저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게
l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다:
l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다.
l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다.
저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다.
Disclaimer
저작자표시. 귀하는 원저작자를 표시하여야 합니다.
비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다.
변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
의학박사 학위논문
소변검체에서 두 유전자 단일 튜브 이중 실시간 중합효소연쇄반응 검사를 이용한 활동성 결핵의 진단
Diagnosis of active tuberculosis using duplex, one-tube nested, real-time PCR in urine specimens
울산대학교 대학원 의학과
류지원
[UCI]I804:48009-200000337863 [UCI]I804:48009-200000337863
소변검체에서 두 유전자 단일 튜브 이중 실시간 중합효소연쇄반응 검사를 이용한 활동성 결핵의 진단
지도교수 심태선
이 논문을 의학박사 학위논문으로 제출함
2020년 8월
울산대학교 대학원 의학과
류지원
류지원의 의학박사 학위논문을 인준함
심사위원 오연목 인 심사위원 심태선 인 심사위원 최창민 인 심사위원 조경욱 인 심사위원 나주옥 인
울 산 대 학 교 대 학 원
2020년 8월
Abstracts
Background: Tuberculosis (TB) is a global health problem and the leading cause of morbidity and mortality worldwide. A delay in TB diagnosis will affect the control of the disease. Therefore, rapid, easy to perform, highly sensitive, and more accurate diagnostic tools during the early stages of infection are crucial. However, conventional smear/culture methods using sputum samples have well-known limitations of low sensitivity and prolonged result time. Furthermore, some pulmonary TB (PTB) patients cannot expectorate sputum. In addition, the diagnosis of extrapulmonary TB (EPTB) needs invasive procedures. Thus, non-sputum diagnostic methods are urgently needed. Advancements in real-time polymerase chain reaction (PCR) in detecting Mycobacterium tuberculosis(MTB)-specific trans- renal DNA (Tr-DNA) from urine, which are small DNA fragments from cells dying throughout the body, have recently been made. However, Tr-DNA-based studies have found that the sensitivity and specificity were 0.5 (95% CI: 0.36 – 0.72) and 0.94 (95% CI: 0.78 – 0.99), respectively, for a combination of PTB and EPTB specimens. Therefore, the development of more sensitive methods remains a critical goal.
Purpose: The aim of this study was to develop a new highly sensitive nucleic acid amplification test (NAAT) using duplex, one-tube nested, real-time PCR for the rapid and accurate detection of MTB in urine specimens.
Methods: Duplex, one-tube nested, real-time PCR was designed with two sequential reactions with two sets of primers and dual probes for the insertion sequences of IS6110 and rpoB in MTB. The analytical sensitivity of the assay was determined through a standard curve of 10-fold dilutions [10 ng, 1 ng, 100 pg, 10 pg, 1 pg, 100 fg, and 10 fg] of DNA isolated from the MTB H37Rv strain. Clinical specimens were used in a preliminary study to evaluate the sensitivity and specificity of the newly developed test. Sputum specimens were provided from 26
patients with culture-positive PTB and 108 healthy subjects, and urine specimens from 45 patients with culture-positive PTB and 30 healthy subjects.
Results: The Ct (cycle threshold) values for MTB H37Rv by rpoB single real-time PCR, IS6110 single real-time PCR, rpoBone-tube nested real-time PCR, IS6110 one- tube nested real-time PCR, and rpoB and IS6110 duplex, one-tube nested, real- time PCR ranged from 17.36 to 37.18, 14.95 to 34.88, 8.44 to 27.92, 5.83 to 26.36, and 4.99 to 24.99, respectively. To increase the sensitivity, the reaction protocol for the duplex, one-tube nested, real-time PCR was modulated from 10 and 40 cycle to 15 and 25 cycle and, as a result, the minimum limit of detection was changed from 10fg to 1fg, respectively. Overall, duplex, one-tube nested, real-time PCR with 15 and 25 cycle was the most sensitive assay for detecting MTB DNA. The sensitivity of the Real MTB-ID (M&D, Korea) assay, and duplex, one-tube nested, real-time PCR test was 46.2% (12/26) and 100% (26/26), respectively, for sputum specimens. In comparison, the sensitivity of the AdvanSureTM TB/ Nontuberculous mycobacterium (NTM) real-time PCR (LG Lifescience, Korea) assay, and the duplex, one-tube nested, real-time PCR test was 6.7% (3/45) and 51.1% (23/45), respectively, for urine specimens.
Conclusions: IS6110 and rpoBgene one-tube nested real-time PCR was useful for detecting MTB in urine specimens due to its relatively high sensitivity and simple manipulation compared to conventional methods.
목차
Abstracts... ⅰ
Tables and Figures... iv
Abbreviations... vi
Introduction... 1
Methods... 4
Results... 9
Discussion ... 18
Conclusion ... 25
References... 26
국문요약... 35
Tables & Figures
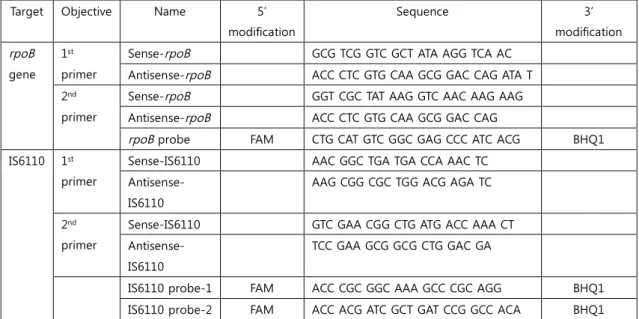
Table 1. Primers and probes used in this study. ... 8
Table 2. Limits of detection of single real-time PCR assays and one-tube nested real-time PCR for the dilution series of MTB H37Rv DNA. ...13
Table 3. Limits of detection of single real-time PCR assays and duplex, one-tube nested, real-time PCR for the dilution series of MTB H37Rv DNA...13
Table 4. The sensitivity and specificity for sputum specimens ...16
Table 5. The sensitivity and specificity for urine specimens...17
Figure 1. Amplification curves of rpoB single real-time PCR ... 9
Figure 2. Amplification curves of rpoB one-tube nested real-time PCR...10
Figure 3. Amplification curves of rpoB single real-time PCR with doubling primer concentrations. ...10
Figure 4a. Amplification curves of rpoB single real-time PCR with increasing cycles ...11
Figure 4b. Amplification curves of rpoB single real-time PCR with doubling primer concentrations and increasing cycles...11
Figure 5a. Amplification curves of rpoB one-tube nested real-time PCR with decreasing concentrations of the 1st primers (2.5 pM, 2.5 pM) ...12
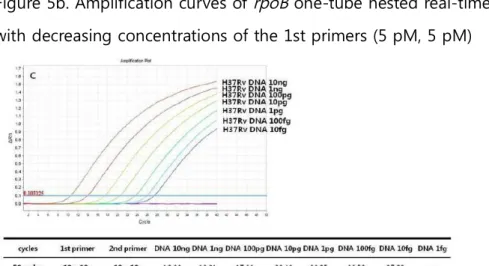
Figure 5b. Amplification curves of rpoB one-tube nested real-time PCR with decreasing concentrations of the 1st primers (5 pM, 5 pM)...12
Figure 5c. Amplification curves of rpoB one-tube nested real-time PCR (10 pM, 10 pM)...12
Figure 6. Amplification curves of IS6110 single real-time PCR ...14 Figure 7. Amplification curves of IS6110 one-tube nested real-time PCR...14 Figure 8. Amplification curves of rpoB and IS6110 duplex, one-tube nested, real- time PCR...15 Figure 9. Amplification curves of rpoB and IS6110 duplex, one-tube nested, real-
time PCR with modified cycles ...15
Abbreviations TB: Tuberculosis
MTB: Mycobacterium tuberculosis AFB: Acid-fast bacilli
NTM: Nontuberculous mycobacterium NAAT: Nucleic acid amplification test PCR: Polymerase chain reaction PTB: Pulmonary tuberculosis EPTB: Extrapulmonary tuberculosis LAM: Lipoarabinomannan
Tr-DNA: Transrenal DNA
HIV: Human immunodeficiency virus TST: Tuberculin skin test
QFT-IT: QuantiFERON○R-TB Gold In-Tube PBS: Phosphate buffer saline
Ct: Cycle threshold gDNA: genomic DNA
AlereLAM: Alere Determine TB LAM Ag
Introduction
1. Epidemiology and burden of Tuberculosis
Worldwide, tuberculosis (TB) remains a threat to global health, and is the leading cause of death, despite advances in the implementation of control strategies over the past decade. Annually, there are approximately 10 million new TB cases and 1.2 million TB-related deaths1. South Korea is an intermediate TB burden country;
about 23,000 new TB cases developed and 1,800 people died from TB in 20192,3. A delay in TB diagnosis will affect the control of the disease4,5. To control TB, timely access to a diagnosis is critical. Therefore, a highly sensitive molecular-based test for the detection of Mycobacterium tuberculosis (MTB) remains an important goal in the control and eventual eradication of the disease worldwide.
