저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Master's Thesis in Medicine
How to approach previously diagnosed
gastric neoplasms that are not definitely
detected
in
scheduled
therapeutic
endoscopy
Graduate School of Ajou University
Department of Gastroenterology
How to Approach Previously Diagnosed
Gastric Neoplasms That Are Not Definitely
Detected
in
Scheduled
Therapeutic
Endoscopy
Sung-Jae Shin, Advisor
I submit this thesis as the
Master’s thesis in medicine
August 2019
Graduate School of Ajou University
Department of Gastroenterology
i
Abstract
-How to approach previously diagnosed gastric neoplasms that are
not definitely detected in scheduled therapeutic endoscopy
Background and aims: Endoscopists sometimes encounter unusual cases in which a previously
diagnosed gastric neoplasm is not detected in the scheduled therapeutic endoscopy. This study aimed to analyze the reasons for undetected lesions in scheduled therapeutic endoscopy and to understand how to approach such cases.
Methods: Between March 2010 and February 2018, that were previously diagnosed as gastric
neoplasms in diagnostic endoscopy were not detected in the scheduled therapeutic endoscopy. A total of 32 patients who did not meet any of the exclusion criteria were enrolled. Additionally, 1870 gastric endoscopic submucosal dissection (ESD) cases, performed in the same period, were retrospectively reviewed and compared with the enrolled cases.
Results: Compared with the 1870 conventional ESD cases, the 32 undetected gastric lesion cases
showed a significantly smaller tumor size, smaller surface area, and lower sampling ratios in univariate logistic regression analysis (p < 0.002). Multivariate logistic regression analysis showed that tumor size is a significant risk factor for undetected gastric neoplasms (p < 0.009). Of the undetected 32 lesions, 1 (3.1%) was pathologically overestimated and 1 (3.1%) seemed to be due to incorrect localization of the initial tumor. Moreover, 9 of the 32 (28.1%) lesions were partially removed at the initial endoscopic forceps biopsy (EFB) and recurred during surveillance. Among the 9 recurred cases, 2, 4, and 3 neoplasms were found by EFB at the scheduled therapeutic endoscopy, at 3 months, and at 6 months surveillance endoscopy, respectively. The mean time to the detection of gastric neoplasm was 3.0 ± 2.6 (0–6) months. Most of the undetected gastric neoplasm cases (21/32, 65.6%) seemed to be due to complete removal at the initial EFB.
Conclusions: If a gastric lesion previously detected on endoscopic screening becomes invisible, we
recommend careful surveillance endoscopy at regular intervals of at least 6 months, or at least 2 times.
Keywords: Stomach Neoplasms; Endoscopy; Neoplasms, residuel
ii
Table of contents
ABSRTRACT
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧i
TABLE OF CONTENTS
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧ii
LIST OF FIGURES
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧iii
LIST OF TABLES
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧iii
I. INTRODUCTION
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧1
II. MATERIALS AND METHODS
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧1
1. Patients ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧1
2. Diagnostic endoscopy ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧2
3. ESD procedure ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧2
4. Endoscopic features ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧2
5. Histologic features ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧3
6. Statistical analysis ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧3
III. RESULTS
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧3
1. Clinical characteristics of UGNs ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧3
2. Comparison of baseline and endoscopic features ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧5
between the UGN and conventional ESD groups
3. Analysis of factors affecting undetection ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧
6
4. Surveillance endoscopy ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧7
IV. DISCUSSION
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧8
V. REFERENCES
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧11
국문요약
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧13
iii
LIST OF FIGURES
► Figure 1. Flow chart of the enrolled study population
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧7
LIST OF TABLES
► Table 1. Clinical characteristics of patients without gastric lesions
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧4
in the scheduled therapeutic endoscopy and comparison
► Table 2. Comparison of baseline and endoscopic features
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧5
between the UGN and conventional ESD groups
► Table 3. Logistic regression analysis of risk factors
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧6
for the undetected gastric neoplasm group
► Table 4. Comparison of baseline and endoscopic features
‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧8
between the tumor recurrence group and the nonrecurrence group
1
I. INTRODUCTION
In South Korea, cancer is the leading cause of death. Stomach cancer is the most commonly diagnosed malignancy, and a screening test (endoscopy) is recommended for patients older than 40 years, every 2 years at a relatively low cost, according to the National Cancer Screening Program [1, 2]. Because of its easy accessibility, endoscopic forceps biopsy (EFB) performed by primary physicians at local clinics has enabled the early detection of many gastric adenomas (well known to be precancerous lesions) and gastric cancers. These cases are often referred to a tertiary medical center for advanced therapeutic endoscopic techniques. Currently, endoscopic mucosal resection and endoscopic submucosal dissection (ESD) are the standard therapeutic tools for gastric epithelial neoplasms, including gastric adenomas and early gastric cancer, with minimal invasiveness. Between these 2 techniques, ESD is the preferred method because it enables curative en bloc resection [3].
