서론
1. 연구의 필요성
상기도 근기능 운동은 폐쇄성 수면무호흡증 환자를 대상
으로 폐쇄성 수면무호흡증에 관련된 상기도 근육의 등장성,
등척성 운동을 교육함으로써 상기도 근기능을 강화 및 폐쇄
성 수면무호흡증 증상을 개선시키는 기술이다. 폐쇄성 수면
무호흡증은 전 인구에서 2-4%, 우리나라에서는 3.2-4.5%
의 빈도로 나타나는 매우 흔한 질병으로[1], 수면 동안 반복
적으로 발생하는 상기도 폐색이 특징적이며, 수면부족, 주간
졸림증, 삶의 질 저하, 가족 간의 갈등 증가 등 여러 문제를
발생시킬 수 있어 적절한 치료가 필요하다[2].
폐쇄성 수면무호흡증의 내과적 치료로는 체중감량, 운동
및 금주와 같은 행동요법과 양압기 치료, 약물요법 등이
있다. 이 중 양압기 치료는 폐쇄성 수면무호흡증의 주된 치
료방법이지만 피부발적 및 손상, 폐쇄공포증 등이 발생할
수 있고, 약물요법에 대해서는 아직 효능이 입증되지 않
았다[3].
이에 긍정적인 치료효과와 재발방지를 위한 치료법들이
제안되고 있으며, 상기도 근기능 운동도 그 중 하나이다. 본
연구는 현재 건강보험요양급여비용 목록에 등재되어 있지
않은 신의료기술인 상기도 근기능 운동에 대해 체계적 문헌
고찰을 시행하고 임상 전문가와의 논의를 통해 동 기술의 안
전성과 유효성을 평가하였다.
상기도 근기능 운동: 체계적 문헌고찰
오 수 미·김 진 형·김 석 현 | 한국보건의료연구원 신의료기술평가사업본부Upper airway myofunctional exercise: a systematic
review
Su-mi Oh, RN · Jin-Hyeong Kim, MS · Seok-Hyun Kim, MD*
Division for New Health Technology Assessment, National Evidence-based Healthcare Collaborating Agency, Seoul, Korea
Received: March 29, 2019 Accepted: April 4, 2019 Corresponding author: Seok-Hyun Kim
E-mail: [email protected]
*Current position: Office of Research Planning and Coordination, National Evidence-based Healthcare Collaborating Agency, Seoul, Korea
© Korean Medical Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons. org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Upper airway myofunctional exercise is a training technique for patients with obstructive sleep apnea involving
isotonic and isometric exercises of the upper airway muscles involved in obstructive sleep apnea designed to
strengthen upper airway myofunction and improve patients’ symptoms. The objective of this review was to evaluate
the safety and effectiveness of upper airway myofunctional exercise. A literature search was conducted using 8
Korean databases, Medline, Embase, and the Cochrane Library. Of the 197 articles that were initially identified, 8
studies were included in this review. The results show that upper airway myofunctional exercise improved the
apnea-hypopnea index in adult patients, and that it led to improvements in symptoms and upper airway myofunction when
administered alone or after adenoidectomy in pediatric patients. On the basis of the current data, upper airway
myofunctional exercise can be considered a safe and effective technique for patients with obstructive sleep apnea.
2. 상기도 근기능 운동
무호흡 환자에서 흔히 관찰되는 연구개와 구개수의 비
후, 구개편도와 혀의 비대 등은 인두기도의 구조적인 협착
을 일으켜서 흡기 시 더 높은 흉곽 음압이 요구되며, 이에
덧붙여 상기도 확장근의 긴장도가 떨어지면 상기도 폐쇄
가 더욱 촉진된다[4,5]. 이처럼 상기도 확장근은 기도의 개
방성 유지에 중요한 역할을 하기 때문에 상기도 근기능을
향상시키는 운동을 통해 폐쇄성 수면무호흡증 증상을 완
화할 수 있다[6]. 이러한 이론적 배경을 바탕으로 하는 상
기도 근기능 운동은 상기도의 등척성, 등장성 운동을 통해
혀, 인두와 연구개의 근육 강도를 증진시킬 수 있으며 특
히 경증에서 중등도의 폐쇄성 무호흡증에서 유용하게 활용
될 수 있다[7].