2. Traditional diagnosis of TB
The traditional diagnosis of TB is based on the detection of acid-fast bacilli (AFB) in smears, and the isolation of MTB from culture6. AFB smear microscopy, a method that was introduced over a century ago, is simple, quick, and inexpensive, but it has limited sensitivity with a detection threshold of 5000 to 10,000 AFB/mL of sputum, even when a fluorescence stain is used6. Also, the detection of AFB in smears cannot differentiate between MTB complex and nontuberculous mycobacterium (NTM)7. Mycobacterial culture is the current reference standard for the diagnosis of TB, and it is highly sensitive and detects as little as 10 AFB/mL of sputum. However, it requires up to eight weeks for a solid culture and six weeks for a liquid culture to provide results8,9. Thus, there is a need for a diagnostic test to detect TB more reliably than the AFB smear, but with similar turnaround time.
Such demands have led to the development of the nucleic acid amplification test (NAAT), which is likely to meet the requirements10,11. Polymerase chain reaction (PCR), one of the representative NAATs, can amplify targeted DNA sequences over 106-fold through cycles of primer annealing and nucleotide extension of the target
sequences by DNA polymerase at specific temperatures and can provide faster and more accurate results than AFB smears and cultures within a day12. However, these procedures are often labor-intensive with multiple steps involving user manipulations with the potential for error and sample contamination13,14. Therefore, for more convenient and sensitive testing, real-time PCR techniques, involving fluorescent dyes or fluorophores with a spectrofluorometric thermal cycler, have eliminated the limitations of the techniques and have advantages such as high sensitively and faster processing time than conventional PCR15. Recently, the real- time PCR-based GeneXpert MTB/RIF test (Cepheid, Sunnyvale, CA, USA) has been widely used to detect MTB16.
3. Urine for diagnosis of TB
However, producing a sputum sample is not always possible, even in pulmonary tuberculosis (PTB) cases. Children, women, and older and severely ill patients cannot easily produce sputum. Furthermore, alternative samples have to be used for extrapulmonary TB (EPTB), such as tissue biopsies, gastric aspirates, stool, or urine. Therefore, to reduce the reliance on sputum, non-sputum-based tests have been identified as an urgent unmet clinical need. From that point of view, a urine sample is a very attractive option because urine is simple to collect without the need for invasive sampling and hazardous bioaerosols and safe to handle. Two methods of detecting MTB in urine specimens have been studied. The first detects mycobacterial lipoarabinomannan (LAM) cell wall antigen and the second detects trans-renal DNA (Tr-DNA) in the urine. There are already commercialized kits for detecting LAM. However, while these kits are useful in HIV-positive patients with advanced immunosuppression, they lack diagnostic usefulness in unselected TB suspects. Therefore, we planned to develop a new kit for detecting Tr-DNA in TB patients. Studies of Tr-DNA from MTB bacilli in the lungs, i.e., cell-free DNA fragments that have crossed the kidney barrier and are found in the urine, began relatively recently17,18. Green and colleagues reported that Tr-DNA provided a
challenging new target for molecular TB diagnosis from an accessible and abundant sample18. These Tr-DNA fragments are usually < 200bp17,19. A meta- analysis study reported that the pooled sensitivity and specificity was 0.5 (95% CI:
0.36 – 0.72) and 0.94 (95% CI 0.78 – 0.99), respectively, for a combination of PTB and EPTB specimens20. In most studies, a single real-time PCR with insertion sequences of IS6110, rpoB, or cfp32/hf6 as gene targets was used for the NAATs20. In this study, we developed a new highly sensitive NAAT combining nested PCR and real-time PCR for the detection MTB, which targeted two sequence insertions, the IS6110 sequence and the rpoB gene of MTB, and consisted of two sequential reactions in a single, closed tube. Duplex, one-tube nested, real-time PCR was designed to have two sequential reactions with two sets of primers and dual probes for the insertion sequences of the IS6110 and rpoB genes.
Methods
1. Subjects and specimens
The study was approved by the Institutional Ethics Committee of Yonsei University Severance Hospital (approval number 4-2010-0527) and Yonsei University Wonju Campus (approval number 2012-3) and all participants provided written informed consent.
From November 2010 to March 2012, a prospective clinical study was undertaken at Yonsei University Severance Hospital (a tertiary referral hospital), Seoul, the Republic of Korea. Sputum specimens were provided from 26 subjects with active TB and from 108 healthy subjects. Urine specimens were provided from 45 subjects with active TB and 30 healthy subjects.
Subjects with MTB culture-positive respiratory specimens were considered the confirmed, active PTB group. Individuals with human immunodeficiency virus (HIV) infection, end-stage renal disease, or leukemia/ lymphoma, and those who had received anti-TB therapy for more than two weeks or immunosuppressive therapy, including anti-cancer chemotherapy for malignant disease, within three months of enrollment, were excluded from the study. The healthy control group consisted of healthy adults with both a negative tuberculin skin test (TST) and a QuantiFERON-TB ○R Gold In-Tube (QFT-IT) test, who were free of TB symptoms and did not have any contact with active PTB patients.
The procedure of specimen treatment and mycobacterial culture procedure were conducted according to theCLSI21guidelines and the Korean Guidelines for the Laboratory Diagnosis of TB22. Sputum specimens were liquefied using an equal volume of N-acetyl- L-cysteine and decontaminated using an
equal volume of 4% sodium hydroxide (NaOH). After decontamination, the specimens were neutralized with sterile phosphate buffer saline (PBS, pH 6.8) and centrifuged at 3000 × g for 20 min. After pouring off the supernatant, the sediment was suspended in sterile saline and used for smear preparation, inoculation into Löwenstein-Jensen (LJ) media, and DNA extraction.
