy with half-fluence rate verteporfin photodynamic therapy.
Table 3. Results after 12 months of follow-up
IVB group* (39 eyes) PDT+IVB group† (25 eyes) p-value Mean difference in BCVA (log MAR) from baseline -0.07 ± 0.36 (p = 0.213) -0.16 ± 0.38 (p = 0.046)
Mean difference in CMT (μm) from baseline -73.1 ± 102.9 (p<0.001) -115.4 ± 115.7 (p<0.001) 0.195
Retreatment (%) 74.4 28.0 <0.001
Mean number of additional IVB injections 1.59 ± 1.33 0.52 ± 1.01 0.001
Values are presented as mean ± SD.
BCVA = best-corrected visual acuity; CMT = central macular thickness; IVB = intravitreal bevacizumab.
*Patients who underwent intravitreal bevacizumab monotherapy; †Patients who underwent combined therapy with half-fluence rate verteporfin photodynamic therapy.
Table 4. Changes in central macular thickness during the 12-month follow-up period
n (eyes) IVB group* n (eyes) PDT+IVB group† p-value
Baseline (μm) 39 283.6 ± 101.8 25 296.6 ± 120.3 0.655
3 months (μm) 38 198.5 ± 66.3 22 204.1 ± 70.0 0.764
6 months (μm) 34 224.4 ± 75.2 21 220.2 ± 110.1 0.888
9 months (μm) 36 208.1 ± 85.9 17 227.0 ± 82.7 0.499
12 months (μm) 39 206.9 ± 89.3 25 181.1 ± 56.8 0.209
Values are presented as mean ± SD.
*Patients who underwent intravitreal bevacizumab monotherapy; †Patients who underwent combined therapy with half-fluence rate verteporfin photodynamic therapy.
Months
Figure 1. Changes in best-corrected visual acuity (BCVA)
during the 12-month follow-up period. Patients underwent in- travitreal bevacizumab monotherapy (IVB group) or combined therapy with half-fluence rate verteporfin photodynamic ther- apy (PDT+IVB group) for occult choroidal neovascularization in age-related macular degeneration. Error bars represent +1 standard error of the mean.료를 받았다. 이중에서 43안은 경과관찰 또는 치료가 예정 대로 이루어지지 않았거나 경과관찰 기간이 12개월 미만이 었다. 예정대로 12개월 이상 경과관찰하면서 예정대로 치 료를 받았던 64안과 그렇지 않은 43안 사이에 치료전 나이, 성비, 당뇨또는고혈압 유병율, 중심와밑 색소상피박리 또 는 출혈의 비율, 최대병변직경, 최대교정시력, 황반중심두 께 등의 차이는 관찰되지 않았다.
대상환자 총 64명 64안 중에 IVB군이 39안, PDT+IVB 군이 25안이었다. 각 군의 치료전 특징들은 Table 1에 요 약하였다. 두군 사이에 치료 전 나이, 성비, 당뇨 또는 고혈 압 유병률, 중심와밑 색소상피박리 또는 출혈의 비율, 최대 병변직경, 최대교정시력, 황반중심두께 등의 차이는 관찰되 지 않았다.
평균최대교정시력은 모든 시기에서 두 군간 유의한 차이 를 보이지 않았다(Table 2, Fig. 1). 치료전과 비교했을 때 치료시작 12개월 후 PDT+IVB군에서는 평균최대교정시력 이 유의하게 향상되었지만(p=0.046) IVB군에서는 그렇지 않았다(p=0.213, Table 3). 치료시작 12개월 후 시력의 안
log MAR BCVA
Table 5. Visual changes from baseline during the 12-month follow-up period
IVB group* (39 eyes) PDT+IVB group† (25 eyes)
Visual Changes 3 months
(n = 38) (%)
6 months (n = 34)
(%)
9 months (n = 36)
(%)
12 months (n = 39)
(%)
3 months (n = 22)
(%)
6 months (n = 21)
(%)
9 months (n = 17)
(%)
12 months (n = 25)
(%) Gain of ≥ 0.3 log MAR 11 (28.9) 10 (29.4) 8 (22.2) 9 (23.1) 8 (36.4) 8 (38.1) 8 (47.1) 9 (23.1) No change or gain of < 0.3 log MAR 19 (50.0) 15 (44.1) 19 (52.8) 17 (43.6) 10 (45.5) 9 (42.9) 4 (23.5) 17 (43.6) Loss of < 0.3 log MAR 5 (13.2) 5 (14.7) 7 (19.4) 10 (25.6) 2 (9.1) 2 (9.5) 2 (11.8) 10 (25.6) Loss of ≥ 0.3 log MAR 3 (7.9) 4 (11.8) 2 (5.6) 3 (7.7) 2 (9.1) 2 (9.5) 3 (17.6) 3 (7.7) IVB = intravitreal bevacizumab; PDT+IVB = photodynamic therapy+intravitreal bevacizumab.