연구방법
1. 연구설계
본 연구는 체계적 문헌고찰을 이용하여 폐쇄성 수면무호
흡증 환자를 대상으로 상기도 근기능 운동의 안전성 및 유효
성을 확인하였다. 본 연구는 PRISMA (Preferred Reporting
Items for Systematic Reviews and Meta-Analysis) 그
룹이 제시한 체계적 문헌고찰 보고지침에 따라 수행되었
다[8].
2. 문헌검색
1) PICO
연구목적에 따른 PICO
(patient-intervention-com-parator-outcome)는 다음과 같다. 대상환자(P)는 폐쇄성
수면무호흡증 환자이고, 중재시술(I)은 상기도 근기능 운동
이며, 비교시술(C)는 비강 호흡 운동(비강 확장기 적용, 코
로 깊게 숨쉬기, 생리식염수 점적), sham 시술, 무시술이다.
마지막으로 연구결과(O)는 안전성 지표인 시술 관련 합병증,
유효성 지표인 증상개선과 상기능 근기능 개선이다. 증상 개
선의 경우 문헌마다 다양한 지표를 제시하고 있어 객관적 지
표 중 무호흡-저호흡 지수, 산소포화도(평균, 최저, 90% 이
하인 시간, 탈포화지수), 주관적 지표 중 주간 졸리움을 주요
지표로 보았다.
2) 문헌검색
국내 문헌검색은 KoreaMed를 포함한 8개 데이터베이
스를 이용하였고, 국외 문헌검색은 Medline,
Ovid-Embase, Cochrane Library 및 국외 의료기술평가기구 홈
페이지 데이터베이스를 이용하여 2017년 3월 31일에 검색
을 수행하였다. 국내 데이터베이스는 색인기능을 고려하여
‘근기능강화’ ‘myofunctional therapy’ 또는 ‘oropharyngeal
exercise’에 초점을 맞추어 광범위하게 검색을 실시하고, 이
후 검색된 범위 내에서 불필요한 문헌을 수작업으로 제외한
결과 확인되는 문헌은 없었다. 국외 데이터베이스는 관련
의학주제표목(Medical Subject Headings) 및 주요 개념어
를 도출하여서 검색을 수행하였다. 이에 따라 ‘{Obstructive
sleep apnea.mp. OR sleep disordered breathing/ OR
Obstructive sleep apnoea.mp. OR (OSA OR OSAS).
mp.} AND [Myofunctional therapy.mp. OR muscle
training/ OR speech therapy.mp. OR speech therapy/
OR Oropharyngeal exercise#.mp. OR tongue-muscle
training.mp. OR {Upper airway adj1 (exercises OR
remodeling)}.mp. OR myofascial reeducation.mp. OR
orofacial myotherapy.mp. OR oral myotherapy.mp.]’의
검색어를 이용한 결과, 총 197편의 문헌이 검색되었다.
이후 엔드노트(EndNote)를 이용하여 46편의 중복 자료
를 제거한 후 남은 151편을 대상으로 논문의 제목과 초록
을 통해 관련 논문을 1차로 선택하고, 선택된 논문의 원문
을 검토하여 다음의 문헌 선정기준에 따라 대상 문헌을 선
정하였다. 폐쇄성 수면무호흡증 환자를 대상으로 상기도 근
기능 운동이 수행되어 적절한 의료결과가 하나 이상 보고
된 연구를 선택하였다. 동물실험 및 전임상시험 연구, 원저
가 아닌 연구, 한국어 또는 영어로 출판되지 않은 연구, 회
색문헌, 증례보고, 중복출판된 연구 및 선택 문헌을 포함하
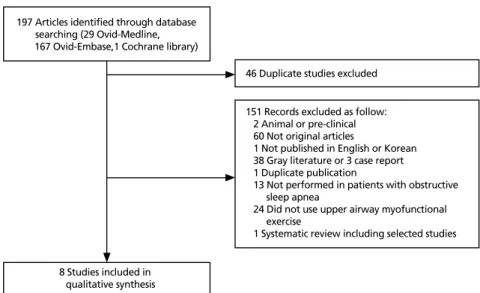
는 체계적 문헌고찰은 배제하였다(Figure 1). 문헌의 선택
및 배제는 두 명의 평가자에 의해 독립적으로 시행되었으
며, 의견이 불일치할 경우 회의를 통해 합의하는 방식을 이
용하였다.