Smears were prepared using the suspended sediment and stained using the Ziehl-Neelsen method. The presence of AFB was examined using a light microscope, and the results of the AFB smear were graded according to the American Thoracic Society/Center for Disease Control and Prevention23 as follows: grade 0, no bacilli in 300 fields; trace, 1 or 2 bacilli in 300 fields; grade 1, 1–9 bacilli in 100 fields; grade 2, 1–9 bacilli in 10 fields; grade 3, 1–9 bacilli in one field, and grade 4, >9 bacilliin one field. The smears were recorded as positive from grade 1 according to the guidelines. Mycobacterial cultureswere performed using LJ media with the suspended sediment and checked every week for eight weeks24.
Urine was stored at -70℃ immediately after collection and thawed at room temperature for use. One ml of urine sample was dispensed into microcentrifuge tubes and centrifuged at 15,000 g for 10 min at 4 ℃. The supernatant was removed and the pellet resuspended in 1 ml of PBS at pH 7.4. After vortexing strongly, the supernatant was discarded after centrifuging at 15,000 g for 10 min at 4 ℃. The same process was repeated twice and washed. Then, 50 ul of 5% chelex resin (Optipharm, Chungju, Korea) was added to the pellet and vortexed for 1 min. DNA was isolated from the urine sediment with a slight modification of the method previously described25. The urine pellets were boiled for 20 min. Cell debris was sedimented by centrifugation for 10 min at15,000 g and the supernatant was used for PCR amplification.
2. DNA extraction
DNA extraction was performed as described previously26. Briefly, 200 μL of distilled water was added to the bacterial pellets and collected mycobacterial colonies. The suspended bacterial pellets, mycobacterial colonies, and sputum sediment were boiled for 10 min. Cell debris was sedimented by centrifugation for 2 min at 10,000 × g, and the supernatant was used for PCR amplification. The DNA concentration was measured using a NanoDrop NT-1000 spectrophotometer (Thermo Scientific, Wilmington, DE, USA).DNA was stored at -20°C prior to using.
3. Minimum limit of detection, sensitivity, and specificity of real-time PCR assays
The real-time PCR assays were performed and validated according to the27 guidelines. The real-time PCR assays were performed three times using a series of MTB H37Rv DNA samples to measure the minimum limit of detection, which was determined as thefinal concentration of MTB DNA for which the cycle threshold (Ct) reached the cutoff, as calculated by the Applied Biosystems 7500 Fast real-time PCR system. A standard curve was generated by plotting the Ct values against the log of the starting quantity of template for each dilution, and the coefficient of determination (R2) was calculated based on the standard curve.
4. Single real-time PCR
The rpoB gene and the IS6110 gene were used as specific targets for MTB and each gene was subjected to single real-time PCR in the following process. For the amplification of genomic DNA (gDNA) from the samples, real-time PCR was carried out with 10 μL of 2x THUNDERBIRD Probe qPCR Mix (Toyobo, Tokyo, Japan), using 5 μL of gDNA as the template, and 5 μL
of 10 μM sense primers, antisense primers, and probes in a total volume of 20 μL. The sequences of the primers and probes are shown in Table 1.
The thermocycling and detecting conditions were 10 min at 95 ℃, followed by 40 cycles of 15 sec at 95 ℃, and 30 sec at 60 ℃. All reactions were performed using a CFX-96 real-time PCR detection system (Bio-Rad Laboratories, Hercules, CA, USA). The real-time PCR detection system was used to the measure the fluorescence formed during the PCR process. For comparison under conditions such as one-tube nested real-time PCR, 20 μM primers were added to the forward primer and reverse primers. The thermocycling and detecting conditions were 10 min at 95 ℃, followed by 40 cycles of 15 sec at 95 ℃, and 30 sec at 60 ℃. A real-time PCR detection system was used to the measure the fluorescence formed during the PCR process. A CFX-96 real-time PCR detection system (Bio-Rad Laboratories, Hercules, CA, USA) was used according to the manufacturer’s instructions.
5. One-tube nested real-time PCR
One-tube nested real-time PCR was performed by selecting specific sequences for MTB from the rpoB and IS6110 genes, and one-tube nested real-time PCR was performed using the rpoB and IS6110 genes simultaneously to improve specificity and sensitivity. For amplification of gDNA from the samples, real-time PCR was carried out with 10 μL of 2x THUNDERBIRD Probe qPCR Mix (Toyobo, Tokyo, Japan) using 5 μL of gDNA as the template; 2.5, 5, and 10 μM 1st sense primers, antisense primers; 10 μM 2nd sense primers and antisense primers and 10 μM probes in a total volume of 25 μL. The sequences of the primers and probes are shown in Table 1. The cycling conditions included an initial denaturation at 95 °C for 10 min, followed by the first amplification stage with 10 cycles of denaturation at 95 °C for 15 sec, annealing/extension at 65 °C for 30 sec;
and a second amplification stage with 40 cycles of denaturation at 95 °C
for 15 sec, annealing/extension at 60 °C for 30 sec. Fluorescent signal acquisition was conducted at the end of every cycle during the second amplification stage.
Target Objective Name 5’
modification
Sequence 3’
modification rpoB
gene 1st primer
Sense-rpoB GCG TCG GTC GCT ATA AGG TCA AC Antisense-rpoB ACC CTC GTG CAA GCG GAC CAG ATA T 2nd
primer
Sense-rpoB GGT CGC TAT AAG GTC AAC AAG AAG Antisense-rpoB ACC CTC GTG CAA GCG GAC CAG
rpoBprobe FAM CTG CAT GTC GGC GAG CCC ATC ACG BHQ1 IS6110 1st
primer
Sense-IS6110 AAC GGC TGA TGA CCA AAC TC Antisense-
IS6110
AAG CGG CGC TGG ACG AGA TC
2nd primer
Sense-IS6110 GTC GAA CGG CTG ATG ACC AAA CT Antisense-
IS6110
TCC GAA GCG GCG CTG GAC GA
IS6110 probe-1 FAM ACC CGC GGC AAA GCC CGC AGG BHQ1 IS6110 probe-2 FAM ACC ACG ATC GCT GAT CCG GCC ACA BHQ1
Table 1. Primers and probes used in this study.
Results
1. Sensitivity of single rpoB real-time PCR and one-tube nested rpoB real- time PCR
Single real-time PCR and one-tube nested real-time PCR were optimized using the genomic DNA of MTB H37Rv. Real-time PCR assays were optimized in the Applied Biosystems 7500 FAST Real-time PCR System (Applied Biosystems) using several concentrations of primers and probes.