*Patients who underwent intravitreal bevacizumab monotherapy; †Patients who underwent combined therapy with half-fluence rate verteporfin photodynamic therapy.
Months
Figure 2. Changes in central macular thickness during the
12-month follow-up period. Patients underwent intravitreal bevacizumab monotherapy (IVB group) or combined therapy with half-fluence rate verteporfin photodynamic therapy (PDT+IVB group) for occult choroidal neovascularization in age-related macular degeneration. Error bars represent +1 standard error of the mean.정 또는 향상된 비율은 IVB군(66.7%)과 PDT+IVB군 (76.0%)간에 통계적인 차이가 없었다(p=0.425). 그렇지 만 의미있는 시력 향상(logMAR 0.3 이상의 시력상승)은 IVB군(23.1%)보다 PDT+IVB군(48.0%)에서 더 흔하였다 (p=0.038, Table 4).
평균중심황반두께는 모든 시기에서 두 군간 유의한 차이 를 보이지 않았다(Table 5, Fig. 2). 치료전과 비교했을 때 치료시작 12개월 후 두군 모두 평균중심황반두께가 유의하 게 감소하였다(p<0.001, Table 3)
재치료를 받은 비율은 PDT+IVB군(28.0%)이 IVB군 (74.4%)보다 적었다(p<0.001). 경과관찰기간 동안에 IVB 군 39안 중에서 10안(25.6%)은 추가적인 치료가 필요하지 않았으며 10안(25.6%)은 1회, 10안(25.6%)은 2회, 4안 (10.3%)은 3회, 5안(12.8%)은 4회의 베바시주맙 유리체 강내주사를 더 시행받았다. PDT+IVB군 25안 중에서 18안 (72.0%)은 추가적인 치료가 필요하지 않았으며 3안(12.0%)
은 1회, 3안(12.0%)은 2회, 1안(4.0%)은 4회의 베바시주맙 유리체강내주사를 더 시행 받았다. IVB군은 평균 1.6회, PDT+IVB 군은 평균 0.5회의 베바시주맙 유리체강내주사 를 더 시행받았다(p=0.001, Table 3).
두군 모두 안압상승, 수정체손상, 유리체출혈, 망막박리, 안내염, 망막색소상피파열, 망막하섬유화, 맥락막허혈, 황 반위축 등의 심각한 합병증은 없었다.
고 찰
본 연구에서 PDT+IVB군은 IVB군에 비해 재치료율이 낮았고 평균 재주사 횟수가 적었다. 치료시작 12개월 후 두 군간에 평균최대교정시력에서의 차이는 없었지만 PDT+IVB 군에서는 평균최대교정시력이 유의하게 향상되었다. IVB군 에서는 치료전과 치료시작 12개월 후 평균최대교정시력의 차이가 없었다. 중심황반두께는 두군 모두 치료 후 감소하 였다.