3. 문헌의 질 평가
선택된 문헌의 질 평가는 영국 Scottish Intercollegiate
Guidelines Network (SIGN)의 방법론
체크리스트[9]를 이용하였다. 질 평가
는 두 명의 평가자가 독립적으로 시행한
후, 판정 결과에 차이가 있는 경우 논의
를 통해 이견을 조정하였다. SIGN의 질
평가 도구는 연구유형에 따라 필수항목
을 선정하고, 질 평가 항목에 거의 모든
또는 모든 기준이 충족되는 경우 ‘++’,
몇 가지 기준이 충족된 경우 ‘+’, 거의 모
든 기준이 충족되지 않는 경우 ‘–’로 평
가하였다(Table 1). 이에 따라 맹검 또는
은폐가 되지 않고, 혼란변수에 관한 언
급이 없으며 두 군간 동질성을 확인하
지 않은 문헌은 ‘–’로 평가하였다. 선택
된 연구들의 연구유형과 질 평가 결과를
종합하여 판정하는 근거의 수준 등급은
Table 2와 같다.
4. 자료추출
평가에 포함된 문헌의 자료추출 과정
은 여러 차례 반복되었으며, 임상전문가
의 의견을 반영하여 자료추출 서식의 적
절성을 검토한 후 사용하였다. 자료추출
은 문헌에 기술된 공통된 내용과 결과에
영향을 주는 연구대상의 특성과 함께 필
수적으로 추출되어야 하는 안전성 및 유
효성에 대한 자료를 추출하였다. 자료추
출은 여러 차례 반복하여 수행하여 내용
을 빠짐없이 추출하고자 하였으며, 임상
전문가 회의를 통해 내용을 최종 확인하
였다.
5. 자료분석
자료분석은 정성적 분석을 시행하였
고, 각 지표의 시술 전·후 평균과 표준편차가 보고된 문헌
이 적어 정량적 분석은 수행하지 않았다.
Table 1. SIGN criteria for assignment of quality of studies
Level Description
1++ High quality meta-analyses, systematic reviews of RCTs, or RCT with a very low risk of bias 1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias 1– Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies
High-quality case-control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal
2+ Well-conducted case-control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal
2– Case-control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal
3 Non-analytic studies, e.g., case reports, case series 4 Expert opinion
SIGN, Scottish Intercollegiate Guideline Network; RCT, randomized controlled trial.
Table 2. SIGN criteria for assignment of levels of evidence
Level Description
A At least one meta-analysis, systematic review, or RCT rated as 1++, and directly applicable to the target population; or a body of evidence consisting principally of studies rated as 1+,
directly applicable to the target population, and demonstrating overall consistency of results B A body of evidence including studies rated as 2++, directly applicable to the target population,
and demonstrating overall consistency of results; or extrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly applicable to the target population and demonstrating overall consistency of results; or extrapolated evidence from studies rated
as 2++
D Evidence level 3 or 4; or extrapolated evidence from studies rated as 2+ SIGN, Scottish Intercollegiate Guideline Network; RCT, randomized controlled trial.
8 Studies included in qualitative synthesis 197 Articles identified through database searching (29 Ovid-Medline, 167 Ovid-Embase,1 Cochrane library)
46 Duplicate studies excluded 151 Records excluded as follow: 2 Animal or pre-clinical 60 Not original articles
1 Not published in English or Korean 38 Gray literature or 3 case report 1 Duplicate publication
13 Not performed in patients with obstructive sleep apnea
24 Did not use upper airway myofunctional exercise
1 Systematic review including selected studies
결과
1. 체계적 문헌고찰 대상 문헌의 일반적 특성
검색된 문헌 총 197편 중 중복 검색된 문헌 46편을 제외한
151편을 토대로 선택 및 배제기준을 적용하여 총 8편의 문헌
이 평가에 포함되었다(Figure 1). 연구유형은 무작위 임상시
험 연구(randomized controlled trial, RCT) 5편, 코호트 연
구 1편, 전후 연구 2편이었고 모두 국외에서 발표된 문헌이
었다. 질 평가 시행 결과, 4편[7,10-12]은 1 ‘+’, 1편[13]은
1 ‘–’, 1편[14]은 2 ‘–’로 평가되었다. 평가에 포함된 문헌을
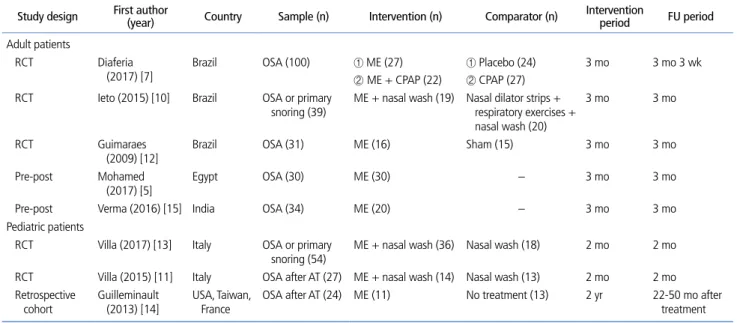
대상별(성인, 소아)로 구분하여 연구 유형, 제1저자의 알파
벳, 연도순으로 제시한 내용은 Table 3과 같다[5,7,10-15].