The analytical sensitivity of the assays was determined through the use of 10-fold dilutions [10 ng, 1 ng, 100 pg, 10 pg, 1 pg, 100 fg, 10 fg (1bacilli)]
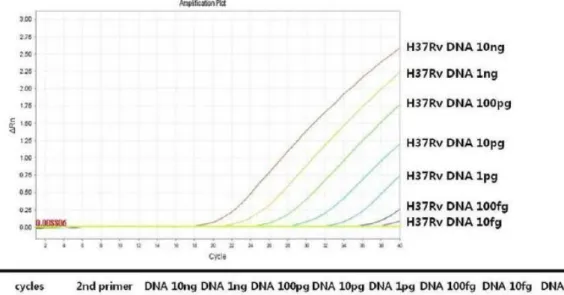
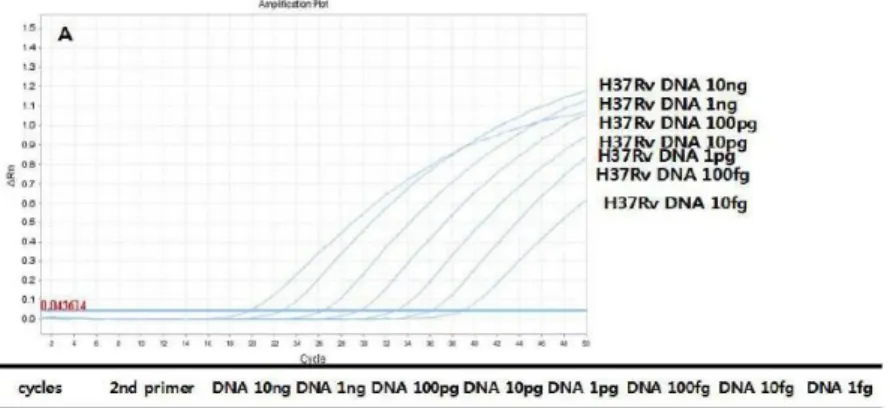
in a standard curve of DNA isolated from the MTB H37Rv strain. The Ct values for the MTB H37Rv by single rpoBreal-time PCR assays ranged from 17.36 to 37.18 with 10pM of primers (Figure 1). In comparison, the Ct values for the MTB H37Rv by one-tube nested rpoB real-time PCR ranged from 10.33 to 27.92 (Figure 2). The results showed that one-tube nested rpoB real-time PCR was 100 times more sensitive than single rpoBreal-time PCR.
Figure 1. Amplification curves of rpoB single real-time PCR.
Figure 2. Amplification curves of rpoB one-tube nested real-time PCR
2. Sensitivity of the rpoB single real-time PCR
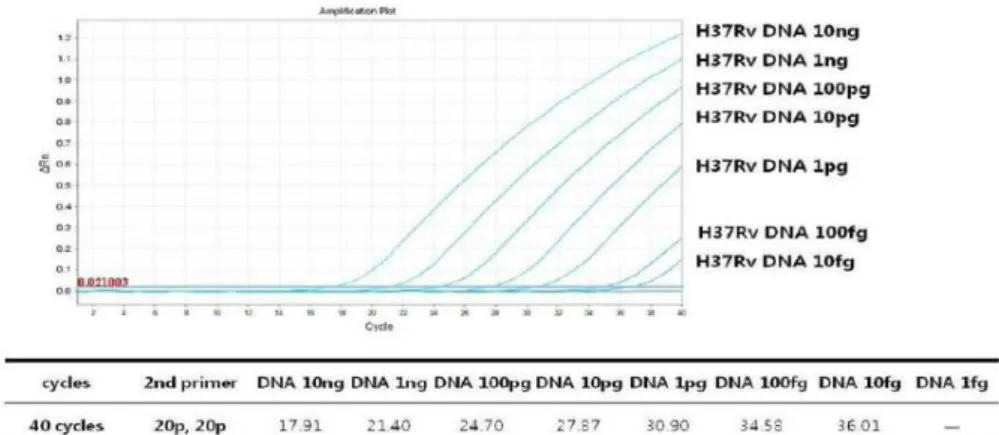
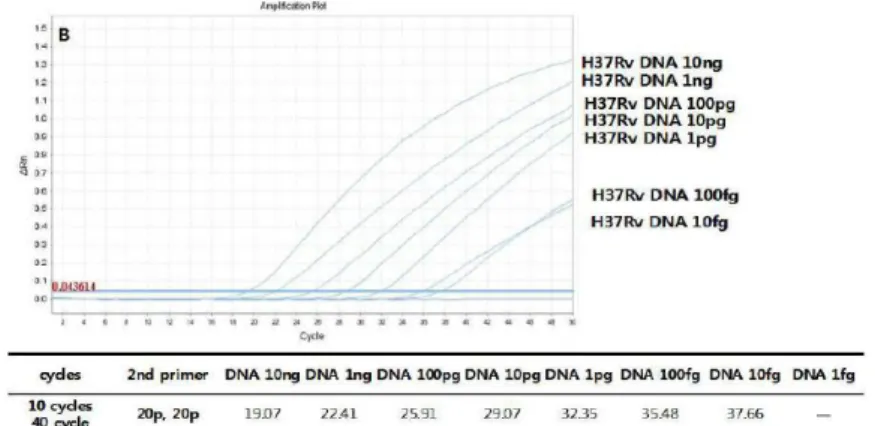
We needed to confirm whether the sensitivity improvement over single rpoB real-time PCR was the effect of the primer concentrations and cycle numbers used. The sensitivity of both assays was verified by using 10 pM and 20 pM concentrations of the 2nd primer (Figure 3), and 40 cycles and 50 cycles (Figure 4a, 4b). As a result, the sensitivity did not increase when using 2nd primer concentrations from 10 pM to 20 pM, and the sensitivity of each concentration decreased when 50 cycles were performed, which is the same cycle number as that used in one-tube nested real-time PCR.
Figure 3. Amplification curves of rpoB single real-time PCR with doubling primer concentrations.
Figure 4a. Amplification curves of rpoBsingle real-time PCR with increasing cycles.
Figure 4b. Amplification curves of rpoB single real-time PCR with doubling primer concentrations and increasing cycles.
