상악 소구치 발치 후
전치의 후방견인에 따른 입술 변화
연세대학교 대학원
치 의 학 과
허 재 욱
상악 소구치 발치 후
전치의 후방견인에 따른 입술 변화
지도교수 김 경 호
이 논문을 석사 학위논문으로 제출함
2011년 6월 일
연세대학교 대학원
치 의 학 과
허 재 욱
허재욱의 석사 학위논문을 인준함
심사위원
인
심사위원
인
심사위원
인
연세대학교 대학원
2011년 6월 일
감사의 글
이 논문이 완성 될 수 있게 해 주신 하나님께 감사드립니다. 제게 새로운 배움의 길을 열어 주시고, 석사과정 2 년 동안 과분할 만큼 관심과 사랑을 베풀어 주신 존경하는 김경호 교수님께 마음 깊이 감사드립니다. 부족한 논문을 세심하게 심사해 주시고 조언을 아끼지 않으신 정주령 교수님과 최윤정 교수님께도 감사드리며, 항상 따뜻한 가르침과 학문적 깊이로 감동을 주시는 교정학 교실의 박영철 교수님, 백형선 교수님, 황충주 교수님, 유형석 교수님, 이기준 교수님, 차정열 교수님께도 감사드립니다. 또한 많은 시간을 들여 자료 정리를 도와준 한세민 선생님께도 감사드립니다. 부족한 아들을 끝없이 용서하고 사랑하며 위해서 기도해 주시는 아버지 어머니께 이 논문이 한가지 기쁨이 되길 원하며, 항상 걱정해 주시고 격려해 주시는 아버님, 어머님께도 감사 말씀을 올립니다. 이 논문이 나오기까지 모든 과정에서 기쁨과 고통을 함께 나누었고 언제나 기꺼이 힘과 위로가 되어준 나의 사랑, 나의 은인, 내 아내 최연미에게 이 논문을 바칩니다. 2011 년 6 월 저자 씀차 례
감사의 글 그림 및 표 차례 ··· ii 국문요약 ··· iii I. 서론 ··· 1 II. 연구 대상 및 방법 ··· 4 1. 연구대상 ··· 4 2. 연구방법 ··· 5 3. 통계처리 ··· 9 III. 연구결과 ··· 10 1. 편악발치군, 양악발치군 간 치료 전후 계측치 비교 ··· 10 2. 치아 이동량과 입술 이동량 간 비율 ··· 12 3. 전치와 입술 이동량 간의 상관관계 ··· 13 4. 다중회귀분석 ··· 14 IV. 총괄 및 고찰 ··· 15 V. 결론 ··· 20 참고문헌 ··· 21 영문요약 ··· 25그림 차례
Fig. 1. Reference lines and measurement points ··· 7 Fig. 2. Measurements of lip thickness and lip area ··· 8
표 차례
Table 1. Mean age and number of subjects ··· 4 Table 2. Comparison of skeletal and dental cephalometric measurements of each
group before treatment ··· 5 Table 3. Definition of reference planes, cephalometric landmarks and
measurement parameters··· 6 Table 4. Comparison of post treatment skeletal and dental changes of cephalometric
measurements between Mx ext and Mx & Mn ext group ··· 10 Table 5. Comparison of post treatment soft tissue changes of cephalometric
measurements between Mx ext and Mx & Mn ext group ··· 11 Table 6. Ratios of the amount of incisor retraction to lip retraction ··· 12 Table 7. Pearson correlation coefficients between the amount of incisor
reraction and lip retraction ··· 13 Table 8. Regression model fit test by ANOVA ··· 14 Table 9. Regression parameter estimates and significance test ··· 14
국문요약
상악 소구치 발치 후 전치의 후방견인에 따른 입술 변화
본 연구는 성장이 완료된 골격성 II급 부정교합 환자에서 상악 소구치를 발치하고 교정치료를 시행한 경우의 상하순 변화를 파악하기 위하여 시행되었다. 연세대학교 강남세브란스병원에서 2001년 1월부터 2010년 10월까지 교정치료를 받은 환자들 중 성장이 끝난 골격성 II급 부정교합 환자군을 대상으로, 상악 제1소구 치만 발치한 48명(남성 17명, 여성 31명, 평균 ANB 5.29°)과 상하악 제1소구치를 발치한 60명(남성 25명, 여성 35명, 평균 ANB 5.53°)을 비교하였다. 교정치료 전후 에 채득한 측모두부방사선사진을 계측하여 편악발치군과 양악발치군에서 상하악 치아 의 이동에 따른 상하순의 변화를 비교하였으며 치아의 후방이동량에 따른 상하순의 이동량의 비율을 구하여 다음과 같은 결과를 얻었다. 1. 편악발치군의 치아 이동에 따른 입술의 이동 비율은 상악(Incisal edge:Labrale superious) 2.09:1, 하악(Incisal edge:Labrale inferious) 0.59:1 이었다. 2. 양악발치군의 치아 이동에 따른 입술의 이동 비율은 상악 2.31:1, 하악 1.31:1 이었다. 3. 상악전치 절단연의 이동량과 상순(Labrale superious) 이동량의 상관계수는 편악발치군 0.704, 양악발치군 0.648 이었고 (p < 0.05), 하악전치 절단연의 이동량과 하순(Labrale inferious)이동량의 상관계수는 편악발치군 0.770, 양악발치군 0.826 이었다 (p < 0.05). 4. 편악발치군에서 하순의 수직길이가 증가하였다. 핵심되는 말 : 소구치 발치, 입술, 견인, 이동 비율, 제 II 급 부정교합상악 소구치 발치 후
전치의 후방견인에 따른 입술 변화
연세대학교 대학원 치의학과
<지도교수 : 김경호>
허재욱
I.