In some cases, initial gastric lesions recognized by EFB on screening endoscopy are not found during the scheduled therapeutic endoscopy. Thus, finding the cause and appropriate surveillance strategies for undetected gastric neoplasms (UGNs) is important. Until recently, UGNs in therapeutic endoscopy have not been investigated.
The aims of this study were to analyze the reasons for UGNs, to compare the endoscopic characteristics of patients with UGNs and those who underwent conventional gastric ESD, and to understand how to approach these uncommon cases.
II. MATERIALS AND METHODS
1. Patients
Between March 2010 and February 2018, previously detected gastric neoplasms in 55 patients were not found in the scheduled therapeutic endoscopy. A total of 32 patients with UGNs, who had undergone ESD or surveillance endoscopy with EFB at the same site at least once within 6 months after the scheduled therapeutic endoscopy, were enrolled. Among these 32 patients, 21 were referred from primary physicians and 11 received their initial diagnosis at Ajou University Hospital. Patients with insufficient documentation were excluded.
During the same period, a total 1870 consecutive patients underwent gastric ESD at the same hospital. These 1870 patients from a prospectively designed ESD database system and the enrolled 32 patients
2 with UGN were retrospectively reviewed and compared.
The Ajou University Hospital institutional review board approved our study with approval no. AJIRB-MED-MDB-19-072.
2. Diagnostic endoscopy
In the diagnostic endoscopy, lesion-targeted EFB using chromoendoscopy with indigo carmine dye spray and a narrow-band imaging system was done if gastric epithelial dysplasia was suspected. To macroscopically estimate the size of the lesion, standard biopsy forceps with a 6-mm opening diameter (FB-21K-1; Olympus, Tokyo, Japan) or 6-mm circular pieces of punched out paper were used. The number of biopsy fragments was determined by considering the size and surface morphology of the lesion.
3. ESD procedure
By using a 1-channel endoscope (GIF-H260 or GIF-Q260J, Olympus) or a 2-channel endoscope (Olympus Q260J, 2TQ260M; Olympus Optical Co., Tokyo, Japan), all ESDs were performed under sedation with both midazolam and propofol. After marking several spots 5 mm outside the lesion margin by using a FlexKnife (Olympus) or argon plasma coagulation, the standard ESD technique was performed with an IT-knife (Olympus) or FlexKnife.
4. Endoscopic features
The endoscopic variables, such as tumor size (length: long diameter), location (upper: cardia, fundus, upper body; middle: mid body, lower body, angle; lower: antrum, prepylorus), number of biopsy fragments, and sampling ratios, were analyzed and compared. The sampling ratio was calculated by dividing the length of the lesion or surface area by the number of biopsy fragments. A lower ratio implies more extensive sampling.
3
5. Histologic features
The histologic diagnoses of pre-ESD EFB specimens were confirmed by 2 experienced pathologists (D.L., Y.B.K.). Further, all EFB slides of patients referred from primary medical centers or private clinics were rechecked by the 2 pathologists to confirm the initial pathologic misdiagnosis. All gastric lesions were classified according to the revised Vienna classification of gastrointestinal neoplasia.
6. Statistical analysis
SPSS software version 23.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses. Continuous variables were presented as mean ± standard deviation, and compared using the Mann-Whitney U-test and Student’s t-test. Categorical variables were presented as the total number with percentage, and compared using the chi-square test, Fisher’s exact test, and linear-by-linear association, if required. To identify the significant endoscopic predictors of UGNs, univariate and multivariate logistic regression analyses were conducted with calculation of odds ratios (ORs) and 95% confidence intervals (CIs). Values of p < 0.05 were considered significant. The follow-up period was counted from the day of the initial therapeutic endoscopy to the day of UGN discovery by EFB or the day of the last surveillance endoscopy.