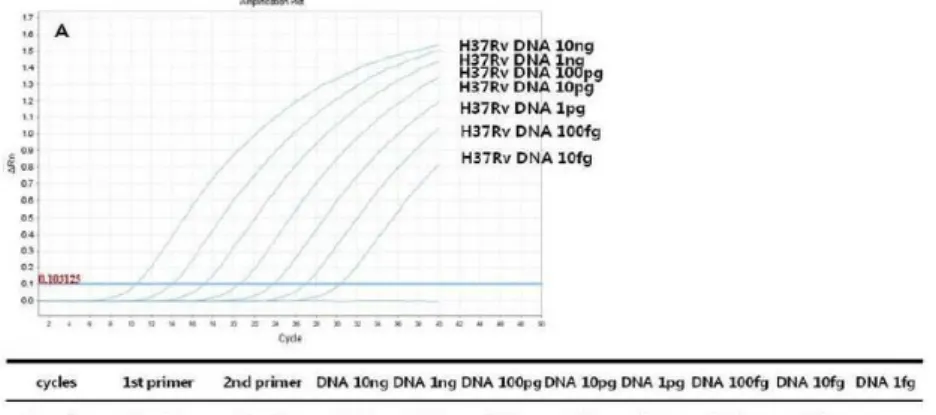
3. Sensitivity of the one-tube nested rpoB real-time PCR
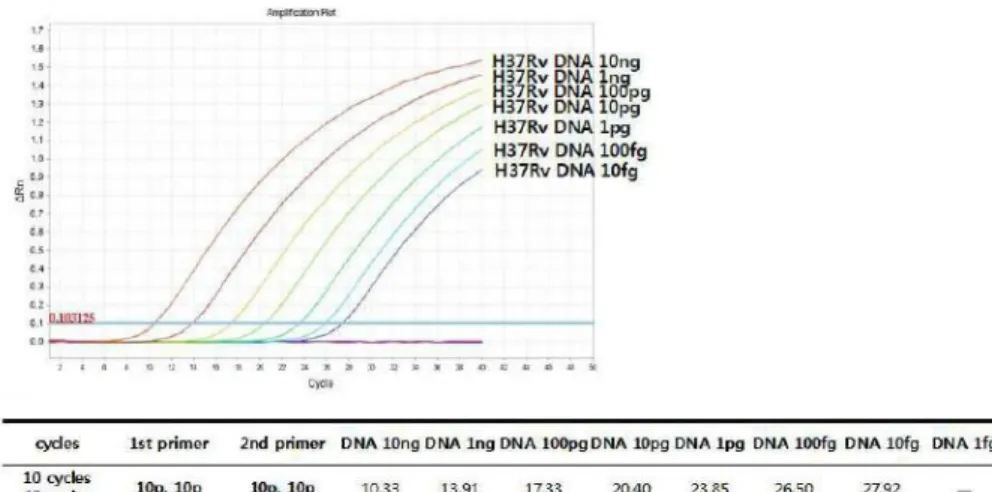
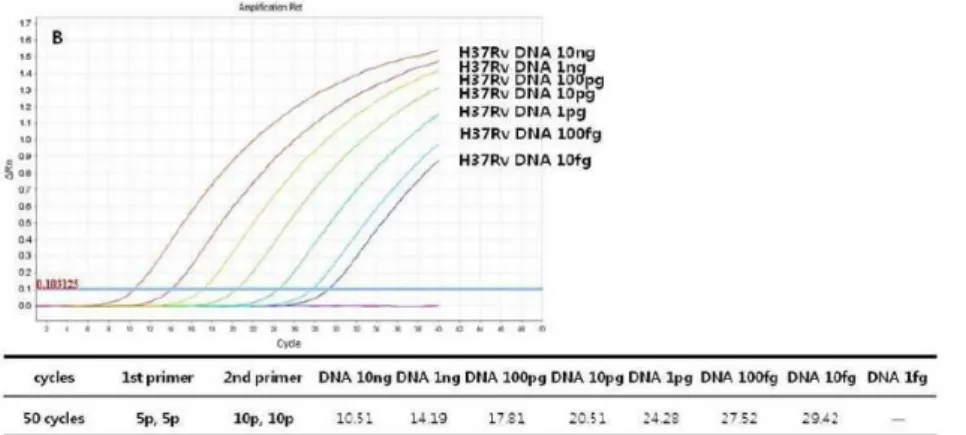
We needed to check the change in sensitivity by adjusting the primer concentrations. The concentrations of 1st primer were 2.5 pM (Figure 5a), 5 pM (Figure 5b), and 10 pM (Figure 5c), and the concentration of 2nd primer was 10 pM. When the sensitivity was checked according to primer concentration, the Ct value was 30.48 at 2.5 pM concentration, and 29.42 at 5 pM concentration, and 27.42 at 10 pM concentration in 100fg concentration. Sensitivity differences in 10-fold primer concentrations were confirmed. Based on these results, we found that sensitivity was at least 100 times higher when performing one-tube nested real-time PCR using a
10 pM concentration of 1stprimer and a 10 pM concentration of 2nd primer (Table 2).
Figure 5a. Amplification curves of rpoBone-tube nested real-time PCR with decreasing concentrations of the 1st primers (2.5 pM, 2.5 pM)
Figure 5b. Amplification curves of rpoB one-tube nested real-time PCR with decreasing concentrations of the 1st primers (5 pM, 5 pM)
Figure 5c. Amplification curves of rpoB one-tube nested real-time PCR (10 pM, 10 Pm)
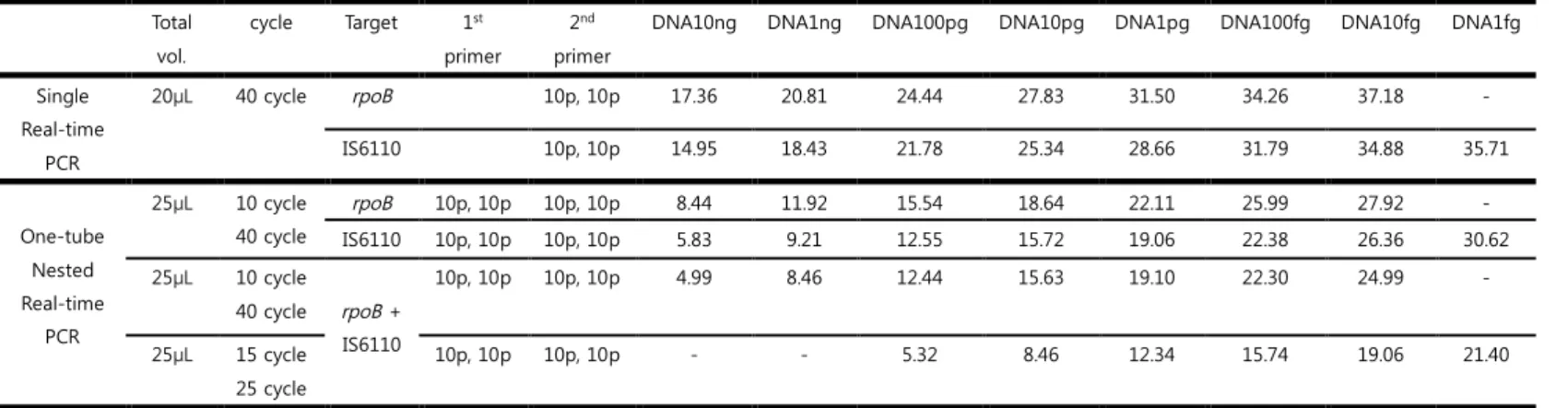
Table 2. Limits of detection of single real-time PCR assays and one-tube nested real-time PCR for the dilution series of MTB H37Rv DNA
Total vol.
cycle Target 1st primer
2nd primer
DNA10ng DNA1ng DNA100pg DNA10pg DNA1pg DNA100fg DNA10fg DNA1fg
Single Real-time
PCR
20μL 40 cycle rpoB 10p, 10p 17.36 20.81 24.44 27.83 31.50 34.26 37.18 -
IS6110 10p, 10p 14.95 18.43 21.78 25.34 28.66 31.79 34.88 35.71
One-tube Nested Real-time
PCR
25μL 10 cycle 40 cycle
rpoB 10p, 10p 10p, 10p 8.44 11.92 15.54 18.64 22.11 25.99 27.92 -
IS6110 10p, 10p 10p, 10p 5.83 9.21 12.55 15.72 19.06 22.38 26.36 30.62
25μL 10 cycle
40 cycle rpoB + IS6110
10p, 10p 10p, 10p 4.99 8.46 12.44 15.63 19.10 22.30 24.99 -
25μL 15 cycle 25 cycle
10p, 10p 10p, 10p - - 5.32 8.46 12.34 15.74 19.06 21.40
Table 3. Limits of detection of single real-time PCR assays and duplex, one-tube nested, real-time PCR for the dilution series of MTB H37Rv DNA
Total vol. cycle 1stprimer 2ndprimer DNA10ng DNA1ng DNA100pg DNA10pg DNA1pg DNA100fg DNA10fg DNA1fg Single
Real-time PCR
20μL
40 cycle 10p, 10p 17.36 20.81 24.44 27.83 31.50 34.26 37.18
20p, 20p 17.91 21.40 24.70 27.87 30.90 34.58 36.01
50 cycle 10p, 10p 19.52 22.90 26.53 29.71 33.25 26.48 38.13
20p, 20p 19.07 22.41 25.91 29.07 32.48 35.48 27.66
One-tube Nested Real-time
PCR
20μL 10 cycle 40 cycle
10p, 10p 10p, 10p 10.33 13.91 17.33 20.40 23.85 26.50 27.92
5p, 5p 10p, 10p 10.51 14.19 17.81 20.51 24.28 27.52 29.42
2.5p,2.5p 10p, 10p 10.45 13.86 17.18 20.57 23.92 26.75 30.48
4. Sensitivity of the single IS6110 real-time PCR and one-tube nested IS6110 real-time PCR
The Ct values for the MTB H37Rv by single IS6110 gene real-time PCR assays ranged from 14.95 to 35.71 with 10 pM of primer (Figure 6). In comparison, the Ct values for the MTB H37Rv by one-tube nested IS6110 real-time PCR ranged from 5.83 to 30.62 (Figure 7). Therefore, the one- tube nested real-time PCR was 100 times more sensitive than the single real-time PCR.