서론
교정치료의 성공 여부는 안면 연조직의 바람직한 변화와 밀접하게 연관되어 있다(Bravo 1994, 31-42). Rudee(Rudee 1964, 421-434)는 사람들이 교정치료를 받고 싶도록 만드는 것은 안면의 조화를 개선시키려는 욕구이며, 안면의 조화란 치아들 간의 조화, 얼굴 외면의 요소들 간의 조화, 치아와 안면 연조직 간의 미적인 비율 등이라고 하였다. 환자들의 교정치료에 대한 욕구가 가지런한 치아의 배열과 안모의 개선을 위한 것이라면, 교정의는 진단과 치료계획 수립 시 치아와 안면 연조직 간의 심미적인 관계에 대한 각별한 고려와 함께 연조직의 변화 양상을 예측할 수 있어야 한다(Kang, Kim, and Choy 2000, 185-196).1900년대 Angle(Angle 1907)의 발치 불가론이 있었으나 이후 교정치료를 위해 발치가 필요한가에 대해 많은 논쟁이 있었고, Tweed(Tweed 1944, 405-428) 등 많은 선학들이 심미적으로 좋은 안모를 위해 발치가 필요하다고 보고한 이후 오늘날 많은 경우에 소구치 발치를 통한 교정치료를 시행하고 있다. 소구치 발치 후 전치부의 이동과 그에 따른 연조직 외형의 변화에 대해 많은 연구가 있었으며(Case 1964, 660-691) 전치부의 이동에 따른 얼굴 외형의 변화 양상에 대해서 다양한
의견들이 발표되었다(Drobocky, and Smith 1989, 220-30). LaMastra(LaMastra 1981, 416-23)는 연조직과 하부 경조직은 높은 상관관계를 가지고 변화하므로 연조직 측모의 예측이 가능하다고 하였으나, 경조직의 변화에 따른 연조직의 변화가 항상 예측 가능하지는 않다는 연구들도 있었다(Burstone 1967, 262-84, Hershey 1972, 45-54, Roos 1977, 165-75, Rudee 1964, 421-434, Subtelny 1961, 105-22, Wisth 1974, 199-204). Burstone(Burstone 1967, 262-84)은 안모의 연조직이 항상 경조직의 직접적 영향을 받지는 않는다고 하였고 Subtelny(Subtelny 1961, 105-22)는 연조직의 성장이 부위에 따라 하부 경조직과 긴밀한 연관을 보이기도 하지만 모든 부분이 일치하지는 않는다고 하였으며 Wisth(Wisth 1974, 199-204)는 개개인의 연조직의 다양성이 너무 커서 연조직 변화를 예측하는 것은 불가능하다고 하였다. 경조직 이동에 대한 연조직의 반응이 다양한 것에 대해, Leonardi 등(Leonardi et al. 2010, 211-216)은 경조직 변화와 그에 따른 연조직 변화 사이에 깊은 상관관계가 있는지에 대해 많은 논쟁이 있으며, 여러 연구들이 상반된 결과를 보이게 만드는 가장 큰 원인은, 많은 연구들이 성장기 환자를 대상으로 함으로써 성장에 의한 변화와 교정치료에 따른 변화를 구별하지 못한 것이라 하였다. Hershey(Hershey 1972, 45-54)도 교정치료의 효과로 외형 변화가 일어나는 것을 관찰하기 위해서는 성장의 영향이 배제되도록 실험군을 정해야 한다고 하였으나, 실제로는 성장의 영향을 배제한, 치아 이동만의 효과에 의한 연조직 변화를 다룬 연구가 많지 않다. 연조직, 특히 하안면 부위의 심미성은 코, 입술, 턱의 조화에 의해 결정된다고 할 수 있다(Kim, and Ryu 1994, 135-147, Ricketts 1968, 272-89). Burcal 등(Burcal, Laskin, and Sperry 1987, 666-670)은 사람들이 코나 턱의 변화보다 입술의 변화에 더 주목한다고 하였다. 대부분의 사람들이 입이 많이 튀어나온 것을 좋아하지 않으므로(Ricketts 1968, 272-89) 발치를 통한 교정치료 시에 전치의 후방이동에 따라 입술도 따라 이동하기를 기대하게 된다. 많은 연구들이 발치를 통한 교정치료시 상하악 전치와 상하순의 이동량 간 비율을 구하였는데, 치아 이동량 대
입술 이동량의 비율을 Sohn과 Park(Sohn, and Park 1984, 429-38)은 상악 3.8:1, 하악 1.6:1로 보고하였고 Kim과 Park(Kim, and Park 1994, 149-159)은 상악 2.84:1, 하악 1.45:1로, Rudee(Rudee 1964, 421-434)는 상악 2.93:1, 하악 0.59:1로 보고하였으며, Roos(Roos 1977, 165-75)는 상악 2.5:1, 하악 1.1:1로, Kim과 Ryu(Kim, and Ryu 1994, 135-147)는 상악 4.7:1, 하악 2:1로 보고하였다. 발치를 동반한 교정치료시 상악 소구치만 발치하는 치료도 종종 행해진다. 큰 수평피개를 갖는 증례를 교정적으로 절충치료 할 때 다양한 발치 패턴이 존재하며(Gianelly 2001, 564), 하악궁에 총생이 존재하지 않거나 돌출도의 수정을 위한 하악절치의 재위치가 요구되지 않는 경우에는 상악 편악발치에 의한 교정치료가 선택적으로 시행된다(Kim et al. 2007, 421-431). Tadic과 Woods(Tadic, and Woods 2007, 808-816)는 성장이 종료된 제II급 부정교합 환자에 있어서 수평피개가 크거나 제I급 견치관계를 얻기 위해 기능적 장치를 사용한 치료가 실패한 경우, 악교정 수술의 대안으로 상악 편악 소구치 발치가 선택될 수 있다고 하였다. 하지만 발치를 동반한 교정치료 후 연조직의 변화를 연구한 문헌들 대부분이 상하악 소구치를 함께 발치한 경우를 대상으로 하고 있고, 대부분 제I급 부정교합자의 연구에 편중되어 있어, 제II급 부정교합자에서 상악 소구치만 발치한 교정치료시의 경조직과 연조직 변화의 관계를 연구한 문헌은 거의 없는 실정이다. 본 연구는 성장이 끝난 골격성 II급 부정교합 환자들 중에서, 상악 제1소구치만 발치하고 치료한 교정환자와, 상악과 하악 제1소구치를 함께 발치한 환자를 대상으로 전치부의 이동과 그에 따른 하안면부 연조직의 변화를 관찰하고 이들 사이의 상관관계를 살펴보기 위해 시행하였다.
II. 연구 대상 및 방법
1. 연구대상
2001년 1월부터 2010년 10월까지 연세대학교 강남세브란스병원에서 교정치료를 받은 환자들 중 상악 제1소구치를 발치하고 교정치료를 진행하여 치료가 완료된 48 명을 선정하여 편악발치군으로 하고 상하악 제1소구치를 발치하여 치료한 60명을 양악발치군으로 하였다. 초진시 골격성 II급 부정교합 환자로 진단되고 수완부골 방사선사진에서 SMI (skeletal maturation index)(Fishman 1982, 88-112) 10 이후였으며, 상하악 고정식 교정장치를 사용하여 교정치료를 받은 사람들을 선정하였다. 전체 연구대상을 편악발치군과 양악발치군으로 분류한 뒤 각각을 남녀로 구분하여 총 4개의 군으로 분류하였다연구대상의 수와 연령 분포는 Table 1과 같으며 초진시 각 그룹별 주요 골격 및 치아 계측치는 Table 2와 같다.
Table 1. Mean age and number of subjects (unit : years)
Male Female
Mean SD Mean SD
Mx ext 21.45 5.17 (n=17) 26.33 9.36 (n=31) Mx & Mn ext 20.41 4.29 (n=25) 26.07 9.16 (n=35)
SD indicates standard deviation; Mx ext, extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars
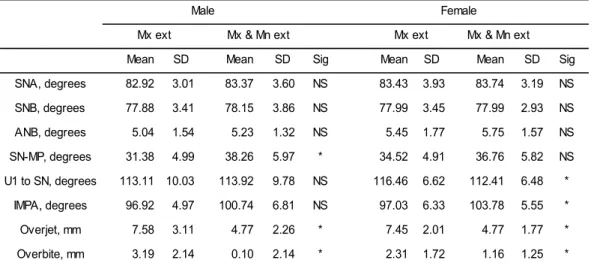
Table 2. Comparison of skeletal and dental cephalometric measurements of each group before treatment
SD indicates standard deviation; Sig, significance; NS, not significant; Mx ext, extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars; SN, sella-nasion plane; MP, mandibular plane; U1, upper central incisal edge; IMPA, incisal mandibular plane angle; * p < 0.05
2. 연구방법
가. 측모 두부방사선사진 계측
교정치료 전, 후에 rest position에서 촬영된 측모 두부방사선 사진을 V-Ceph 6.0 (OSSTEM IMPLANT co., Ltd. Seoul, Korea) 프로그램을 이용하여 tracing 후 25개의 선계측, 8개의 각계측, 2개의 면적 계측을 행하였다. 계측시 사용된 용어들의 정의는 Table 3과 같다. 확대율은 100% 가 되도록 촬영된 X-ray 이미지의 ruler를 이용해 V-Ceph 프로그램 내에서 조정 하였다.
모든 계측은 1인의 조사자가 하였으며 2주 간격으로 2회 계측을 통해 측정오류에 대한 검정을 시행하여 유의한 오차가 없음을 확인하였다.