운동방법은 문헌마다 약간의 차이는 있었으나 주로 연구
개, 혀, 안면, 하악 운동을 기본으로 하고 있었고, 환자들은
전문가에 의해 교육 및 시범 받은 상기도 근기능 운동을 집
에서 지속적으로 시행 후 주기적으로 재평가 받는 방식을 이
용하였다. 구체적인 운동 방법으로는, 성인을 대상으로 한
연구에서는 혀를 브러쉬로 닦기, 경구개 밀기, 입천장에 대
항하여 빨기, 입술을 포개거나 오므리기, 목젖을 상승시키
기, 볼 근육을 누르기, 입 벌렸다 닫기, 풍선불기 등 이었고,
소아를 대상으로 한 연구에서는 혀를 회전시키고 좌우로 움
직이기, 입술을 포개고 진동을 주기, 연구개와 목젖을 상승
시키기, 안면 운동, 턱 움직이기 등이었다.
2. 안전성 및 유효성
상기도 근기능 운동의 안전성에 대해서 보고된 문헌은 확
인되지 않았다. 유효성에 대해서는 8편의 문헌에서 보고하
였으며, 대상별(성인, 소아)로 구분하여 결과를 제시하였다.
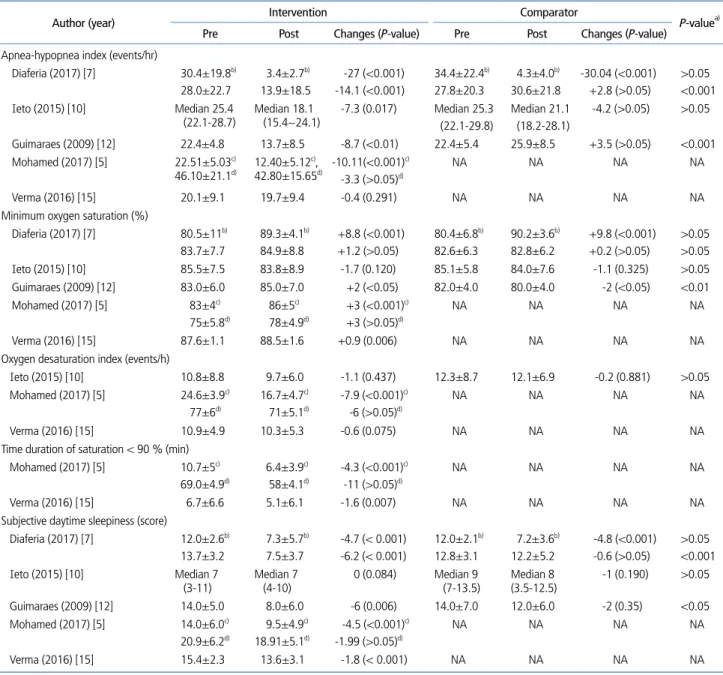
유효성 지표 중 증상개선에 대한 주요 결과를 요약한 내용은
Table 4 [5,7,10,12,15]와 Table 5 [11,14]와 같다.