MARINA 연구와 ANCHOR 연구에서는 라니비주맙(rani- bizumab) 유리체강내주사를 매달 시행하여 나이관련황반 변성 환자에서 효과적인 치료결과를 보여 주었다.2,4 그렇 지만 매달 경과관찰하면서 매달 치료를 받는 것은 노인 환 자에게 시간적, 경제적 부담을 주게 된다. 또한 안내염 등의 합병 가능성이 증가하게 된다. 따라서 다양한 치료방법과 경과관찰 방법이 연구되어 왔다. PrONTO 연구에서는 3번 연속 주사를 시행한 뒤 필요한 경우에만 재주사를 시행하 였고,7,9다른 연구들에서는 경과관찰 간격을 늘리는 방법을 시도하였다.8,24본 연구에서도 IVB군에서는 3번 연속 베바 시주맙 유리체강내주사를 시행하였고 필요한 경우에 재치 료를 시행하였으며 병변이 안정적이면 경과관찰 기간을 점 진적으로 늘렸다. 그럼에도 66.7%에서 시력이 안정되거나 향상되었다.
항-VEGF 약물이 혈관신생(angiogenesis)을 억제하고 혈관누출을 감소시키는 것과 달리, 광역학요법은 혈관내피 세포를 직접 손상시키고 혈전을 야기시켜 선택적으로 신생
혈관을 폐쇄시킨다.25,26두 치료는 작용기전이 달라서 상승 효과가 기대되기 때문에 광역학요법과 항-VEGF 유리체강 내주사의 병합치료가 시도되고 있으며22,27,28또한 광역학요 법을 병합하는 것이 나이관련황반변성의 치료에서 항-VEGF 유리체강내주사의 횟수를 줄일 수 있는지에 대한 연구도 많이 이루어지고 있다.10-15Lew et al10은 광역학요법 병합 치료를 받은 45안과 베바시주맙 단독치료를 받은 27안을 후향적으로 연구하였으며 치료시작 6개월후 병합치료가 최 대교정시력과 재치료율에서 더 좋은 결과를 보였다고 보고 하였다. Rudnisky et al11은 광역학요법 병합치료를 받은 236안과 베바시주맙 단독치료를 받은 139안을 후향적으로 연구하였으며 12개월 이상 경과한 후 최대교정시력과 주사 횟수가 두 군간에 차이가 없었다고 보고하였다. Bashshur et al12은 전향적 연구에서 광역학요법과 1회의 라니비주맙 유리체강내주사를 20안에서, 3회 연속 라니비주맙 유리체 강내주사를 20안에서 시행한 뒤 필요한 경우에 라니비주맙 유리체강내주사를 시행하며 12개월동안 경과관찰하였다.
그들은 병합치료가 재주사 횟수를 줄였지만 라니비주맙 단 독치료군에서 더 좋은 시력향상을 보였다고 보고하였다.12 MONT BLANC 연구와 DENALI 연구는 다기관, 이중맹검, 무작위 연구로서 습성 나이관련황반변성 광역학요법 병합 치료와 라니비주맙 단독치료를 1년동안 비교하였으며 필요 시 광역학요법의 재치료도 시행하였다.13,14MONT BLANC 연구에서 광역학요법 병합치료는 라니비주맙 단독치료보다 효과가 나쁘지 않았으나 라니비주맙 재주사 횟수를 줄이지 는 못하였다.13 DENALI 연구에서는 광역학요법 병합치료 가 라니비주맙 단독치료보다 효과가 나쁘지는 않았고 라니 비주맙 재주사 횟수를 평균 7.6회에서 2.2-2.8회로 줄였으 나 평균 1.9회의 광역학요법이 시행되었다.14Krebs et al15 은 무작위 전향적 연구에서 광역학요법 병합치료는 라니비 주맙 재주사 횟수를 줄였지만 라니비주맙 단독치료가 시력 을 향상시킨 것과 달리 병합치료군에서는 시력이 악화되었 다고 보고하였다. 광역학요법 병합치료에 대한 많은 연구가 보고되었지만 그 결과는 다양하다. 또한 이전 연구들은 맥 락막신생혈관의 형태를 구분한 결과는 보여주지 않았다. 따 라서 우리는 습성 나이관련황반변성 환자 중에서 잠복 형 태의 맥락막신생혈관을 동반한 경우를 대상으로 광역학요 법 병합치료의 효과를 연구하였고 병합치료가 시력을 향상 시켰고 재치료율과 재주사 횟수를 감소시켰음을 보여 주었 다. 작용기전이 다른 두 치료의 병합이 상승효과를 나타내 어 재치료율을 낮추었고, 재치료율의 감소가 시력의 향상에 기여하였을 것으로 생각된다. 그러나 이는 다수의 환자를 대상으로 하는 전향적인 연구를 통해 재확인하는 것이 필 요할 것이다.