Mean SD Mean SD Sig Mean SD Mean SD Sig SNA, degrees 82.92 3.01 83.37 3.60 NS 83.43 3.93 83.74 3.19 NS SNB, degrees 77.88 3.41 78.15 3.86 NS 77.99 3.45 77.99 2.93 NS ANB, degrees 5.04 1.54 5.23 1.32 NS 5.45 1.77 5.75 1.57 NS SN-MP, degrees 31.38 4.99 38.26 5.97 * 34.52 4.91 36.76 5.82 NS U1 to SN, degrees 113.11 10.03 113.92 9.78 NS 116.46 6.62 112.41 6.48 * IMPA, degrees 96.92 4.97 100.74 6.81 NS 97.03 6.33 103.78 5.55 * Overjet, mm 7.58 3.11 4.77 2.26 * 7.45 2.01 4.77 1.77 * Overbite, mm 3.19 2.14 0.10 2.14 * 2.31 1.72 1.16 1.25 * Male Female
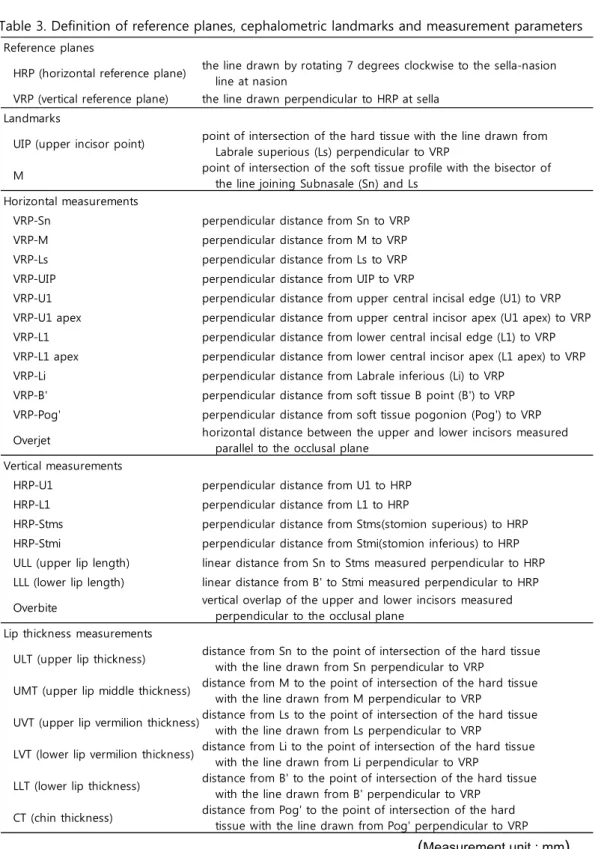
Table 3. Definition of reference planes, cephalometric landmarks and measurement parameters
(Measurement unit : mm)
Reference planes
HRP (horizontal reference plane) the line drawn by rotating 7 degrees clockwise to the sella-nasion line at nasion VRP (vertical reference plane) the line drawn perpendicular to HRP at sella
Landmarks
UIP (upper incisor point) point of intersection of the hard tissue with the line drawn from Labrale superious (Ls) perpendicular to VRP M point of intersection of the soft tissue profile with the bisector of the line joining Subnasale (Sn) and Ls Horizontal measurements
VRP-Sn perpendicular distance from Sn to VRP VRP-M perpendicular distance from M to VRP VRP-Ls perpendicular distance from Ls to VRP VRP-UIP perpendicular distance from UIP to VRP
VRP-U1 perpendicular distance from upper central incisal edge (U1) to VRP VRP-U1 apex perpendicular distance from upper central incisor apex (U1 apex) to VRP VRP-L1 perpendicular distance from lower central incisal edge (L1) to VRP VRP-L1 apex perpendicular distance from lower central incisor apex (L1 apex) to VRP VRP-Li perpendicular distance from Labrale inferious (Li) to VRP
VRP-B' perpendicular distance from soft tissue B point (B') to VRP VRP-Pog' perpendicular distance from soft tissue pogonion (Pog') to VRP Overjet horizontal distance between the upper and lower incisors measured parallel to the occlusal plane Vertical measurements
HRP-U1 perpendicular distance from U1 to HRP HRP-L1 perpendicular distance from L1 to HRP
HRP-Stms perpendicular distance from Stms(stomion superious) to HRP HRP-Stmi perpendicular distance from Stmi(stomion inferious) to HRP ULL (upper lip length) linear distance from Sn to Stms measured perpendicular to HRP LLL (lower lip length) linear distance from B' to Stmi measured perpendicular to HRP Overbite vertical overlap of the upper and lower incisors measured perpendicular to the occlusal plane Lip thickness measurements
ULT (upper lip thickness) distance from Sn to the point of intersection of the hard tissue with the line drawn from Sn perpendicular to VRP UMT (upper lip middle thickness) distance from M to the point of intersection of the hard tissue with the line drawn from M perpendicular to VRP UVT (upper lip vermilion thickness)distance from Ls to the point of intersection of the hard tissue with the line drawn from Ls perpendicular to VRP LVT (lower lip vermilion thickness) distance from Li to the point of intersection of the hard tissue with the line drawn from Li perpendicular to VRP LLT (lower lip thickness) distance from B' to the point of intersection of the hard tissue with the line drawn from B' perpendicular to VRP CT (chin thickness) distance from Pog' to the point of intersection of the hard tissue with the line drawn from Pog' perpendicular to VRP
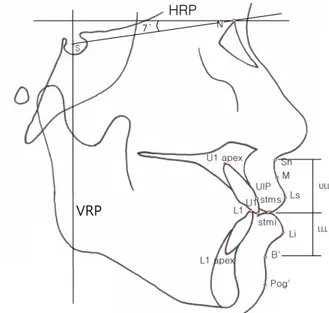
나. 기준선 설정 및 수평, 수직 선계측 (Fig. 1)
Sella-Nasion line에서 nasion 기준으로 후상방 7도 올린 선을 수평기준선(HRP), Sella에서 수평기준선에 내린 수선을 수직기준선(VRP)으로 하였다.
수평 계측항목들로는 Sn (Subnasale), M, Ls (Labrale superious), UIP, U1 (Upper central incisal edge), U1 apex (Upper central incisor apex), L1 (Lower central incisal edge), L1 apex (Lower central incisor apex), Li (Labrale inferious), B' (soft tissue B point), Pog' (soft tissue Pogonion)의 수직 기준선 까지의 거리를 계측하고 overjet을 계측하였다. 이중 UIP, M의 정의는 다음과 같다. - UIP (Upper incisor point) : Ls에서 VRP에 내린 수선이 경조직과 처음 만나는 점 - M : Sn과 Ls를 연결한 선의 수직이등분선이 연조직 외형과 만나는 점
수직 계측항목으로는, U1, L1, Stms(stomion superious), Stmi(stomion inferious)의 수평기준선까지의 거리와 overbite을 계측하고 ULL, LLL을 측정하였다. - ULL (Upper lip length) : HRP에 수직이 되도록 측정한 Sn과 Stms 사이의 거리 - LLL (Lower lip length) : HRP에 수직이 되도록 측정한 B'와 Stmi 사이의 거리
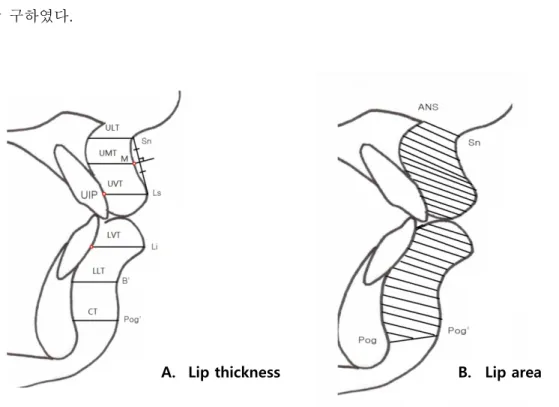
다. 입술 두께 및 면적 계측 (Fig. 2)
입술 및 이부의 두께를 상하악 3 부위에서 각각 측정하였다.
Sn, M, Ls, Li, B', Pog'에서 수직기준선에 내린 수선이 경조직과 처음 만나는 점까지의 거리를 계측하고 그 길이를 각각 ULT, UMT, UVT, LVT, LLT, CT로 명명하였다.
또한, 상순면적(전방은 연조직 line, 후방은 경조직 line과 상순의 하후방 line, 하방은 상순하연, 상방은 Sn-ANS line)과 하순면적(전방은 연조직 line, 후방은 경조직 line과 하순의 상후방 line, 하방은 Pog-Pog’line, 상방은 하순 상연)을 각각 구하였다.
Fig. 2 Measurements of lip thickness (A) and lip area (B).