성인 대상 연구는 총 5편이었다(RCT 3편, 전후 연구
2편). 이 중 1편에서는 지속적 상기도 양압술의 보조 시술로
써 상기도 근기능 운동을 시행하였다. 비교 연구에서 무호
흡-저호흡 지수의 시술 전·후 변화량(3편)은 중재군 -7.3
에서 -14.1, 비교군 -4.2에서 3.5이었다(군간 차이: 2편
P<0.001, 1편 P>0.05). 산소포화도(3편)는 이질적인 결과
를 제시하였다(군간 차이: 1편 P<0.01, 2편 P>0.05). 주간
졸리움의 변화량(3편)은 중재군 -6.2에서 0, 비교군 -2에
서 -0.6이었으며(군간 차이: 2편 P<0.05, 1편 P>0.05), 대
부분의 주관적 지표는 중재군에서만 유의하게 개선되었다.
Table 3. Characteristics of included studies
Study design First author(year) Country Sample (n) Intervention (n) Comparator (n) Intervention period FU period Adult patients RCT Diaferia (2017) [7] Brazil OSA (100) ① ME (27) ② ME + CPAP (22) ① Placebo (24) ② CPAP (27) 3 mo 3 mo 3 wk
RCT Ieto (2015) [10] Brazil OSA or primary
snoring (39) ME + nasal wash (19) Nasal dilator strips + respiratory exercises + nasal wash (20)
3 mo 3 mo
RCT Guimaraes (2009) [12]
Brazil OSA (31) ME (16) Sham (15) 3 mo 3 mo Pre-post Mohamed
(2017) [5] Egypt OSA (30) ME (30) – 3 mo 3 mo Pre-post Verma (2016) [15] India OSA (34) ME (20) – 3 mo 3 mo Pediatric patients
RCT Villa (2017) [13] Italy OSA or primary
snoring (54) ME + nasal wash (36) Nasal wash (18) 2 mo 2 mo RCT Villa (2015) [11] Italy OSA after AT (27) ME + nasal wash (14) Nasal wash (13) 2 mo 2 mo Retrospective
cohort Guilleminault (2013) [14] USA, Taiwan, France OSA after AT (24) ME (11) No treatment (13) 2 yr 22-50 mo after treatment FU, follow up; RCT, randomized controlled trial; OSA, obstructive sleep apnea; ME, upper airway myofunctional exercise; CPAP, continuous positive airway pressure; AT, adeno-tonsillectomy.
전후 연구에서 무호흡-저호흡 지수의 변화량(2편)은
-10.11에서 0.4이었고(전·후 차이: 1편
P<0.001, 1편
P=0.291), 2편 모두에서 산소포화도는 유의하게 개선되었
다. 주간졸리움의 변화량(2편)은 -4.5에서 -1.8이었다(전·
후 차이: 모두 P<0.001). 상기도 근기능 개선과 관련하여 중
재 전보다 후에 Modified Mallampati Index가 유의하게 감
소하였다.
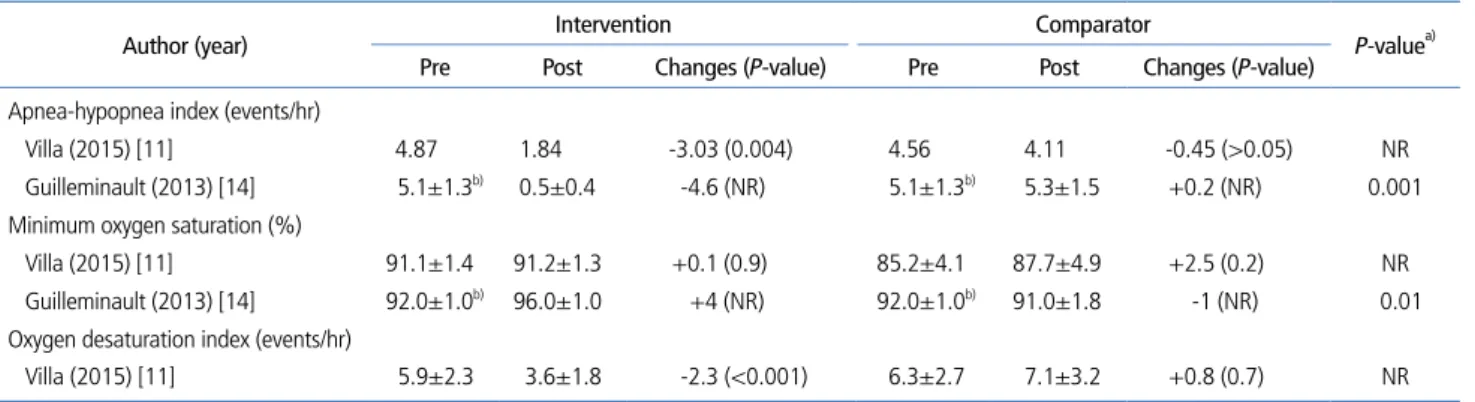
소아 대상 연구는 총 3편이었다(RCT 2편, 후향적 코호트
1편). 이 중 2편은 아데노이드편도절제술 후 보조시술로써
상기도 근기능 운동을 시행하였다. 무호흡-저호흡 지수의
시술 전·후 변화량(2편)은 중재군 -4.6에서 -3.03, 비교
군 -0.45에서 0.2이었다(군간 차이: 1편 P<0.001, 1편 보
고 안됨). 최저 산소포화도는 결과가 이질적이었고(군간 차
이: 1편 P=0.01, 1편 유사함), 최저, 평균 산소포화도 및
Table 4. Symptom improvement after upper airway myofunctional exercise (adult patients)
Author (year) Intervention Comparator P-valuea) Pre Post Changes (P-value) Pre Post Changes (P-value)