Figure 6. Amplification curves of single IS6110 real-time PCR
Figure 7. Amplification curves of one-tube nested IS6110 real-time PCR
5. Sensitivity of the rpoB and IS6110 duplex, one-tube nested, real-time PCR To improve the sensitivity of the one-tube nested real-time PCR, the rpoB
one-tube nested real-time PCR was performed by adding the IS6110 gene.
The Ct values for the MTB H37Rv by single rpoB real-time PCR assays ranged from 4.99 to 24.9 with 10 pM of primer (Figure 8). In addition, to further increase sensitivity, we performed 15 and 25 cycles instead of 10 and 40 cycles where 10 and 40 cycles could detect 10 fg/㎕ of MTB DNA as positive. However, 15 and 25 cycles could detect 1 fg/㎕ of MTB DNA as positive, respectively (Figure 9). Based on these results, we found that sensitivity was at least 100 times higher when performing duplex, one-tube nested, real-time PCR using 10 pM concentrations of the 1st primer and 10 pM concentrations of the 2nd primer with 15 and 25 cycles (Table 3).
Figure 8. Amplification curves of rpoB and IS6110 duplex, one-tube nested, real-time PCR
Figure 9. Amplification curves of rpoB and IS6110 duplex, one-tube nested, real-time PCR with modified cycles
6. Sensitivity and specificity of the real-time PCR
Clinical specimens were used to identify the sensitivity and specificity of the newly developed duplex, one-tube nested, real-time PCR. The specificity was checked by collecting sputum and urine from healthy controls, and the sensitivity was checked by using samples of patients with confirmed to have AFB culture-positive PTB.
6-1. Sputum specimens
The sensitivity of the newly developed duplex, one-tube nested, real-time PCR was compared to a commercial single real-time PCR, Real MTB-ID (M&D, Korea) test to determine the detection rate of MTB in the clinical sputum specimens. The specificity and specificity of the Real MTB-ID test were 100% and 46.2% (12/26), respectively, while those of the duplex, one- tube nested, real-time PCR were 100% and 100% (26/26), respectively (Table 4).
Healthy controls (n=108)
Pulmonary Tuberculosis patients (n=26)
AFB stain - Negative
(n=2)
Trace (n=2)
1+
(n=2)
2+
(n=7)
3+
(n=4)
4+
(n=9)
total
AFB culture - 2 2 2 7 4 9 26
Single PCR (%) - 0 (0) 1 (50) 0 (0) 6 (85) 1 (25) 4 (44) 12 (46.2)
One-tube nested PCR (%)
- 2 (100) 2 (100) 2 (100) 7 (100) 4 (100) 9 (100) 26 (100)
Table 4. The sensitivity and specificity for sputum specimens 6-2. Urine specimens
The sensitivity of the newly developed duplex, one-tube nested, real-time PCR was compared to a commercial single real-time PCR assay, the AdvanSure MTB/NTM real-time PCR (LG Life Sciences Ltd., Korea) test, to determine the detection rate of MTB in clinical urine specimens. The specificity and sensitivity of the AdvanSure MTB/NTM real-time PCR test were 100% and 6.7% (3/45), respectively, while those of the duplex, one- tube nested, real-time PCR were 100% and 51.1% (23/45), respectively (Table 5).
Table 5. The sensitivity and specificity for urine specimens Healthy controls
(n=30)
Pulmonary Tuberculosis patients (n=45)
AFB stain - Negative
(n=11)
Positive (n=34)
total
AFB culture - 11 34 45
Single PCR (%) - 1 (9) 2 (5.8) 3 (6.7)
One-tube nested PCR (%)
- 4 (36.3) 19 (55) 23 (51.1)
Discussion
In this study, we developed a highly sensitive PCR assay, duplex, one-tube nested, real-time PCR assay targeting the IS6110 and rpoBsequences of MTB for detecting MTB, taking advantage of nested PCR and real-time PCR. Duplex, one-tube nested, real-time PCR is a rapid, simple, and sensitive method, which can sensitively detect MTB by sequential amplification of the IS6110 and rpoB sequences of MTB in a single, closed tube. The duplex, one-tube nested, real-time PCR was approximately 100 times more sensitive than single, one-tube nested, real-time PCR. The detection limit of the duplex, one-tube nested, real-time PCR was 1 fg/㎕ of MTB DNA, which is supposed to be the lowest limit of nucleic acid detection.
Furthermore, the sensitivity of the duplex, one-tube nested, real-time PCR was 51.1%
(23/45) for urine specimens. Therefore, this study serves as a preliminary investigation for future research and assay development using Tr-DNA.
The IS6110 sequence of MTB is a conventional target for detecting MTB due to its multiple copies in the genome and specificity for MTB. However, the IS6110 copy number in MTB varies28. Choi et al. demonstrated the ability to detect MTB Tr-DNA by IS6110 single, one-tube nested, real-time PCR of sputum specimens from persons with sputum culture-positive TB disease in a previous study29. Thereafter, we hypothesized that the combination of another MTB gene with the IS6110 sequence as targets might increase the MTB detection sensitivity of the assay. Our hypothesis is supported by the results that the IS6110 and rpoBduplex, one-tube nested, real-time PCR assay was approximately 100 times more sensitive than the single IS6110, one-tube nested, real-time PCR. To the best of our knowledge, this is the first study in which MTB was diagnosed in urine specimens using a duplex, one-tube nested, real-time PCR method.
The type of specimen is one of the most important determinants in TB diagnosis.
Sputum is widely used as the testing specimen but is limited by its complexity, heterogeneity, and infectious potential during sample collection. Also, sputum
production is often difficult in patients with HIV infections, those severely ill, and in children. Furthermore, sputum has limited usefulness in diagnosing EPTB.
Therefore, many studies have investigated the use of biological specimens other than sputum, such as blood, urine, and exhaled breath to diagnose TB. Of these, urine is the most attractive specimen type, because of its availability; ease of access, processing, and storage; and the low infection risk to healthcare workers during sample collection30. There are two methods to detect MTB in urine specimens. The first is to detect LAM cell wall antigen in urine. One commercially available point- of-care test (Alere Determine TB LAM Ag [AlereLAM]) had suboptimal sensitivity in an unselected population. Recently the novel Fujifilm SILVAMP TB-LAM (FujiLAM) test demonstrated sensitivity superior to the AlereLAM assay31. However, urine LAM appears promising as a diagnostic tool only in HIV-positive patients with CD4 cell counts less than 200 cells/㎕ in different clinical settings. Furthermore, while urine LAM has been used as an enhanced diagnostic tool, Tr-DNA has the potential for strain-specific identification or a more persistent biomarker during the treatment of active TB disease. Therefore, the second methods has been actively studied, which is the detection of Tr-DNA using PCR assays. In the early studies, PCR tests were used successfully to detect MTB in urine sample of patients with genitourinary TB, where the infectious bacteria are present in the urinary tract32. Thereafter, attempts were made to detect MTB DNA in the urine of patients with PTB and EPTB other than genitourinary TB. There is increasing evidences that urine contains DNA fragments derived from the cell-free nucleic acids in the blood caused by the breakdown of nucleic acid released from dying human cells and microorganisms.