광역학요법은 정상 맥락막과 망막색소상피층에도 영향 을 끼칠 수 있는 것으로 알려졌는데29베바시주맙 유리체강 내주사와 병합했을 때 정상 맥락막에 대한 광화학적 스트 레스가 증가될 수 있다는 보고도 있다.30따라서 우리는 광 역학요법에서 절반에너지를 이용하였다.22,23,26,31
본 연구의 PDT+IVB군에서 망막색소상피파열 또는 황반위축 같은 광 역학요법과 관련된 합병증은 관찰되지 않았다.
본 연구는 후향적 연구이고 적은 환자를 대상으로 하였 다는 제한점을 갖고 있다. 또한 잠복 맥락막신생혈관을 진 단할 때 인도시아닌그린 혈관조영술(indocyanine green angiography, ICG)을 시행하지 않았다는 제한점도 있다. 이 로 인해 대상 환자들 중에 결절맥락막혈관병증(polypoidal choroidal vasculopathy) 환자가 일부 포함되어 치료결과에 영향을 미쳤을 수 있다. Moon et al32과 Lee et al33은 결절 맥락막혈관병증이 있는 한국인에서 광역학요법 병합치료는 더 나은 결과를 보였다고 하였다.임상적으로 ICG 없이 형 광안저촬영검사로 잠복 맥락막신생혈관을 진단하는 경우도 흔하기 때문에 본 연구의 결과는 임상의들에게 실질적인 도움이 될 것이다.
결론으로 잠복 맥락막신생혈관을 동반한 나이관련황반 변성 환자에서 절반에너지의 광역학요법 병합치료는 12개 월동안 최대교정시력을 향상시켰고 베바시주맙 단독치료보 다 재치료율과 재주사 횟수를 감소시켰다. 그렇지만 다수의 환자를 대상으로 하는 전향적 연구가 더 필요할 것으로 생 각한다.
REFERENCES
1) Verteporfin Roundtable Participants. Guidelines for using verte- porfin (Visudyne) in photodynamic therapy for choroidal neo- vascularization due to age-related macular degeneration and other causes: update. Retina 2005;25:119-34.
2) Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neo- vascular age-related macular degeneration. N Engl J Med 2006;
355:1419-31.
3) Spaide RF, Laud K, Fine HF, et al. Intravitreal bevacizumab treat- ment of choroidal neovascularization secondary to age-related macular degeneration. Retina 2006;26:383-90.
4) Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus ver- teporfin for neovascular age-related macular degeneration. N Engl J Med 2006;355:1432-44.
5) Regillo CD, Brown DM, Abraham P, et al. Randomized, dou- ble-masked, sham-controlled trial of ranibizumab for neovascular age-related macular degeneration: PIER Study year 1. Am J Ophthalmol 2008;145:239-48.
6) Sonmez K, Sonmez PA, Ozkan SS, Atmaca LS. One-year out- comes of less frequent bevacizumab in age-related macular degeneration. Retina 2011;31:645-53.
7) Fung AE, Lalwani GA, Rosenfeld PJ, et al. An optical coherence
tomography-guided, variable dosing regimen with intravitreal ra- nibizumab (Lucentis) for neovascular age-related macular degeneration. Am J Ophthalmol 2007;143:566-83.
8) Cohen SY, Dubois L, Tadayoni R, et al. Results of one-year's treat- ment with ranibizumab for exudative age-related macular degener- ation in a clinical setting. Am J Ophthalmol 2009;148:409-13.
9) Lalwani GA, Rosenfeld PJ, Fung AE, et al. A variable-dosing regi- men with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. Am J Ophthalmol 2009;148:43-58.e1.
10) Lew YJ, Park HJ, Lee TG, et al. Primary combined photodynamic therapy and intravitreal bevacizumab injection for neovascular age-related macular degeneration. J Korean Ophthalmol Soc 2010;51:35-41.