III. RESULTS
1. Clinical characteristics of UGNs
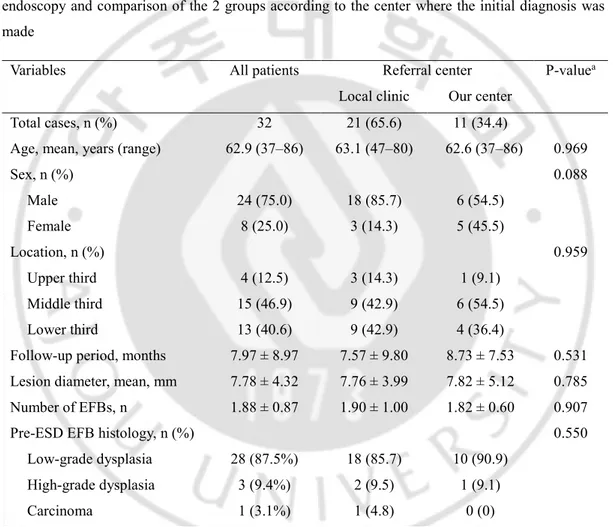
A total of 55 patients (55 cases) were discharged without undergoing a scheduled therapeutic procedure owing to the absence of the previously detected gastric lesion. Of them, 23 were excluded from this study (4: insufficient documentation, 19: no surveillance endoscopy within 6 months) and 32 patients were finally enrolled. The patients were divided into 2 groups according to the center where the initial diagnostic endoscopy was performed: 21 patients (65.6%) from local clinics and 11 patients (34.4%) evaluated at our medical center. There were no significant differences between the 2 groups (Table 1). Among the enrolled patients, 24 (75%) were men and the mean age was 62.9 (range 37–86) years. The initial location based on EFB samplings was the upper third of the stomach in 4 patients (12.5%), the middle-third portion in 15 patients (46.7%), and the lower-third portion in 13
4
patients (40.6%). The mean follow-up period was 7.97 ± 8.97 (range 3–48) months. The mean lesion size and number of EFB samplings were 7.78 ± 4.32 mm and 1.88 ± 0.87, respectively. In the initial EFB pathology, 28 lesions (87.5%) were low-grade dysplasias (LGDs), 3 (9.4%) were high-grade dysplasias (HGDs), and 1 (3.1%) was a moderately differentiated adenocarcinoma.
Table 1. Clinical characteristics of patients without gastric lesions in the scheduled therapeutic
endoscopy and comparison of the 2 groups according to the center where the initial diagnosis was made
Variables All patients Referral center P-valuea
Local clinic Our center
Total cases, n (%) 32 21 (65.6) 11 (34.4)
Age, mean, years (range) 62.9 (37–86) 63.1 (47–80) 62.6 (37–86) 0.969
Sex, n (%) 0.088 Male 24 (75.0) 18 (85.7) 6 (54.5) Female 8 (25.0) 3 (14.3) 5 (45.5) Location, n (%) 0.959 Upper third 4 (12.5) 3 (14.3) 1 (9.1) Middle third 15 (46.9) 9 (42.9) 6 (54.5) Lower third 13 (40.6) 9 (42.9) 4 (36.4)
Follow-up period, months 7.97 ± 8.97 7.57 ± 9.80 8.73 ± 7.53 0.531 Lesion diameter, mean, mm 7.78 ± 4.32 7.76 ± 3.99 7.82 ± 5.12 0.785 Number of EFBs, n 1.88 ± 0.87 1.90 ± 1.00 1.82 ± 0.60 0.907
Pre-ESD EFB histology, n (%) 0.550
Low-grade dysplasia 28 (87.5%) 18 (85.7) 10 (90.9) High-grade dysplasia 3 (9.4%) 2 (9.5) 1 (9.1)
Carcinoma 1 (3.1%) 1 (4.8) 0 (0)
n: number; ESD: endoscopic submucosal dissection; EFB: endoscopic forceps biopsy
5
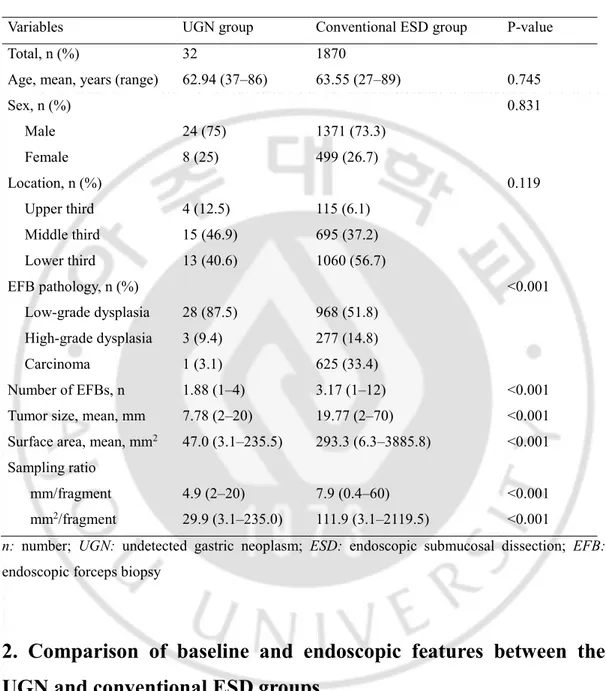