See table 3 for lip thickness measurement parameters. Upper lip area was outlined anteriorly by the soft-tissue line, posteriorly by the hard-tissue line and the lower posterior third of the upper lip outline, inferiorly by the upper lip border, and superiorly by the line connecting Sn and ANS. Lower lip area was outlined anteriorly by the soft-tissue line, posteriorly by the hard-tissue line and the upper posterior third of the lower lip outline, superiorly by the lower lip border, and inferiorly by the line connecting Pog and Pog'
B. Lip area A. Lip thickness
라. 각도계측
SNA, SNB, ANB, SN-MP, Nasolabial angle, Mentolabial angle, U1 to SN, IMPA 에 대한 8개의 각계측을 시행하였다.
3. 통계처리
PASW Statistics 18(IBM Corporation, NY, USA) 프로그램을 이용하여 다음과
같은 항목들에 대해 통계처리를 하였으며 p < 0.05 시 유의한 차이가 있는 것으로 보았다. - 남, 녀 각각에서 편악발치군과 양악발치군의 치료 전후 변화량 차이를 independent t-test를 이용해 유의성 검정하였다. - 남녀 편악발치군과 양악발치군에서 상악 전치와 상순 이동량 간의 비율(U1:Ls, UIP:Ls), 하악 전치와 하순 이동량 간의 비율(L1:Li), 상악 전치와 하순 이동량 간의 비율(U1:Li)을 각각 구하였다. - 남녀 편악발치군과 양악발치군에서 상악전치와 상순, 하악 전치와 하순, 상악 전치와 하순의 이동량 간 상관관계를 Pearson 상관계수를 이용해 분석하였다. - 상악에서 치아와 입술 이동량 간의 비율에 영향을 미치는 요소들을 찾아보기 위해 다중 회귀분석을 시행하였다. 편악발치군과 양악발치군 각각에서 상순(Ls) 이동량을 상악 전치(UIP)의 이동량으로 나눈 값, 즉 상악 치아 1mm 이동시의 상순 이동량을 종속변수로 하고 초진시의 계측치들 중 하악 전치의 위치와 관련된 L1, VRP-L1 apex, HRP-VRP-L1, IMPA를 제외한 나머지를 독립변수로 하여 계단식 다중회귀 분석(stepwise multiple regression analysis)을 시행하였다. 상악 전치 이동량 계측의 기준을 U1으로 하였을 때는 적합한 모델이 산출되지 않아 UIP를 상악 전치 이동의 기준으로 하여 분석하였다.
III. 연구결과
1. 편악발치군, 양악발치군 간 치료 전후 계측치 비교
가. 골격, 치아 변화
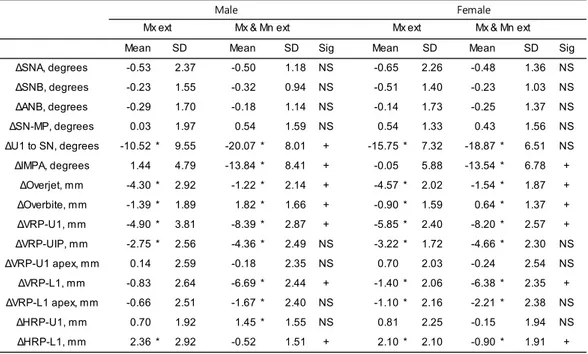
IMPA, overjet, overbite, 상하악 전치의 수평 위치, 하악 전치의 수직위치 등의 치료 전후 변화량이 남녀 모두에서 편악발치군과 양악발치군 간에 유의한 차이를 보였다 (p < 0.05). 골격관련 계측치들(SNA, SNB, ANB, SN-MP)과 상악 전치
절단연의 수직적 위치 변화량(ΔHRP-U1)은 편악발치군과 양악발치군 간에 유의차가
없었다 (p > 0.05) (Table 4).
Table 4. Comparison of post treatment skeletal and dental changes of cephalometric measurements between Mx ext and Mx & Mn ext group
SD indicates standard deviation; Sig, significance; NS, not significant; Mx ext, extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars; Δ, change of each measurements between before
and after treatment; SN, sella-nasion plane; MP, mandibular plane; U1, upper central incisal edge; VRP, vertical reference plane; HRP, horizontal reference plane; UIP, point of intersection of the hard tissue with the line drawn from Labrale superious perpendicular to VRP; L1, lower central incisal edge; IMPA, incisal mandibular plane angle; * p < 0.05(significant difference between before and after treatment measurements); + p < 0.05(significant difference between Mx ext and Mx & Mn ext group); See Table 3 for measurement parameters
Mean SD Mean SD Sig Mean SD Mean SD Sig ∆SNA, degrees -0.53 2.37 -0.50 1.18 NS -0.65 2.26 -0.48 1.36 NS ∆SNB, degrees -0.23 1.55 -0.32 0.94 NS -0.51 1.40 -0.23 1.03 NS ∆ANB, degrees -0.29 1.70 -0.18 1.14 NS -0.14 1.73 -0.25 1.37 NS ∆SN-MP, degrees 0.03 1.97 0.54 1.59 NS 0.54 1.33 0.43 1.56 NS ∆U1 to SN, degrees -10.52 * 9.55 -20.07 * 8.01 + -15.75 * 7.32 -18.87 * 6.51 NS ∆IMPA, degrees 1.44 4.79 -13.84 * 8.41 + -0.05 5.88 -13.54 * 6.78 + ∆Overjet, mm -4.30 * 2.92 -1.22 * 2.14 + -4.57 * 2.02 -1.54 * 1.87 + ∆Overbite, mm -1.39 * 1.89 1.82 * 1.66 + -0.90 * 1.59 0.64 * 1.37 + ∆VRP-U1, mm -4.90 * 3.81 -8.39 * 2.87 + -5.85 * 2.40 -8.20 * 2.57 + ∆VRP-UIP, mm -2.75 * 2.56 -4.36 * 2.49 NS -3.22 * 1.72 -4.66 * 2.30 NS ∆VRP-U1 apex, mm 0.14 2.59 -0.18 2.35 NS 0.70 2.03 -0.24 2.54 NS ∆VRP-L1, mm -0.83 2.64 -6.69 * 2.44 + -1.40 * 2.06 -6.38 * 2.35 + ∆VRP-L1 apex, mm -0.66 2.51 -1.67 * 2.40 NS -1.10 * 2.16 -2.21 * 2.38 NS ∆HRP-U1, mm 0.70 1.92 1.45 * 1.55 NS 0.81 2.25 -0.15 1.94 NS ∆HRP-L1, mm 2.36 * 2.92 -0.52 1.51 + 2.10 * 2.10 -0.90 * 1.91 +
Mx ext Mx & Mn ext Mx ext Mx & Mn ext Male Female
나. 연조직 변화
Li와 B’는 양악발치군에서 유의하게 더 많이 후방이동 되었으며 B’에서의 하순 두께(LLT)가 양악발치군에서 유의성 있게 더 감소하였다(p <0.05)(Table 5).