11) Rudnisky C, Liu C, Ng M, et al. Intravitreal bevacizumab alone versus combined verteporfin photodynamic therapy and intra- vitreal bevacizumab for choroidal neovascularization in age-re- lated macular degeneration: visual acuity after 1 year of follow-up.
Retina 2010;30:548-54.
12) Bashshur ZF, Schakal AR, El-Mollayess GM, et al. Ranibizumab monotherapy versus single-session verteporfin photodynamic therapy combined with as-needed ranibizumab treatment for the management of neovascular age-related macular degeneration.
Retina 2011;31:636-44.
13) Larsen M, Schmidt-Erfurth U, Lanzetta P, et al. Verteporfin plus ra- nibizumab for choroidal neovascularization in age-related macular degeneration: twelve-month MONT BLANC study results.
Ophthalmology 2012;119:992-1000.
14) Kaiser PK, Boyer DS, Cruess AF, et al. Verteporfin plus ranibizu- mab for choroidal neovascularization in age-related macular de- generation: twelve-month results of the DENALI study. Ophthal- mology 2012;119:1001-10.
15) Krebs I, Vécsei Marlovits V, Bodenstorfer J, et al. Comparison of Ranibizumab monotherapy versus combination of Ranibizumab with photodynamic therapy with neovascular age-related macular degeneration. Acta Ophthalmol 2013;91:e178-83.
16) Cohen SY, Creuzot-Garcher C, Darmon J, et al. Types of choroidal neovascularisation in newly diagnosed exudative age-related mac- ular degeneration. Br J Ophthalmol 2007;91:1173-6.
17) Verteporfin In Photodynamic Therapy Study Group. Verteporfin therapy of subfoveal choroidal neovascularization in age-related macular degeneration: two-year results of a randomized clinical trial including lesions with occult with no classic choroidal neo- vascularization--verteporfin in photodynamic therapy report 2.
Am J Ophthalmol 2001;131:541-60.
18) Soubrane G, Harding SP, Wolf S, Weichselberger A. Verteporfin therapy in occult with no classic CNV due to AMD: results of the Photodynamic Therapy in Occult-Only Lesions study. Eye (Lond) 2009;23:791-800.
19) Costagliola C, Romano M, Corte MD, et al. Intravitreal bev- acizumab for treatment-naive patients with subfoveal occult cho- roidal neovascularization secondary to age-related macular degen- eration: a 12-month follow-up study. Retina 2009;29:1227-34.
20) Furino C, Boscia F, Recchimurzo N, et al. Intravitreal bevacizumab for treatment-naïve subfoveal occult choroidal neovascularization in age-related macular degeneration. Acta Ophthalmol 2009;87:
404-7.
21) Japanese Age-Related Macular Degeneration Tial (JAT) Study Group. Japanese age-related macular degeneration trial: 1-year re- sults of photodynamic therapy with verteporfin in Japanese pa- tients with subfoveal choroidal neovascularization secondary to age-related macular degeneration. Am J Ophthalmol 2003;136:
1049-61.
22) Costagliola C, Romano MR, Rinaldi M, et al. Low fluence rate photodynamic therapy combined with intravitreal bevacizumab for neovascular age-related macular degeneration. Br J Ophthalmol 2010;94:180-4.
23) Sacu S, Varga A, Michels S, et al. Reduced fluence versus standard photodynamic therapy in combination with intravitreal triamcinolone:
short-term results of a randomised study. Br J Ophthalmol 2008;
92:1347-51.
24) Spaide R. Ranibizumab according to need: a treatment for age-re- lated macular degeneration. Am J Ophthalmol 2007;143:679-80.
25) Ciulla TA, Rosenfeld PJ. Antivascular endothelial growth factor therapy for neovascular age-related macular degeneration. Curr Opin Ophthalmol 2009;20:158-65.
26) Miller JW, Schmidt-Erfurth U, Sickenberg M, et al. Photodynamic therapy with verteporfin for choroidal neovascularization caused by age-related macular degeneration: results of a single treatment in a phase 1 and 2 study. Arch Ophthalmol 1999;117:1161-73.
27) Kiss CG, Simader C, Michels S, Schmidt-Erfurth U. Combination of verteporfin photodynamic therapy and ranibizumab: effects on retinal anatomy, choroidal perfusion and visual function in the pro- tect study. Br J Ophthalmol 2008;92:1620-7.