Table 2. Comparison of baseline and endoscopic features between the UGN and conventional ESD
groups
Variables UGN group Conventional ESD group P-value
Total, n (%) 32 1870
Age, mean, years (range) 62.94 (37–86) 63.55 (27–89) 0.745
Sex, n (%) 0.831 Male 24 (75) 1371 (73.3) Female 8 (25) 499 (26.7) Location, n (%) 0.119 Upper third 4 (12.5) 115 (6.1) Middle third 15 (46.9) 695 (37.2) Lower third 13 (40.6) 1060 (56.7) EFB pathology, n (%) <0.001 Low-grade dysplasia 28 (87.5) 968 (51.8) High-grade dysplasia 3 (9.4) 277 (14.8) Carcinoma 1 (3.1) 625 (33.4) Number of EFBs, n 1.88 (1–4) 3.17 (1–12) <0.001 Tumor size, mean, mm 7.78 (2–20) 19.77 (2–70) <0.001 Surface area, mean, mm2 47.0 (3.1–235.5) 293.3 (6.3–3885.8) <0.001 Sampling ratio
mm/fragment 4.9 (2–20) 7.9 (0.4–60) <0.001 mm2/fragment 29.9 (3.1–235.0) 111.9 (3.1–2119.5) <0.001
n: number; UGN: undetected gastric neoplasm; ESD: endoscopic submucosal dissection; EFB:
endoscopic forceps biopsy
2. Comparison of baseline and endoscopic features between the
UGN and conventional ESD groups
We compared the baseline and endoscopic features of the UGN group (n = 32) and the conventional ESD group (n = 1870), as shown in Table 2. In the conventional ESD group, the mean age was 63.55 (range 27–89) years and 1371 patients (73.3%) were men. Of the lesions, 1060 (56.7%), 695 (37.2%), and 115 (6.1%) were located in the lower-third, middle-third, and upper-third portions, respectively.
6
In the initial pathology based on EFB, 968 (51.8%) were LGDs, 277 (14.8%) were HGDs, and 625 (33.4%) were carcinomas. The EFB number, tumor size, and surface area were 3.17 (range 1–12), 19.77 (range 2–70) mm, and 293.3 (6.3–3885.8) mm2, respectively. The sampling ratios were 7.9 (range 0.4–60) mm/fragment and 111.9 (3.1–2119.5) mm2/fragment. Between the 2 groups, there were significant differences in EFB pathology, number of EFB, tumor size, surface area, and sampling ratios (p < 0.001).
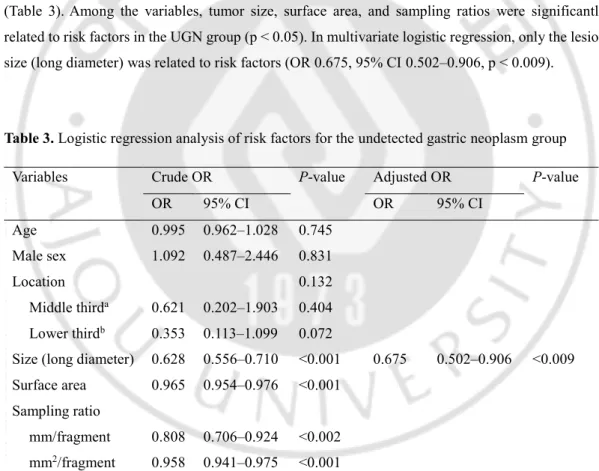
3. Analysis of factors affecting undetection
We performed univariate logistic regression to analyze the risk factors associated with the UGN group (Table 3). Among the variables, tumor size, surface area, and sampling ratios were significantly related to risk factors in the UGN group (p < 0.05). In multivariate logistic regression, only the lesion size (long diameter) was related to risk factors (OR 0.675, 95% CI 0.502–0.906, p < 0.009).