Apnea-hypopnea index (events/hr)
Diaferia (2017) [7] 30.4±19.8b) 28.0±22.7 3.4±2.7b) 13.9±18.5 -27 (<0.001) -14.1 (<0.001) 34.4±22.4b) 27.8±20.3 4.3±4.0b) 30.6±21.8 -30.04 (<0.001) +2.8 (>0.05) >0.05 <0.001 Ieto (2015) [10] Median 25.4
(22.1-28.7) Median 18.1 (15.4~24.1) -7.3 (0.017) Median 25.3 (22.1-29.8) Median 21.1 (18.2-28.1) -4.2 (>0.05) >0.05 Guimaraes (2009) [12] 22.4±4.8 13.7±8.5 -8.7 (<0.01) 22.4±5.4 25.9±8.5 +3.5 (>0.05) <0.001 Mohamed (2017) [5] 22.51±5.03c) 46.10±21.1d) 12.40±5.12 c), 42.80±15.65d) -10.11(<0.001) c) -3.3 (>0.05)d) NA NA NA NA Verma (2016) [15] 20.1±9.1 19.7±9.4 -0.4 (0.291) NA NA NA NA Minimum oxygen saturation (%)
Diaferia (2017) [7] 80.5±11b) 83.7±7.7 89.3±4.1b) 84.9±8.8 +8.8 (<0.001) +1.2 (>0.05) 80.4±6.8b) 82.6±6.3 90.2±3.6b) 82.8±6.2 +9.8 (<0.001) +0.2 (>0.05) >0.05 >0.05 Ieto (2015) [10] 85.5±7.5 83.8±8.9 -1.7 (0.120) 85.1±5.8 84.0±7.6 -1.1 (0.325) >0.05 Guimaraes (2009) [12] 83.0±6.0 85.0±7.0 +2 (<0.05) 82.0±4.0 80.0±4.0 -2 (<0.05) <0.01 Mohamed (2017) [5] 83±4c) 75±5.8d) 86±5c) 78±4.9d) +3 (<0.001)c) +3 (>0.05)d) NA NA NA NA Verma (2016) [15] 87.6±1.1 88.5±1.6 +0.9 (0.006) NA NA NA NA Oxygen desaturation index (events/h)
Ieto (2015) [10] 10.8±8.8 9.7±6.0 -1.1 (0.437) 12.3±8.7 12.1±6.9 -0.2 (0.881) >0.05 Mohamed (2017) [5] 24.6±3.9c) 77±6d) 16.7±4.7c) 71±5.1d) -7.9 (<0.001)c) -6 (>0.05)d) NA NA NA NA Verma (2016) [15] 10.9±4.9 10.3±5.3 -0.6 (0.075) NA NA NA NA Time duration of saturation < 90 % (min)
Mohamed (2017) [5] 10.7±5c) 69.0±4.9d) 6.4±3.9c) 58±4.1d) -4.3 (<0.001)c) -11 (>0.05)d) NA NA NA NA Verma (2016) [15] 6.7±6.6 5.1±6.1 -1.6 (0.007) NA NA NA NA Subjective daytime sleepiness (score)
Diaferia (2017) [7] 12.0±2.6b) 13.7±3.2 7.3±5.7b) 7.5±3.7 -4.7 (< 0.001) -6.2 (< 0.001) 12.0±2.1b) 12.8±3.1 7.2±3.6b) 12.2±5.2 -4.8 (<0.001) -0.6 (>0.05) >0.05 <0.001 Ieto (2015) [10] Median 7
(3-11) Median 7 (4-10) 0 (0.084) Median 9 (7-13.5) Median 8 (3.5-12.5) -1 (0.190) >0.05 Guimaraes (2009) [12] 14.0±5.0 8.0±6.0 -6 (0.006) 14.0±7.0 12.0±6.0 -2 (0.35) <0.05 Mohamed (2017) [5] 14.0±6.0c) 20.9±6.2d) 9.5±4.9c) 18.91±5.1d) -4.5 (<0.001)c) -1.99 (>0.05)d) NA NA NA NA Verma (2016) [15] 15.4±2.3 13.6±3.1 -1.8 (< 0.001) NA NA NA NA Values are presented as mean±standard deviation or mean.