Table 5. Comparison of post treatment soft tissue changes of cephalometric measurements between Mx ext and Mx & Mn ext group
SD indicates standard deviation; Sig, significance; NS, not significant; Mx ext, extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars; Δ, change of each
measurements between before and after treatment; Sn, subnasale; Ls, Labrale superious; Li, Labrale inferious; M, point of intersection of the soft tissue profile with the bisector of the line joining Sn and Ls; VRP, vertical reference plane; HRP, horizontal reference plane; Stms, stomion superious; Stmi, stomion inferious; UIP, point of intersection of the hard tissue with the line drawn from Labrale superious perpendicular to VRP; L1, lower central incisal edge; IMPA, incisal mandibular plane angle; * p < 0.05(significant difference between before and after treatment measurements); + p < 0.05 (significant difference between Mx ext and Mx & Mn ext group); See
Mean SD Mean SD Sig Mean SD Mean SD Sig ∆Nasolabial angle, degrees 6.33 * 6.08 8.37 * 6.98 NS 4.82 * 6.86 9.06 * 6.77 + ∆Mentolabial angle, degrees 6.72 * 10.21 5.68 * 11.15 NS 9.59 * 12.56 4.64 * 12.96 NS
∆VRP-Sn, mm -0.66 1.91 -0.95 * 1.29 NS -0.43 1.41 -0.71 * 1.58 NS ∆VRP-M, mm -1.64 * 2.07 -2.29 * 2.09 NS -1.80 * 1.29 -2.55 * 1.94 NS ∆VRP-Ls, mm -2.59 * 2.58 -3.52 * 2.07 NS -2.66 * 1.63 -3.64 * 2.36 NS ∆VRP-Li, mm -1.57 * 2.58 -4.89 * 2.24 + -2.31 * 1.95 -5.05 * 2.43 + ∆VRP-B', mm -0.54 2.53 -2.27 * 2.00 + -0.86 2.36 -2.88 * 2.41 + ∆VRP-Pog', mm -0.76 3.13 -1.19 * 2.33 NS -0.49 2.50 -1.31 * 2.54 NS ∆ULL, mm 0.05 1.62 0.57 * 1.17 NS 0.38 * 1.12 0.10 1.41 NS ∆LLL, mm 0.84 * 1.64 -0.52 2.56 NS 1.57 * 1.87 0.66 * 1.78 NS ∆HRP-Stms, mm 0.98 2.00 1.59 * 1.33 NS 1.16 * 1.72 0.85 * 2.05 NS ∆HRP-Stmi, mm 0.23 2.29 -0.65 2.22 NS 0.03 2.51 -1.18 * 3.04 NS ∆ULT, mm 0.19 1.73 -0.07 1.23 NS 0.06 2.08 0.19 1.73 NS ∆UMT, mm -0.85 * 1.43 -0.58 1.64 NS -0.81 * 1.41 -1.24 * 1.33 NS ∆UVT, mm -0.45 1.91 -0.10 2.15 NS 0.12 1.75 0.02 1.69 NS ∆LVT, mm -1.27 * 1.39 -1.13 1.93 NS -1.35 * 2.03 -0.75 2.83 NS ∆LLT, mm -0.21 0.91 -1.56 1.32 + -0.27 1.11 -1.31 2.39 + ∆CT, mm -0.53 1.23 -0.31 1.72 NS 0.28 1.39 -0.54 2.22 NS ∆Upper lip area, mm² 4.95 25.52 16.46 * 30.96 NS 7.93 29.25 3.98 29.27 NS ∆Lower lip area, mm² 1.35 26.25 -12.21 33.22 NS -2.92 30.52 -18.19 * 26.75 +
Male Female Mx ext Mx & Mn ext Mx ext Mx & Mn ext
2. 치아 이동량과 입술 이동량 간 비율
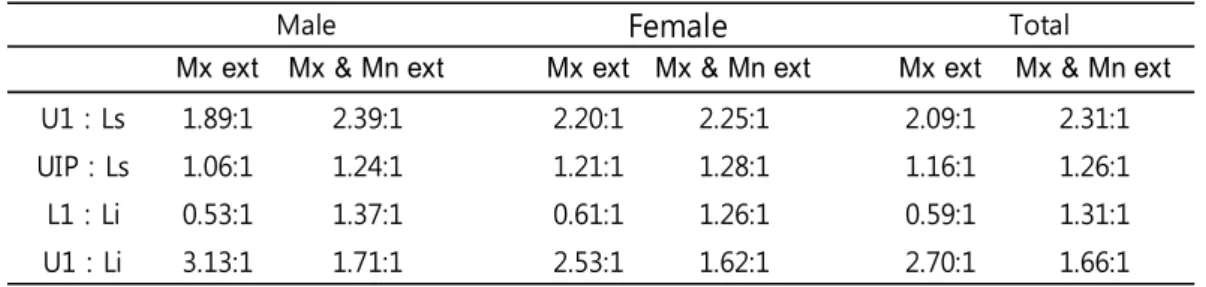
상악 전치와 상순 이동량 간의 비율(U1:Ls)은 남성에서 편악발치군 1.89:1, 양악 발치군 2.39:1 이었으며, 여성에서는 편악발치군 2.20:1, 양악발치군 2.25:1 이었다. 상악전치 이동량 계측기준을 UIP로 한 경우의 비율(UIP:Ls)은 남,녀 편악발치군이 각각 1.06:1, 1.21:1, 남,녀 양악발치군이 각각 1.24:1, 1.28:1 이었다. 하악전치와 하순 이동량 간의 비율(L1:Li)은 남성에서 편악발치군 0.53:1, 양악발치군 1.37:1, 여성에서 편악발치군 0.61:1, 양악발치군 1.26:1을 각각 나타냈다. 상악 전치와 하순 이동량 간의 비율(U1:Li)은 남성에서 편악발치군 3.13:1, 양악발치군 1.71:1 이었으며 여성에서 편악발치군 2.53:1, 양악발치군 1.62:1 이었다(Table 6).Table 6. Ratios of the amount of incisor retraction to lip retraction
Mx ext indicates extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars; U1, upper central incisal edge; Ls, Labrale superious; UIP, point of intersection of the hard tissue with the line drawn from Labrale superious perpendicular to vertical reference plane; L1, lower central incisal edge; Li, Labrale inferious; See Table 3 for measurement parameters
Mx ext Mx & Mn ext Mx ext Mx & Mn ext Mx ext Mx & Mn ext
U1 : Ls 1.89:1 2.39:1 2.20:1 2.25:1 2.09:1 2.31:1
UIP : Ls 1.06:1 1.24:1 1.21:1 1.28:1 1.16:1 1.26:1
L1 : Li 0.53:1 1.37:1 0.61:1 1.26:1 0.59:1 1.31:1
U1 : Li 3.13:1 1.71:1 2.53:1 1.62:1 2.70:1 1.66:1
3. 전치와 입술 이동량 간의 상관관계
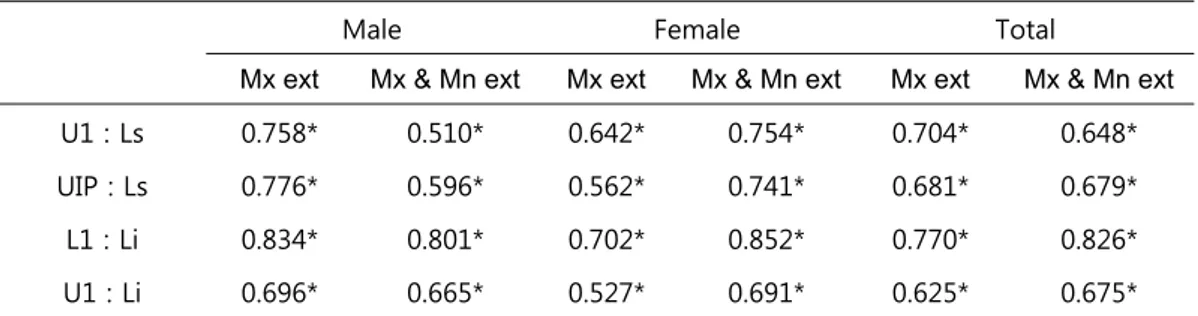