The use of PCR-based methods to detect MTB in urine has already been reported previously with varying yield. However, the problem with urine TB-PCR was that there was a high degree of variability in the consistency and sensitivity. A meta- analysis of Tr-DNA based studies found that the sensitivity varied from 3.8% to 79% for a combination of PTB and EPTB samples. This was probably due to a lack of reliable and standardized nucleic acid isolation and PCR methods, resulting in a
huge variance in the results. In fact, meta-regression conducted in the meta- analysis study found that the lower urine storage temperatures (sensitivity 0.71 vs.
0.35 for temperatures < -70 ℃ vs ≥ - 70 ℃, P = 0.05); slower centrifuge speeds (sensitivity 0.61 vs. 0.19 for < 5000 revolutions per minute [rpm] vs. ≥ 5000 rpm, P = 0.05); and the IS6110 target gene (sensitivity 0.70 vs. 0.33 for IS6110 vs. rpoB, P = 0.08) increased the sensitivity. Covariates, such as urine volume or fraction, storage duration, and additives were not mentioned or were too heterogenetic to analyze. Therefore, standardized testing methods and reproducibility are prerequisites for the implementation of PCR methods.
In general, the sensitivity of the MTB PCR for paucibacillary sputum specimens is known to be lower than that of the AFB smear-positive specimens. Previous reports revealed that the sensitivity and specificity of the sputum PCR reached 95% in smear-positive specimens, whereas the values for 40 to 77% of the smear-negative cases were more than 95%33-36. Moreover, Choi reported that the sensitivity of the one-tube nested real-time PCR for smear-negative or trace specimen was 100% in sputum specimens28. However, there are not many studies on the sensitivity of urine MTB PCR assays in patients with paucibacillary sputum. In our study, the sensitivity of the sputum duplex, one-tube nested, real-time PCR for AFB smear- negative or trace sputum specimens was 100% (4/4), and the sensitivity of the urine duplex, one-tube nested, real-time PCR test for patients with AFB smear- negative results was 36.3% (4/11). These results were consistent with those of studies indicating that the urine PCR-based molecular assay showed sensitivity varying from 38% to 66.7% in paucibacillary specimens37,38. Peter et al. reported that the sensitivity of urine Xpert MTB/RIF was 38% in HIV-negative patients with sputum AFB smear-negative results and 40% in HIV-positive patients with sputum scarce AFB results38. However, most studies have been done on HIV-positive patients. Although our findings are preliminary and were obtained on a small number of individuals, this preliminary study indicated that duplex, one-tube
nested, real-time PCR may potentially aid the diagnosis of TB in HIV-negative patients when a sputum-based diagnosis is not possible.
Up to 25% of the TB cases present with extrapulmonary involvement and EPTB can constitute up to 50% of the TB cases in HIV-positive patients 39,40. Although the total number of TB patients has decreased, a decrease in the number of EPTB patients has been slower. Therefore, the proportion of EPTB is growing compared to PTB. The problem with EPTB is the difficulty in establishing a definitive diagnosis.
The diagnosis of EPTB can be challenging, owing to the paucibacillary nature of the specimens. A negative AFB smear, lack of granulomas on biopsy histopathology examination, and failure to culture MTB cannot exclude a diagnosis of EPTB. A major breakthrough in the diagnosis of EPTB was achieved by the development of NAAT using direct extrapulmonary specimens. However, there is a high variation in sensitivity. In extrapulmonary TB such as pleural, meningeal, urinary, peritoneal, and pericardial TB, the sensitivity of direct specimen PCR ranged between 2.8%
and 100%, with a relatively high specificity of between 57% and 100%40. The diagnosis is strongly influenced by different extrapulmonary specimen types from atypical presentations and low bacterial loads. Therefore, recent research has focused on new diagnostic tools that could indirectly detect MTB regardless of the location of the lesions and also detect biomarkers in non-invasive samples.
However, few studies using urine PCR for EPTB have been reported and many questions remain concerning the desirability of these assays. Previous reports revealed that the sensitivity of urine PCR in EPTB patients varied from 27% to 70%
37, 41-43. Fortun et al. reported that 16s-rRNA amplification in urine was positive in 70% of the patients with EPTB compared to only 18% of the PTB patients41. Excluding the genitourinary form, 16s-rRNA in urine had a sensitivity of 72%, 67%, and 90% in lymphadenitis, multifocal forms, and miliary TB, respectively. Cruz et al.
showed similar results, that the sensitivity of IS6110 nested PCR for MTB in patients with EPTB was 47.8% and 52% in blood and urine, respectively, compared to 20%
and 26.9%, respectively, in PTB patients42. In our study, it was not possible to
investigate the sensitivity of our duplex, one-tube nested, real-time PCR in EPTB patients. Based on these studies, there is a possibility that the duplex, one-tube nested, real-time PCR assay will increase the sensitivity of detection in EPTB patients. Further study is needed in EPTB patients.
In immunosuppressed HIV-positive patients, the frequency of EPTB and miliary TB is increased, sputum smear microscopy performance is reduced, and up to one- third of the patients cannot produce sputum for a diagnostic sample. Therefore, the diagnosis of TB in HIV-positive patients is challenging and often delayed38. As a result, many studies have focused on urine samples to diagnose TB in HIV- positive patients. For patients with a CD4 T-cell count of fewer than 50 cells per
㎕, the sensitivity of the urine LAM test ranged from 56% to 85%, with a specificity of > 88%44,45. Therefore, the World health Organization (WHO) recommended that a urine AlereLAM test is used for HIV-positive patients with CD4 T-cell counts equal to or less than 10046. Some studies have reported that the LAM test is also useful in HIV-negative patients47, but the data are limited due to the lack of studies.
However, few studies have compared urine PCR to diagnose TB in HIV-positive and HIV-negative patients. As the LAM results showed, urine PCRs tests are also expected to be more sensitive in detecting MTB in HIV-positive patients than in HIV-negative patients. Therefore most studies on the urine PCR have focused on patients co-infected with TB and HIV. Kafwabulula et al. reported that the sensitivity of the urine PCR was lower in HIV-negative patients than in HIV-positive patients (64% vs. 23%; P = 0.05)25. Torrea et al. also reported that MTB was detected significantly more frequently in HIV-positive versus HIV-negative patients with microbiological positive PTB (52.4% vs. 30.5%, P = 0.001) and in patients with EPTB (67.4% vs. 46.3%, P = 0.05)37. However, in another study, there was no difference between HIV-positive and HIV-negative patients (45.2% vs. 40.0%)48. In our study, the sensitivity of urine PCR was relatively high at 55% with in all HIV-negative patients. A further larger cohort study is needed to compare both groups.