NA, not applicable.
a)Difference between two groups. b)Upper airway myofunctional exercise + continuous positive airway pressure vs. continuous positive airway pressure. c)Moderate group. d)Severe group.
탈포화지수는 시술 전보다 후에 유의하게 개선되었다(1편).
상기도 근기능 개선과 관련하여 중재군에서만 구강호흡 감
소, 입술과 혀의 근기능(근긴장, 강도, 위치)이 강화되었고,
비교군에서는 유의한 호전을 보이지 않았다(2편, 군간 차이
보고 안됨).
결론
본 연구는 체계적 문헌고찰을 통하여 폐쇄성 수면무호흡
증 환자를 대상으로 폐쇄성 수면무호흡증에 관련된 상기도
근육의 등장성, 등척성 운동을 교육하는 것에 대해 안전성
및 유효성을 평가하였다. 상기도 근기능 운동의 안전성에 대
해서 보고된 문헌은 없었으나, 동 기술은 상기도 근육 운동
을 통하여 근기능을 강화시키고 증상을 개선시키는 기술로,
환자에게 직접적인 위해가 없어 동 기술을 수행함에 있어 안
전성에 문제가 없는 것으로 평가하였다. 또한 성인 대상 문
헌에서는 단독 시행으로도 무호흡-저호흡 지수가 개선되었
고, 소아 대상 문헌에서는 단독 또는 보조적으로 시행 시 증
상을 개선하고 상기도 근기능을 강화시키는 결과가 보고되
어 동 기술을 안전성 및 유효성이 있는 기술로 평가하였다.
근거의 수준은 평가에 포함된 연구의 유형과 질 평가 결과를
고려하여 성인 대상의 경우 B로, 소아 대상의 경우 C로 평
가하였다.
Acknowledgement
This study was supported by research funds of the
Ministry of Health and Welfare.
찾아보기말: 폐쇄성 수면무호흡; 상기도 근기능 운동;
체계적 문헌고찰ORCID
Su-mi Oh, http://orcid.org/0000-0002-5220-1299 Jin-Hyeong Kim, http://orcid.org/0000-0001-5129-7762 Seok-Hyun Kim, http://orcid.org/0000-0003-1714-9824
REFERENCES
1. Chung YS. Diagnosis of obstructive sleep apnea syndrome. Hanyang Med Rev 2013;33:227-232.
2. Isidoro SI, Salvaggio A, Lo Bue A, Romano S, Marrone O, Insalaco G. Effect of obstructive sleep apnea diagnosis on health related quality of life. Health Qual Life Outcomes 2015; 13:68.
3. Min J, Kim SJ. Medical management of obstructive sleep apnea. Korean J Med 2015;89:21-26.
4. Eckert DJ, Malhotra A. Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc 2008;5:144-153.
5. Mohamed AS, Sharshar RS, Elkolaly RM, Serageldin SM. Upper airway muscle exercises outcome in patients with obstructive sleep apnea syndrome. Egypt J Chest Dis Tuberc 2017;66:121-125.