상악 전치 절단의 이동량과 Ls의 이동량, 하악 전치 절단의 이동량과 Li 이동량 간의 Pearson 상관계수를 구하였다(Table 7). 편악발치군에서 상악 0.704, 하악 0.770의 상관계수를 보였으며 양악발치군에서는 상악 0.648, 하악 0.826 이었다(p < 0.05). UIP 의 이동량과 Ls 이동량 간의 상관계수는 편악발치군 0.681, 양악발치군은 0.679 이었다(p < 0.05). 상악절치 절단과 Li 간의 상관계수는 편악발치군 0.625, 양악발치군 0.675 였다(p < 0.05).Table 7. Pearson correlation coefficients between the amount of incisor retraction and lip retraction
Male Female Total
Mx ext Mx & Mn ext Mx ext Mx & Mn ext Mx ext Mx & Mn ext U1 : Ls 0.758* 0.510* 0.642* 0.754* 0.704* 0.648* UIP : Ls 0.776* 0.596* 0.562* 0.741* 0.681* 0.679* L1 : Li 0.834* 0.801* 0.702* 0.852* 0.770* 0.826* U1 : Li 0.696* 0.665* 0.527* 0.691* 0.625* 0.675*
Mx ext indicates extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars; U1, upper central incisal edge; Ls, Labrale superious; UIP, point of intersection of the hard tissue with the line drawn from Labrale superious perpendicular to vertical reference plane; L1, lower central incisal edge; Li, Labrale inferious; * p < 0.05; See Table 3 for measurement parameters
4. 다중회귀분석
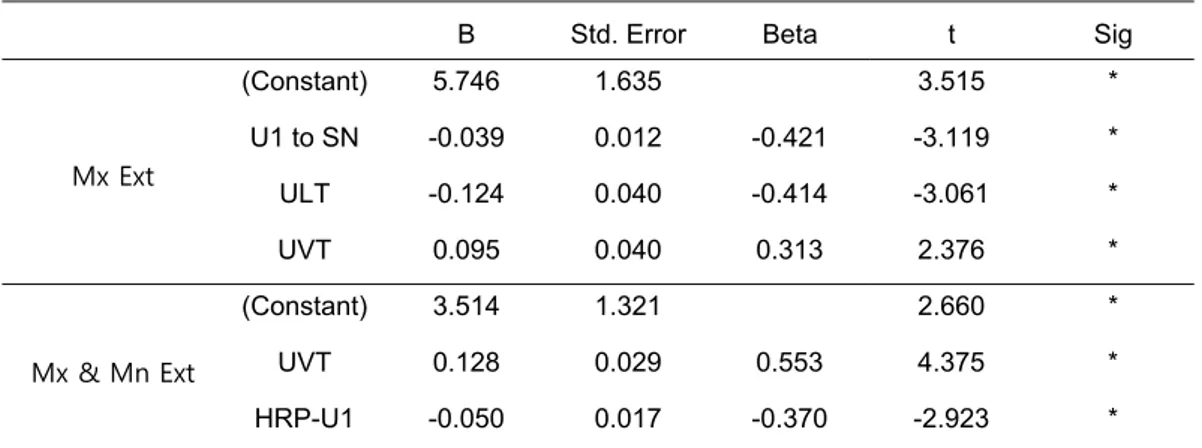
Ls 이동량을 UIP 이동량으로 나눈 값을 종속변수로 하여 그 값이 0 미만인 경우 즉, 치아 이동 방향과 반대로 입술이 이동한 경우는 종속변수 값을 0으로, 3 이상인 경우 즉, 치아 이동량의 세배 이상 입술이 이동한 경우는 3으로 수정하여 계단식 다중회귀분석(stepwise multiple regression analysis)을 시행한 결과가 Table 8, Table 9와 같다. 편악발치군에서는 U1 to SN, ULT, UVT가 입술/치아 이동량 비율에 영향을 주고 양악발치군에서는 UVT, U1의 초진시 수평기준선 까지의 거리(HRP-U1)가 영향을 주는 것으로 나타났다. 회귀계수가 UVT는 양(+)의 값을 가져 UVT가 크면 치아 이동량 대비 입술 이동량이 증가하는 것으로 나타났고, 회귀식에 포함된 나머지 변수들은 회귀계수가 음(-)의 값을 가져, 변수값이 작을수록 입술 이동량이 증가하는 것으로 나타났다.
Table 8. Regression model fit test by ANOVA
F value Sig R Square Adjusted R Square Mx Ext 6.248 * 0.319 0.268 Mx & Mn Ext 10.2 * 0.264 0.238
Sig indicates Significance; Mx ext, extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars; * p < 0.05
Table 9. Regression parameter estimates and significance test
B Std. Error Beta t Sig
Mx Ext (Constant) 5.746 1.635 3.515 * U1 to SN -0.039 0.012 -0.421 -3.119 * ULT -0.124 0.040 -0.414 -3.061 * UVT 0.095 0.040 0.313 2.376 * Mx & Mn Ext (Constant) 3.514 1.321 2.660 * UVT 0.128 0.029 0.553 4.375 * HRP-U1 -0.050 0.017 -0.370 -2.923 *
Sig indicates significance; B, unstandardized coefficients; Beta, standardized coefficients; Mx ext, extraction of upper premolars only; Mx & Mn ext, extraction of upper and lower premolars; * p < 0.05; See Table 3 for measurement parameters
IV. 총괄 및 고찰
상하악 소구치를 발치한 교정치료의 결과로 나타나는 하안면부 연조직 외형의 변화를 설명하려는 노력들이 많이 있었다. 그 중에서도 전치의 견인에 따라 입술이 견인되는 비율을 언급한 문헌들이 많이 있었는데(Kim, and Park 1994, 149-159, Kim, and Ryu 1994, 135-147, Roos 1977, 165-75, Rudee 1964, 421-434, Sohn, and Park 1984, 429-38), 대부분의 문헌들이 상순에 비해 하순이 치아 이동량 대비 더 많이 이동되는 것으로 보고하였으며 상악에서는 입술의 이동량이 치아의 이동량보다 적다고 하였다. 상순의 이동량이 상악 전치 이동량에 미치지 못하는 원인으로는 상순의 두께(Anderson, Joondeph, and Turpin 1973, 324-36, Ricketts 1960, 103-33), 입술의 strain(Oliver 1982, 141-9), 개개인의 해부학적 형태의 다양성(Subtelny 1961, 105-22, Wisth 1974, 199-204) 등이 보고되었다. 상하악 소구치를 발치한 경우와 상악 소구치만 발치한 경우를 비교한 본 연구에서도 치아 이동에 대해 편악, 양악발치군 모두 상순보다 하순의 이동량이 많은 것으로 나타났다. 전치 절단을 기준으로 했을 때 상악은 편악발치군 2.09:1, 양악발치군 2.31:1로 치아 대 입술 이동량 비율이 큰 차이가 없었으나 하악은 편악발치군 0.59:1, 양악발치군 1.31:1로 두 군 사이에 상당한 차이가 있어서, 편악발치군이 하악전치 이동량 대비 하순의 이동량이 더 많은 것으로 나타났다. 하악전치의 견인량이 크지 않은 편악발치군에서 하순의 이동량이 적지 않은 것은, 하순의 이동이 하악 전치 뿐 아니라 상악 전치의 이동에도 영향을 받은 결과로 이해할 수 있을 것이다. Angle(Angle 1907)은 하순의 곡선을 결정하는 것은 하악 치아가 아니라 상악 치아라고 하였고 Rudee(Rudee 1964, 421-434)는 상악 절치와 하순 이동량간 상관계수가 0.4885 이며 이동량간 비율도 평균 1:1로 직접적인 연관성을 갖는다고 하였다. O’Reilly(O'Reilly Proportional Changes of Hard and Soft Tissue Profiles as a Result of Orthodontic Treatment, Master’s Thesis, University of Washington, Seattle)도 상악 절치와 하순간에 0.481의 상관계수를 보고하였다. 본