28) Antoszyk AN, Tuomi L, Chung CY, Singh A. Ranibizumab com- bined with verteporfin photodynamic therapy in neovascular age-related macular degeneration (FOCUS): year 2 results. Am J Ophthalmol 2008;145:862-74.
29) Parodi MB, Da Pozzo S, Ravalico G. Retinal pigment epithelium changes after photodynamic therapy for choroidal neovascularization in pathological myopia. Acta Ophthalmol Scand 2007;85:50-4.
30) Rouvas AA, Papakostas TD, Ladas ID, Vergados I. Enlargement of the hypofluorescent post photodynamic therapy treatment spot af- ter a combination of photodynamic therapy with an intravitreal in- jection of bevacizumab for retinal angiomatous proliferation.
Graefes Arch Clin Exp Ophthalmol 2008;246:315-8.
31) Michels S, Hansmann F, Geitzenauer W, Schmidt-Erfurth U.
Influence of treatment parameters on selectivity of verteporfin therapy. Invest Ophthalmol Vis Sci 2006;47:371-6.
32) Moon SW, Kim MS, Kim ES, et al. Photodynamic therapy com- bined with intravitreal injection of vascular endothelial growth fac- tor antibody for polypoidal choroidal vasculopathy. Ophthalmologica 2011;225:169-75.
33) Lee JK, Lee JW, Lee JE, et al. Intravitreal Bevacizumab with or without photodynamic therapy for the treatment of polypoidal cho- roidal vasculopathy. J Korean Ophthalmol Soc 2010;51:684-92.
=ABSTRACT=
Bevacizumab Monotherapy Versus Combined Therapy with Photodynamic Therapy for Occult Choroidal Neovascularization in
Age-Related Macular Degeneration
Jong-Hyun Oh, MD, PhD1, Seong-Woo Kim, MD, PhD2, Jaeryung Oh, MD, PhD2, Soon-Sun Kwon, PhD3, Kuhl Huh, MD, PhD2
Department of Ophthalmology, Ilsan Hospital, Dongguk University1, Goyang, Korea Department of Ophthalmology, Korea University College of Medicine2, Seoul, Korea Department of Biostatistics, Korea University College of Medicine3, Seoul, Korea
Purpose: To compare clinical outcomes between intravitreal bevacizumab (IVB) monotherapy and combined therapy with half-fluence rate verteporfin photodynamic therapy (PDT) for occult choroidal neovascularization (CNV) secondary to age-related macular degeneration (AMD).
Methods: Medical records were reviewed in consecutive patients who underwent IVB monotherapy or combined therapy with PDT for occult CNV secondary to AMD and had a 12-month follow-up period. After 3 consecutive monthly IVB in- jections, both groups were eligible for additional IVB injections when necessary. Best-corrected visual acuity (BCVA), cen- tral macular thickness (CMT), and number of additional IVB injections were compared between the groups.
Results: Thirty-nine eyes underwent IVB monotherapy (IVB group) and 25 eyes underwent combined therapy (PDT+IVB group). Mean BCVA improved significantly in the PDT+IVB group (p = 0.046) and not in IVB group (p = 0.213). A significant reduction in mean CMT occurred in both groups (p < 0.001). The mean number of additional IVB injections was 1.6 ± 1.33 in the IVB group and 0.5 ± 1.01 in the PDT+IVB group (p = 0.001). There were no serious complications.
Conclusions: Combined therapy with half-fluence rate PDT improved BCVA and reduced the number of additional IVB in- jections in the eyes with occult CNV secondary to AMD.
J Korean Ophthalmol Soc 2013;54(10):1554-1560
Key Words: Age-related macular degeneration, Bevacizumab, Occult choroidal neovascularization, Photodynamic therapy
Address reprint requests to Seong-Woo Kim, MD, PhD Department of Ophthalmology, Korea University Ansan Hospital
#123 Jeokgeum-ro, Danwon-gu, Ansan 425-707, Korea
Tel: 82-31-412-5160, Fax: 82-31-412-4864, E-mail: [email protected]