Table 3. Logistic regression analysis of risk factors for the undetected gastric neoplasm group
Variables Crude OR P-value Adjusted OR P-value
OR 95% CI OR 95% CI Age 0.995 0.962–1.028 0.745 Male sex 1.092 0.487–2.446 0.831 Location 0.132 Middle thirda 0.621 0.202–1.903 0.404 Lower thirdb 0.353 0.113–1.099 0.072
Size (long diameter) 0.628 0.556–0.710 <0.001 0.675 0.502–0.906 <0.009 Surface area 0.965 0.954–0.976 <0.001
Sampling ratio
mm/fragment 0.808 0.706–0.924 <0.002 mm2/fragment 0.958 0.941–0.975 <0.001
OR: odds ratio; CI: confidence interval
aMiddle-third lesion compared with upper-third lesion. bLower-third lesion compared with upper-third lesion.
7
4. Surveillance endoscopy
After the therapeutic endoscopy, we performed follow-up endoscopy at 3, 6, and 12 months, and annually thereafter, although some patients did not follow our surveillance protocol. Despite the absence of the original tumor, we performed EFB at the location of the previous tumor, during the scheduled therapeutic endoscopy and all surveillance endoscopies.
Among the EFB slides from private clinics, one (1/32, 3.1%) showed intestinal metaplasia, which was confirmed by our hospital pathologist and previously judged as LGD (Figure 1). In the same patient, the EFBs obtained during the scheduled therapeutic endoscopy and at the 3-month surveillance endoscopy also confirmed the lesion to be intestinal metaplasia. In another patient (1/31, 3.1%) with a previously identified gastric lesion (in the posterior wall of the upper body), a gastric neoplasm (in the posterior wall of the angle) was found in the EFB at 3 months and an ESD (posterior wall of the angle) was performed at 6 months. On the follow-up endoscopy, 9 neoplasms (9/32, 28.1%) were discovered at the same location as that of the pre-ESD EFB. In the EFB, 2 gastric neoplasms were identified on scheduled therapeutic endoscopy; 4 gastric neoplasms, on the 3-month surveillance endoscopy; and 3 gastric neoplasms, on the 6-month surveillance endoscopy. The mean time to the detection of gastric neoplasm was 3.0 ± 2.6 months (range, 0–6 months). In the other 21 neoplasms (21/32, 65.6%), we could not find any evidence of gastric tumor on surveillance endoscopy with EFB.
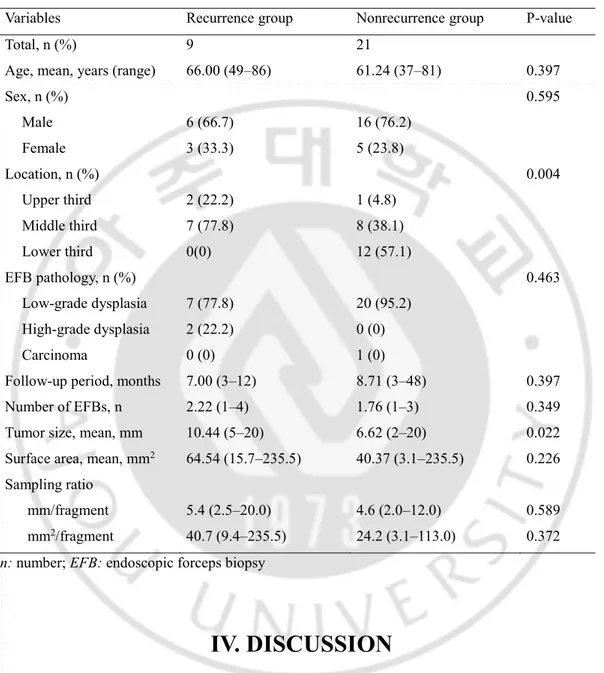
We compared the baseline and endoscopic features between the tumor recurrence and nonrecurrence groups, excluding 2 cases of overestimation and incorrect localization (Table 4). We found a significant difference in tumor size (p < 0.022).