연구에서는 상악전치 절단과 하순 사이의 Pearson 상관계수가 편악 발치군에서 0.625, 양악 발치군에서는 0.675를 나타내었다. 상악전치 절단과 하순의 이동 비율은 편악발치군(2.70:1)이 양악 발치군(1.66:1) 만큼 치아 이동량 대비 입술 이동량이 크지는 않았으나 편악발치군에서 거의 이동하지 않는 하악 전치를 생각할 때 상당량의 이동을 보인 것으로 판단할 수 있다. 입술 이동량이 치아 이동량에 미치지 못하는 경우는 그 차이만큼 입술이 두꺼워 졌거나 치아 이동량이 입술 이동과 직접 연관되지 않은 위치에서 계측된 것으로 볼 수 있을 것이다. Ricketts(Ricketts 1960, 103-33)와 Anderson(Anderson, Joondeph, and Turpin 1973, 324-36)은 상악 절치 후방견인시 상순의 두께가 증가하여 치아의 이동량 만큼 상순 전돌의 양상이 감소하지 않는다고 하였으며 Kim과 Ryu(Kim, and Ryu 1994, 135-147)는 상하악 소구치를 발치한 제I급 부정교합 환자의 연구에서 치료후 홍순부 두께증가를 보고하였다. 그러나 본 연구에서는 상순 이동량 계측의 기준이 되는 Ls 부위에서의 상순 두께(UVT)가 남녀 편악, 양악 발치군 모두에서 치료 전후 큰 변화가 없었으며, 이는 상순이 직하방의 경조직 이동량과 비슷한 양만큼 이동한 것으로 생각할 수 있다. 본 연구에서는 전체 sample의 78.7%가 치료후 UVT의 변화량이 초진시 두께의 20% 이내였으며 전체 sample의 50% 에서는 변화량이 10% 이내였다. 치아 이동에 대한 입술 이동량의 비율을 언급한 대부분의 문헌들이 전치 절단을 치아 이동의 기준으로 삼았다. 그러나, 교정치료의 주된 대상이 되는 젊은 연령에서는 상악 전치 절단보다는 상순 직하방의 치아 순면이 상순에 직접 접촉하기 때문에 입술의 이동에 더 직접적인 영향을 줄 수 있으리라 생각된다. 본 연구에서 상악전치 절단을 치아이동 계측의 기준으로 할 때보다, Ls와 같은 수평면상에 있는 UIP를 기준으로 삼았을 때 치아 이동량 대 입술 이동량의 비율이 편악발치군 1.16:1, 양악발치군 1.26:1로서, 상악전치 절단을 기준으로 할 때의 편악, 양악발치군 각각 2.09:1, 2:31:1 보다 1:1에 더 근접하였다. 상순 두께가 크게 변화하지 않았는데도 불구하고 UIP를 기준으로 했을 때보다 전치 절단을 기준으로 했을 때 치아 이동에 대한 입술 이동량이 적게 나타나는 것은, 치체 이동보다는 경사 이동의 경향이 더
강한 상악 전치의 견인양상으로 인해 실제 상순의 이동에 영향을 주는 정도보다 상악 전치 이동량이 더 크게 계측되어서 나타나는 결과라 할 수 있겠다. 따라서 상악 전치의 절단보다는 UIP를 상악 전치 이동의 기준으로 했을 때 좀 더 예측 가능한 치아와 입술 이동량 간 비율이 표현된다고 하겠다. Ls와의 상관계수는 편악발치군에서 UIP와 상악 전치 절단이 각각 0.681과 0.704, 양악발치군에서는 0.679와 0.648로, UIP와 전치 절단 간에 큰 차이가 없었다. 그러나 UIP는 Ls의 수직위치나 치아 이동에 따라 변화될 수 있는 위치여서 일관성 있는 측정이 쉽지 않아 임상적으로 적용하기에는 한계가 있다고 하겠다. Hershey(Hershey 1972, 45-54)는 상악 전치 치관의 최전방점을 UIP라 하여 치아 이동의 기준을 삼은 바 있으나 본 연구에서와 달리 상순의 위치를 고려하지 않은 계측점이다. 입술의 이동에 직접적인 관련이 있고, 보다 재현성이 있는 상악 전치 계측점에 대한 연구가 필요하리라 생각된다. 상악 전치 이동에 대한 상순의 이동량에 영향을 주는 요소를 확인하기 위해 다중회귀분석을 시행하였다. Talass 등(Talass, Talass, and Baker 1987, 385-94)은 상순의 이동량을 종속변수로 한 회귀분석을 통해 상순 이동량에 영향을 주는 변수들을 구하였다. 본 연구에서는 입술 이동량 자체보다는, 치아 이동 정도에 입술이 따라서 이동하는 비율에 주목하기 위해 종속변수로서 입술 이동량 대신 치아의 단위 이동량 당 입술이 이동한 양을 선택하였다. UIP나 Ls의 이동량이 극히 적은 경우의 계측오차로 인한 오류를 보정하기 위해 Ls의 이동량을 UIP의 이동량으로 나눈 종속변수 값이 0 미만, 즉 치아이동과 반대로 입술이 이동한 것으로 나타난 경우는 종속변수 값을 0으로, 종속변수 값이 3 이상, 즉 치아 이동량의 3배 이상 입술이 이동한 것으로 표현된 경우는 3으로 종속변수 값을 변환해 분석하였다. 편악발치군에서는 U1 to Sn, ULT, UVT가 영향을 주는 독립변수로 나왔고 양악발치군에서는 UVT와 U1의 수평기준선 까지의 거리(HRP-U1)가 영향을 주는 변수인 것으로 나타났다. Oliver(Oliver 1982, 141-9)는 입술이 두꺼운 군과 얇은 군 각각에서 치아 이동량과 상순 이동량 간의 상관계수를 구했을 때 상순이 얇은 경우 상악 전치 이동량과 상순 이동량 사이의 상관관계가 더 크다고 하였다. 반면에,
Talass 등(Talass, Talass, and Baker 1987, 385-94)은 상순이 두꺼운 경우에 상악치아 견인에 따라 상순이 더 많이 이동하며 subnasale 부위 연조직이 얇을수록 상순이 더 많이 이동한다고 하였다. 본 연구의 계단식 다중회귀분석 결과 편악발치군에서는 subnasale 부위에서의 입술 두께를 나타내는 ULT는 얇을수록, Ls에서의 입술 두께인 UVT는 두꺼울수록 치아 견인량 대비 입술 견인량이 증가하는 것으로 나타나 Talass 등(Talass, Talass, and Baker 1987, 385-94)의 보고와 같은 결과를 보였다. 양악발치군에서도 UVT가 두꺼울수록 입술 견인량이 증가하는 것으로 나타났으나 ULT는 영향을 주는 변수로 나타나지 않았다.
전치 이동에 따른 상순 이동량의 남녀간 차이에 대해 Angelle(Angelle 1973, 267-80)는 전치부 후방이동시 남자에서 상순이 더 많이 후방이동 한다고 하였고 Bishara(Bishara, Cummins, and Zaher 1997, 18-27)는 II급 1류 부정교합자의 발치와 비발치 치료에 대한 비교연구에서 남녀간에는 교정치료 후 연조직 변화의 차이가 없다고 하였다. 본 연구에서 편악발치군(남 1.89:1, 여 2.20:1)에서는 남자에서 상순이 더 많이 후방이동 하였으나 양악발치군(남 2.39:1, 여 2.25:1)에서는 남녀간 차이가 크지 않았다. 편악발치군과 양악발치군 모두 상순의 수직적 길이 변화는 크지 않았으며 이는 상하악 소구치를 발치한 환자에서 전치의 후방견인으로 인해 상순의 길이가 변화하지 않는다는 Kang 등(Kang, Kim, and Choy 2000, 185-196)의 연구와 일치하였다. 그러나 편악발치군에서는 하순의 수직적 길이가 남성 0.69mm, 여성 1.57mm 증가했는데 Talass 등(Talass, Talass, and Baker 1987, 385-94)은 II급 1류 여성 부정교합 환자 대상의 연구에서 발치를 통한 교정치료 후 상순 길이는 변하지 않으나 하순 길이는 증가한다고 하였다. 하순의 수직길이는 편악발치군에서 치료 후
유의하게 증가하였으며(남성 0.84±1.64mm, 여성 1.57±1.87mm, p < 0.05)
양악발치군에서는 남성은 유의성있는 변화가 없었고 여성에서는 유의하게
증가하였다(0.66±1.78mm, p < 0.05). 본 연구에서는 입술의 수직적 변화와 lip incompetency의 관계는 고려하지 않았으나 Kim과 Ryu(Kim, and Ryu 1994, 135-147)는 양악 전돌증 환자에서 소구치 발치시 redundant lip 보다는 incompetent
lip에서 상순의 수직길이의 증가가 크다고 하였고, Hershey(Hershey 1972, 45-54)는 redundant lip과 incompetent lip 간에 치아 견인에 따른 입술의 변화 양상이 차이가 없다고 하였다
본 연구에서는 측모 두부방사선사진을 이용하여 2차원적으로 치아와 입술의 변화를 분석하였으나, 오늘날 급속도로 그 기술이 발전하고 있는 3차원적 분석도구를 응용한 추가적인 연구가 진행되길 기대한다.