Table 5. Symptom improvement after upper airway myofunctional exercise (pediatric patients)
Author (year) Intervention Comparator P-valuea) Pre Post Changes (P-value) Pre Post Changes (P-value)
Apnea-hypopnea index (events/hr)
Villa (2015) [11] 4.87 1.84 -3.03 (0.004) 4.56 4.11 -0.45 (>0.05) NR Guilleminault (2013) [14] 5.1±1.3b) 0.5±0.4 -4.6 (NR) 5.1±1.3b) 5.3±1.5 +0.2 (NR) 0.001 Minimum oxygen saturation (%)
Villa (2015) [11] 91.1±1.4 91.2±1.3 +0.1 (0.9) 85.2±4.1 87.7±4.9 +2.5 (0.2) NR Guilleminault (2013) [14] 92.0±1.0b) 96.0±1.0 +4 (NR) 92.0±1.0b) 91.0±1.8 -1 (NR) 0.01 Oxygen desaturation index (events/hr)
Villa (2015) [11] 5.9±2.3 3.6±1.8 -2.3 (<0.001) 6.3±2.7 7.1±3.2 +0.8 (0.7) NR Values are presented as mean±standard deviation or mean.
NR, not reported.
6. Camacho M, Certal V, Abdullatif J, Zaghi S, Ruoff CM, Capa-sso R, Kushida CA. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep 2015;38:669-675.
7. Diaferia G, Santos-Silva R, Truksinas E, Haddad FLM, Santos R, Bommarito S, Gregorio LC, Tufik S, Bittencourt L. Myo-functional therapy improves adherence to continuous positive airway pressure treatment. Sleep Breath 2017;21:387-395. 8. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group.
Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 2009;62: 1006-1012.
9. Scottish Intercollegiate Guidelines Network. Critical apprai-sal notes and checklists [Internet]. Edinburgh: Scottish Inter-collegiate Guidelines Network; 2011 [cited 2019 Mar 30]. Available from: http://www.sign.ac.uk/checklists-and-notes. html.
10. Ieto V, Kayamori F, Montes MI, Hirata RP, Gregorio MG, Alencar AM, Drager LF, Genta PR, Lorenzi-Filho G. Effects of oropharyngeal exercises on snoring: a randomized trial. Chest 2015;148:683-691.
11. Villa MP, Brasili L, Ferretti A, Vitelli O, Rabasco J, Mazzotta AR, Pietropaoli N, Martella S. Oropharyngeal exercises to reduce symptoms of OSA after AT. Sleep Breath 2015;19:281-289.
12. Guimaraes KC, Drager LF, Genta PR, Marcondes BF, Lorenzi-Filho G. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am J Respir Crit Care Med 2009;179:962-966.
13. Villa MP, Evangelisti M, Martella S, Barreto M, Del Pozzo M. Can myofunctional therapy increase tongue tone and reduce
symptoms in children with sleep-disordered breathing? Sleep Breath 2017;21:1025-1032.
14. Guilleminault C, Huang YS, Monteyrol PJ, Sato R, Quo S, Lin CH. Critical role of myofascial reeducation in pediatric sleep-disordered breathing. Sleep Med 2013;14:518-525.
15. Verma RK, Johnson J JR, Goyal M, Banumathy N, Goswami U, Panda NK. Oropharyngeal exercises in the treatment of obstructive sleep apnoea: our experience. Sleep Breath 2016; 20:1193-1201.
Peer Reviewers’ Commentary
이 논문은 신의료기술로 평가된 폐쇄성 수면무호흡증 환자에 대 한 상기도 근기능 운동의 안정성과 유효성에 대해 소개하고 있 다. 체계적인 문헌고찰 보고지침에 따라 평가한 결과, 환자에게 직접적인 위해가 없었고, 성인에서는 단독 시행으로도 무호흡-저호흡 지수가 개선되었고, 소아에서는 단독 또는 보조적으로 시 행 시 증상을 개선하고 상기도 근기능을 강화시키는 결과가 나 타나는 것으로 보고되고 있어 안전성 및 유효성이 있는 기술로 평가하고 있다. 아직 폐쇄성 수면무호흡환자에서 많이 사용되고 있지는 않으나 이 논문을 통해 안전성과 유효성이 있음을 알림 으로써, 앞으로 성인과 소아 폐쇄성 수면무호흡 환자에서 보조 치료방법으로 상기도 근기능 강화운동을 시행하는 것이 환자의 증상 개선에 유용한 신의료기술이 될 수 있을 것으로 판단된다. [정리: 편집위원회]