8
Table 4. Comparison of baseline and endoscopic features between the tumor recurrence group and
the nonrecurrence group (1 overestimation and 1 incorrect localization case were excluded)
Variables Recurrence group Nonrecurrence group P-value
Total, n (%) 9 21
Age, mean, years (range) 66.00 (49–86) 61.24 (37–81) 0.397
Sex, n (%) 0.595 Male 6 (66.7) 16 (76.2) Female 3 (33.3) 5 (23.8) Location, n (%) 0.004 Upper third 2 (22.2) 1 (4.8) Middle third 7 (77.8) 8 (38.1) Lower third 0(0) 12 (57.1) EFB pathology, n (%) 0.463 Low-grade dysplasia 7 (77.8) 20 (95.2) High-grade dysplasia 2 (22.2) 0 (0) Carcinoma 0 (0) 1 (0)
Follow-up period, months 7.00 (3–12) 8.71 (3–48) 0.397
Number of EFBs, n 2.22 (1–4) 1.76 (1–3) 0.349
Tumor size, mean, mm 10.44 (5–20) 6.62 (2–20) 0.022
Surface area, mean, mm2 64.54 (15.7–235.5) 40.37 (3.1–235.5) 0.226 Sampling ratio
mm/fragment 5.4 (2.5–20.0) 4.6 (2.0–12.0) 0.589 mm2/fragment 40.7 (9.4–235.5) 24.2 (3.1–113.0) 0.372
n: number; EFB: endoscopic forceps biopsy
IV. DISCUSSION
No study has analyzed UGNs previously diagnosed on diagnostic EFB. This is the first study to assess these unusual cases, and our results might provide relevant data for establishing a guideline.
There are 4 possible reasons why previously diagnosed gastric neoplasms are not detected in the scheduled therapeutic endoscopy. First, pathologic overestimation at the initial EFB is a considerable factor. Yang et al [4] reported the rate of pathologic overestimation as 9.6% of non-neoplastic
9
pathologic cases after ESD, and Jhi et al [5] reported that 13.8% of cases were initially misdiagnosed as neoplastic lesions. In a reactive and regenerative epithelium, the cells are usually immature and lack cytoplasmic mucin, resulting in hyperchromatic nuclei. The epithelium shows a gradual transition from normal to atypical cells. The distinction between reactive/regenerative atypia and LGD can be difficult, because these histologic types often overlap in clinical practice, especially in association with substantial inflammation and/or erosion [6, 7]. Further, interobserver differences in gastric neoplasm diagnosis can result in pathologic overdiagnosis [7]. In the current study, a case (1 of 32, 3.1%) of intestinal metaplasia, upon rechecking by our experienced pathologists, was pathologically overestimated as LGD in a private clinic. This implies that careful reexamination of the pathology slide by a professional pathologist could be helpful, considering a possible pathologic misdiagnosis. Second, incorrect localization of the initial gastric lesion is another reason. Several studies have reported about the incorrect localization of the original tumor [4, 8, 9]. In this study, we found a presumptive case of incorrect localization. In the case, a primary physician indicated the presence of a gastric lesion at the posterior wall of the upper body of the stomach, with the pathology slide judged as HGD. The lesion was not found in therapeutic endoscopy performed at our hospital, and a gastric lesion was found in the posterior wall of the angle on follow-up endoscopy at 3 months. There are 2 possible explanations for why the gastric lesion at 3 months tandem endoscopy was found at a different location (posterior wall of the angle) from that of the initial lesion (posterior wall of the upper body). Incorrect indication of the original tumor location by the primary physician was possible, although we could not exclude the probability that the gastric lesion (posterior wall of the angle) at 3 months endoscopy was missed synchronous gastric neoplasm in the initial endoscopy. Several studies have reported on the synchronous multiplicity of gastric cancer in a surgically resected stomach [10-16] and the existence of missed synchronous gastric neoplasms (mSGNs) in an ESD-treated stomach [17-20]. Therefore, elaborate endoscopic examination is recommended, considering the possibility of an incorrectly indicated tumor location and of mSGNs. Third, biopsy removal of the original lesion is the other important reason. Some studies have reported on the biopsy removal of the original tumor [4, 8, 21]. Smaller tumor size, large number of biopsy fragments, and higher sampling ratios (calculated by dividing the size of the tumor or the surface area by the number of biopsy fragments) are the risk factors because these variables reflect more extensive sampling. In this study, univariate and multivariate logistic regression analyses showed the same results as other studies, in that tumor size (p < 0.001), surface area (p < 0.001), and sampling ratios (p < 0.002 and p < 0.001) were associated with the UGN group (Table 3). Therefore, we presumed that removal of the initial neoplastic foci through extensive biopsy was the main reason in most cases of UGNs. In our study, a 64-year-old male patient with LGD underwent diagnostic ESD owing to the absence of the original
10
tumor, and the ESD result was no evidence of tumor. This case was a confirmative evidence of complete biopsy removal. Fourth, the possibility of partial removal or a remnant tumor is the last reason. Nine gastric neoplasms (9/32 cases, 28.1%) at the same location of the previous lesion were found in surveillance endoscopy, and 8 of them were subjected to ESD. The neoplasm size of the tumor recurrence group was significantly greater than that of the nonrecurrence group (p < 0.022, Table 4). We assumed that the original lesion was partially removed by the initial EFB, and the remnant tumor was discovered on follow-up endoscopy.