V. 결론
본 연구는 성장이 완료된 골격성 II급 부정교합 환자에서 상악 제1소구치 혹은 상하악 제1소구치를 발치하고 교정치료를 시행한 남녀를 대상으로 치료 전, 후 측모두부 방사선 사진을 계측하여 전치의 후방견인에 따라 나타나는 입술주위 연조직의 변화를 남녀, 편악발치군과 양악발치군으로 구분해 비교 관찰하여 다음과 같은 결과를 얻었다. 1. 편악발치군의 치아 이동에 따른 입술의 이동 비율은 상악(Incisal edge:Labrale superious) 2.09:1, 하악(Incisal edge:Labrale inferious) 0.59:1 이었다.2. 양악발치군의 치아 이동에 따른 입술의 이동 비율은 상악 2.31:1, 하악 1.31:1 이었다. 3. 상악전치 절단연의 이동량과 상순(Labrale superious) 이동량의 상관계수는 편악발치군 0.704, 양악발치군 0.648 이었고 (p < 0.05), 하악전치 절단연의 이동량과 하순(Labrale inferious)이동량의 상관계수는 편악발치군 0.770, 양악발치군 0.826 이었다 (p < 0.05). 4. 편악발치군에서 하순의 수직길이가 증가하였다.
참고문헌
Anderson, J. P., D. R. Joondeph and D. L. Turpin. 1973. "A cephalometric study of profile changes in orthodontically treated cases ten years out of retention". The Angle Orthodontist, 43(3): 324-36.
Angelle, P. L. 1973. "A cephalometric study of the soft tissue changes during and after orthodontic treatment". Transactions. European Orthodontic Society: 267-80.
Angle, E. H. 1907. Treatment of malocclusion of the teeth : Angle's system. 7th Ed. Philadelphia, Pa.: The S.S. White Dental Manufacturing.
Bishara, S. E., D. M. Cummins and A. R. Zaher. 1997. "Treatment and posttreatment changes in patients with Class II, Division 1 malocclusion after extraction and nonextraction treatment". American journal of orthodontics and dentofacial orthopedics, 111(1): 18-27.
Bravo, L. A. 1994. "Soft tissue facial profile changes after orthodontic treatment with four premolars extracted". The Angle orthodontist, 64(1): 31-42.
Burcal, R. G., D. M. Laskin and T. P. Sperry. 1987. "Recognition of profile change after simulated orthognathic surgery". Journal of Oral and Maxillofacial Surgery, 45(8): 666-670.
Burstone, C. J. 1967. "Lip posture and its significance in treatment planning". American journal of orthodontics, 53(4): 262-84.
Case, C. S. 1964. "The question of extraction in orthodontia". American journal of orthodontics, 50(9): 660-691.
Drobocky, O. B. and R. J. Smith. 1989. "Changes in facial profile during orthodontic treatment with extraction of four first premolars". American journal of orthodontics and dentofacial orthopedics, 95(3): 220-30.
Fishman, L. S. 1982. "Radiographic evaluation of skeletal maturation. A clinically oriented method based on hand-wrist films". The Angle orthodontist, 52(2): 88-112. Gianelly, A. A. 2001. "Bidimensional technique theory and practice". American Journal of Orthodontics and Dentofacial Orthopedics, 119: 564.
Hershey, H. G. 1972. "Incisor tooth retraction and subsequent profile change in postadolescent female patients". American journal of orthodontics, 61(1): 45-54. Kang, C. S., K. H. Kim and K. C. Choy. 2000. "The vertical changes of the lip and perioral soft tissue resulting from incisor retraction". Korean journal of orthodontics, 30(2): 185-196.
Kim, H. D. and Y. C. Park. 1994. "The study of comparison before and after orthodontic treatment in class I bialveolar protrusion cases with four bicuspid extraction". Korean journal of orthodontics, 24(1): 149-159.
Kim, T. K. and Y. K. Ryu. 1994. "LIP PROFILE CHANGES AFTER ORTHODONTIC TOOTH MOVEMENT IN FEMALE ADULT WITH BIMAXILLARY PROTRUSION". Korean journal of orthodontics, 24(1): 135-147.
Kim, Y. S., S. J. Kim, S. G. Kang and Y. J. Lee. 2007. "A comparative study of pre- and post-treatment cephalometric measurements: Upper premolar extraction only vs. upper/lower premolar extraction groups". Korean journal of orthodontics 37(6): 421-431.
LaMastra, S. J. 1981. "Relationships between changes in skeletal and integumental points A and B following orthodontic treatment". American journal of orthodontics, 79(4): 416-23.
Leonardi, R., A. Annunziata, V. Licciardello and E. Barbato. 2010. "Soft tissue changes following the extraction of premolars in nongrowing patients with bimaxillary protrusion". The Angle Orthodontist, 80(1): 211-216.
O'Reilly, W. C. Proportional Changes of Hard and Soft Tissue Profiles as a Result of Orthodontic Treatment, Master’s Thesis, University of Washington, Seattle.
Oliver, B. M. 1982. "The influence of lip thickness and strain on upper lip response to incisor retraction". American journal of orthodontics, 82(2): 141-9.
Ricketts, R. M. 1960. "The influence of orthodontic treatment on facial growth and development". The Angle Orthodontist, 30(3): 103-33.
───. 1968. "Esthetics, environment, and the law of lip relation". American journal of orthodontics, 54(4): 272-89.
Roos, N. 1977. "Soft-tissue profile changes in class II treatment". American journal of orthodontics, 72(2): 165-75.
Rudee, D. A. 1964. "Proportional profile changes concurrent with orthodontic therapy". American journal of orthodontics, 50(6): 421-434.
Sohn, B. H. and Y. C. Park. 1984. "A Roentgenocephalometric Study of Teeth and Profile Changes in Orthodontically Treated Patient with Four Bicuspid Extraction". The journal of the Korean dental association, 25: 429-38.
Subtelny, J. D. 1961. "The soft tissue profile, growth and treatment changes". The Angle Orthodontist, 31(2): 105-22.
Tadic, N. and M. G. Woods. 2007. "Incisal and soft tissue effects of maxillary premolar extraction in Class II treatment". The Angle Orthodontist, 77(5): 808-816.
Talass, M. F., L. Talass and R. C. Baker. 1987. "Soft-tissue profile changes resulting from retraction of maxillary incisors". American journal of orthodontics and dentofacial orthopedics, 91(5): 385-94.
Tweed, C. H. 1944. "Indications for the extraction of teeth in orthodontic procedure". American journal of orthodontics and oral surgery, 30: 405-428.
Wisth, J. 1974. "Soft tissue response to upper incisor retraction in boys". British journal of orthodontics, 1(5): 199-204.
ABSTRACT
Lip change following incisor retraction after
upper premolar extraction
Huh, Jae Wook Dept. of Dentistry The Graduate School Yonsei University
The purpose of this study was to investigate the changes of upper and lower lips in adult patients treated with extraction of only upper premolars.
Among Class II malocclusion patients who had been treated in Gangnam Severance Hospital, Yonsei University between January 2001 and October 2010, following subjects were selected; 48 patients(male 17, female 31, mean ANB 5.29°) treated with extraction of only upper first premolars and 60 patients(male 25, female 35, mean ANB 5.53°) treated with extraction of both upper and lower first premolars. The treatment changes of both groups were compared. Cephalometric x-ray films taken before and after orthodontic treatment were measured, upper and lower lip changes following upper and lower incisor retraction were compared between two different extraction groups in each gender group. The ratios of incisor retraction to lip retraction were calculated and the correlation coefficients were calculated.
The results were as follows.
1. The ratio of movement between incisors and lips in upper premolars only extraction group is, in maxilla (Incisal edge:Labrale superius) 2.09:1, mandible (Incisal edge:Labrale inferius) 0.59:1.
2. The ratio of movement between incisors and lips in upper and lower premolars extraction group is, in maxilla 2.31:1, mandible 1.31:1.
3. The correlation coefficients between movements of maxillary incisal edge and upper lip (Labrale superious) were 0.704 in upper premolars only extraction group, 0.648 in upper and lower premolars extraction group (p < 0.05). The correlation coefficients between movements of mandibular incisal edge and lower lip (Labrale inferious) were 0.770 in upper premolars only extraction group, 0.826 in upper and lower premolars extraction group (p < 0.05). 4. Vertical lower lip length was increased in upper premolars only extraction
group.