In most of our study cases, the undetected lesion could be the result of biopsy removal. Taking into consideration the cost and discomfort for the patients raises the question of how long these unusual cases should be followed up. Endoscopists cannot ignore UGNs because the natural progression of gastric epithelial neoplasms to carcinoma is well reported [22, 23]. In this study, EFB identified 2 gastric neoplasms at the scheduled therapeutic endoscopy, 4 gastric neoplasms at 3 months surveillance endoscopy, and 3 gastric neoplasms at 6 months surveillance endoscopy. The mean interval to the discovery of gastric neoplasms was 3.0 ± 2.6 (0–6) months. According to our study, follow-up endoscopy until at least 6 months or endoscopic evaluation at least 2 times seem to be suggestive. If there is no gastric lesion after endoscopy at 6 months or >2 times of endoscopic evaluation, the complete removal of the previous gastric lesion by EFB can be presumed.
The present study has several limitations. First, interobserver differences, such as among pathologists, could have affected the initial pathologic results of EFB. Second, as the mean surveillance period, including the endoscopic resection cases, was relatively short at 7.97 months, we were not able to investigate the obvious natural course of UGNs. Third, the number of UGN cases was relatively small (n = 32) and the surveillance results might not be perfect because a few patients did not follow our protocol of surveillance endoscopy scheduled at 3, 6, and 12 months, and yearly thereafter.
In conclusion, extensive biopsy removal is the main reason for indefinite gastric lesions in the scheduled therapeutic endoscopy. Further, incorrect localization and biopsy overestimation are other possible reasons. In some cases, incompletely removed lesions on EFB are discovered in follow-up diagnostic endoscopy, requiring endoscopic resection. Although there is no gastric lesion during the therapeutic endoscopy, performing EFB at the same location of the previous lesion is recommended, owing to the possibility of remnant tumor tissue. Thereafter, regular diagnostic endoscopy with EFB should be performed until at least 6 months or at least 2 times.
11
V. REFERENCE
1. Jung, K.W., et al., Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2015. Cancer Res Treat, 2018. 50(2): p. 303-316.
2. Jung, M., National Cancer Screening Programs and evidence-based healthcare policy in South Korea. Health Policy, 2015. 119(1): p. 26-32.
3. Gotoda, T., et al., Endoscopic submucosal dissection of early gastric cancer. J Gastroenterol, 2006. 41(10): p. 929-42.
4. Yang, M.J., et al., Non-neoplastic pathology results after endoscopic submucosal dissection for gastric epithelial dysplasia or early gastric cancer. Endoscopy, 2015. 47(7): p. 598-604.
5. Jhi, J.H., et al., Negative pathology after endoscopic resection of gastric epithelial neoplasms: importance of pit dysplasia. Korean J Intern Med, 2017. 32(4): p. 647-655.
6. Goldstein, N.S. and K.J. Lewin, Gastric epithelial dysplasia and adenoma: historical review and histological criteria for grading. Hum Pathol, 1997. 28(2): p. 127-133.
7. Lauwers, G.Y. and R.H. Riddell, Gastric epithelial dysplasia. Gut, 1999. 45(5): p. 784-790.
8. Kim, E., et al., Where has the tumor gone? The characteristics of cases of negative pathologic diagnosis after endoscopic mucosal resection. Endoscopy, 2009. 41(09): p. 739-745.
9. Won, C.S., et al., Upgrade of lesions initially diagnosed as low-grade gastric dysplasia upon forceps biopsy following endoscopic resection. Gut Liver, 2011. 5(2): p. 187-93.
10. Esaki, Y., K. Hirokawa, and M. Yamashiro, Multiple gastric cancers in the aged with special reference to intramucosal cancers. Cancer, 1987. 59(3): p. 560-565.
11. Honmyo, U., et al., Clinicopathological analysis of synchronous multiple gastric carcinoma. Eur J Surg Oncol, 1989. 15(4): p. 316-321.
12. Iwafuchi, M. and H. Watanabe, Synchronous multiple early gastric cancer; study of surgically resected stomach. Nihon Rinsho, 1996. 54(5): p. 1217-1223.
13. Kodera, Y., et al., Incidence, diagnosis and significance of multiple gastric cancer. Br J Surg, 1995. 82(11): p. 1540-1543.
12 distal gastrectomy. Cancer, 1990. 65(11): p. 2602-5.
15. Mitsudomi, T., et al., A clinicopathological study of synchronous multiple gastric cancer. Br J Surg, 1989. 76(3): p. 237-240.
16. Moertel, C.G., J.A. Bargen, and E.H. Soule, Multiple gastric cancers; review of the literature and study of 42 cases. Gastroenterology, 1957. 32(6): p. 1095-103.
17. Kim, H.H., et al., Missed synchronous gastric neoplasm with endoscopic submucosal dissection for gastric neoplasm: experience in our hospital. Dig Endosc, 2013. 25(1): p. 32-38.
18. Kim, H.H., et al., Causes of missed synchronous gastric epithelial neoplasms with endoscopic submucosal dissection: a multicenter study. Scand J Gastroenterol, 2013. 48(11): p. 1339-1346.
19. Lee, H.L., et al., When do we miss synchronous gastric neoplasms with endoscopy? Gastrointest Endosc, 2010. 71(7): p. 1159-1165.
20. Yoo, J.H., et al., How can we predict the presence of missed synchronous lesions after endoscopic submucosal dissection for early gastric cancers or gastric adenomas? J Clin Gastroenterol, 2013. 47(2): p. e17-e22.
21. Kim, Y., et al., Histologic diagnosis based on forceps biopsy is not adequate for determining endoscopic treatment of gastric adenomatous lesions. Endoscopy, 2010. 42(08): p. 620-626.
22. Park, S.Y., et al., Long-term follow-up study of gastric intraepithelial neoplasias: progression from low-grade dysplasia to invasive carcinoma. Eur J Gastroenterol Hepatol, 2008. 20(10): p. 966-970.
23. Yamada, H., et al., Long-term follow-up study of gastric adenoma/dysplasia. Endoscopy, 2004. 36(05): p. 390-396.
13 -국문 요약-
진단목적의 위 내시경상 발견된 위 신생물이 치료내시경에서 명확히 관
찰되지 않는 경우 어떻게 접근할 것인가
배경 및 목표: 진단내시경에서 확인된 위 신생물이 치료내시경에서 확인되지 않는 경 우가 드물게 관찰된다. 치료내시경에서 관찰되지 않는 병변에 대한 원인을 분석하고, 어떻게 추적관찰 할 것인가 생각해보았다. 방법: 2010년 5월부터 2018년 2월까지의 기간동안, 진단 내시경에서 발견되었으나 치료 내시경에서 관찰되지 않은 55개(55명)의 위 신생물이 있었다. 이 중 배제기준을 만족하 지 않은 32개의 위신생물(32명)을 연구에 포함시켰다. 또한 동일 기간에 내시경적 점막 하 절제술을 시행한 1870개의 위신생물 사례들을 확인하고, 연구대상인 32개(32명)의 위 신생물과 비교하였다. 결과: 내시경적 점막 절제술을 시행한 1870개의 사례와 비교하였을 때, 치료내시경에서 관찰되지 않은 32개의 위 병변들은 단변량 로지스틱 회귀분석에서 통계적으로 유의하 게 작은 종양 크기, 종양 표면면적, 샘플 비를 보였다(p < 0.002). 다변량 로지스틱 회귀 분석에서는 오직 종양 크기만이 관찰되지 않는 위병변의 중요한 위험인자임에 대해 통 계적으로 의미 있었다(P < 0.009). 치료내시경에서 관찰되지 않은 위 병변 중에서, 1 (1/32, 3.1%)개는 조직학적으로 과평가 되었고, 1 (1/32, 3.1%)개는 초기 종양의 위치가 잘못 표 기된 것으로 보인다. 9 (9/32, 28.1%)개의 병변은 검사 내시경에서 생검 겸자로 부분적으 로 제거되어 치료내시경에서 관찰되지 않다가, 남은 부분이 추적관찰에서 재발한 것으14 로 보인다. 재발한 9개의 증례 중에, 2개는 치료내시경 생검에서 발견되었고, 4개의 증례 는 3개월째 추적내시경 생검에서, 3개의 증례는 6개월째 추적내시경 생검에서 발견되었 다. 진단내시경에서 관찰되지 않은 병변이 추적내시경에서 관찰될 때까지의 평균 시간 은 3.0 ± 2.6 (0–6) 개월이었다. 대부분의 관찰되지 않은 위 신생물(21/32, 65.6%)은 초기 진단 내시경에서 생검겸자에 의하여 완전히 제거된 것으로 생각된다. 결론: 진단 내시경에서 관찰된 위 병변이 치료내시경에서 관찰되지 않는 경우, 일정한 간격의 추적내시경을 6개월 이상, 또는 적어도 2회 이상의 추적내시경을 시행할 것을 권유한다.