In a recent study, Labugger et al. reported that they developed a new molecular assay based on Tr-DNA and tested it for the diagnosis of PTB at the initiation of anti-TB therapy and specifically, during treatment follow-up49. In this study, they analyzed the correlation between Tr-DNA and the time to positivity in cultures or AFB microscopy scores at the onset of treatment, and no correlation was observed.
Kinetics in treatment-naïve patients showed low base-line Tr-DNA levels, which increased to maximal Tr-DNA levels within one week, and maximal Tr-DNA levels were correlated positively with a radiological score. This study suggested that their assay could be a method to assess treatment responses. Further study of our duplex, one-tube nested, real-time PCR is needed to determine if it could be used in TB treatment monitoring.
In summary, the urine duplex, one-tube nested, real-time PCR test cannot be used alone for TB screening but there is a possibility it could be used in conjunction with AFB smears and cultures. The urine duplex, one-tube nested, real-time PCR could be particularly useful in determining whether to start TB treatment without waiting for the AFB culture results in patients with suspected TB but AFB smear- negative results.
Detecting circulating Tr-DNA in urine has great potential for diagnosing MTB infection, but this study had several limitations. First, this study was a preliminary study. Therefore, the sample size was very small. Second, altering the preparation methods of DNA from urine may have the potential to improve the sensitivity of this assay. In this study, urine samples were stored at -70 ℃, and centrifuged at 15,000× g. Different urine storage temperatures, slower centrifuge speeds, and separate analysis of the supernatants and sediments could increase the sensitivity17,20. Third, in this study, there were no HIV-positive patients or EPTB patients.
Our results are the basis for further prospective studies in which larger groups of patients will be analyzed, including HIV-positive patients, smear-negative PTB
patients, and EPTB patients. Future studies will examine quantitative analysis by the duplex, one-tube nested, real-time PCR method to provide an analytical test for monitoring treatment.
Conclusion
In conclusion, a new, efficient, highly sensitive, duplex, one-tube nested, real-time PCR assay, targeting the IS6110 and rpoBsequences, was developed for detecting MTB in urine specimens. If the results presented here are confirmed in future studies, the application of the duplex, one-tube nested, real-time PCR could increase the yield of TB diagnoses in HIV-negative subjects as well as in HIV- positive subjects.
References
1. WHO. Global tuberculosis control: surveillance, planning, financing: WHO
report 2019. World Health Organization; Geneva (2019).
2. Korea Centers for Disease Control and Prevention. Annual Report on the
Notified Tuberculosis in Korea 2019. Cheongju: Korea Centers for Disease
Control and Prevention; (2019).
3. Cho KS. Tuberculosis control in the Republic of Korea. Epidemiol Health
2018;40:e2018036.
4. Alavi SM, Bakhtiyariniya P, Albagi A: Factors associated with delay in diagnosis
and treatment of pulmonary tuberculosis. Jundishapur J Microbiol, 8:e19238
(2015).
5. Virenfeldt J, Rudolf F, Camara C, Furtado A, Gomes V, Aaby P, Petersen E, Wejse
C: Treatment delay affects clinical severity of tuberculosis: a longitudinal cohort
study. BMJ Open 4:e004818 (2014).
6. Bates JH. Diagnosis of tuberculosis. Chest. 76: 757-763 (1979).
7. Maurya AK, Nag VL, Kant S, Jushwaha RA, Kumar M, Mishra V, Rhaman W,
Dhole TN. Evaluation of an immunochromatographic test for discrimination
between Mycobacterium tuberculosis complex & non tuberculous
mycobacteria in clinical isolates from extra-pulmonary tuberculosis. Indian J.
Med. Res. 135, 910-906 (2012).
8. Centers for Disease Control and Prevention (CDC). National Institute of Health.
Biosafety in Microbiological and Biomedical Laboratories. 5th edition. HHS
Publication Noa. (CDC) 21-1112. Washington: US government Printing Office.
438p (2009).
9. Hepple P, Ford N, McNerney R. Microscopy compared to culture for the
diagnosis of tuberculosis in induced sputum samples: a systematic review. Int
J Tuberc Lung Dis. 16, 579-88 (2012).
10. Beavis KG, Lichty MB, Jungkind DL, Giger O. Evaluation of Ampicor PCR for
direct detection of Mycobacterium tuberculosis from sputum specimens. J Clin
Microbiol. 33, 2582-2586 (1995).
11. Woods GL, Molecular techniques in mycobacterial detection. Arch Pathol Lab
Med 125, 122-126 (2001).
12. Saiki RK, ,Gelfand DH, Stoffel S, Scharf SJ, Higuchi R, Horn GT, Mullis KB, Erich
HA. Primer-directed enzymatic amplification of DNA with a thermostable DNA
polymerase. Science. 239, 487-491 (1988).
13. Kitchin PA, Szotyori Z, Fromholc C, Almond N. Avoidance of PCR false positives.
Nature. 344, 201 (1990).
14. Levidiotou S, Vrioni G, Galanakis E, Gesouli E, Pappa C, Stefanou D. Four-year
experience of use of the Cobas Amplicor system for rapid detection of Mycobacterium tuberculosis complex in respiratory and nonrespiratory
specimens in Greece. Eur J Clin Microbiol Infect Dis. 22, 349-356 (2003).
15. Kraus G, Cleary T, Miller N, Seivright R, Young AK, Spruill G, Hnatyszyn HJ. Rapid
and specific detection of the Mycobacterium tuberculosis complex using
fluorogenic probes and real-time PCR. Mol Cell Probes. 15, 375-383 (2001).
16. Boehme CC, Nabeta P, Hillemann D, Nicol MP, Shenai S, Krapp F. Rapid
molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 262,
1005-1015 (2010).
17. Cannas A, Goletti D, Girardi E, Chiacchio T, Calvo L, Cuzzi G, Piacentini M,
Melkonyan H, Umansky SR, Lauria FN, Ippolito G, Tomei LD. Mycobacterium
tuberculosis DNA detection in soluble fraction of urine from pulmonary
tuberculosis patients. Int J tuberc Lung dis. 12(2), 146-151 (2008).
18. Green C, Huggett JF, Talbot E, Mwaba P, Reither K, Zumla AI. Rapid diagnosis
of tuberculosis through the detection of mycobacterial DNA in urine by nucleic acid amplification methods. Lancet Infect. Dis. 9 (8), 505-511 (2009).
19. Botezatu I, Serdyuk O, Potapova G. Genetic analysis of DNA excreted in urine:
a new approach for detecting specific genomic DNA sequences from cells
dying in an organism. Clin Chem 46, 1078-1084 (2000).
20. Marangu D, Devine B, John-Stewart G. Diagnostic accuracy of nucleic acid
amplification tests in urine for pulmonary tuberculosis: a meta-analysis. Int J
Tuberc Lung Dis 19(11). 1339-1347 (2015).
21. Clinical and Laboratory Standards Institute (CLSI). Susceptibility Testing of
Mycobacteria, Nocardiae, and Other Aerobic Actinomycetes; Approved
Standard. NCCLS document M24-A. USA: NCCLS, Wayne; (2003).
22. Korean Guideline for Laboratory Diagnosis of Tuberculosis, 2012, Korean
Centers of Disease Control, Osong, Korea.
23. American Thoracic Society. Diagnostic standards and classification of
tuberculosis in adults and children. Am J Respir Crit Care Med ;161:1376
(2000).
24. World Health Organization (WHO). Laboratory services in tuberculosis
control, Part II: microscopy. World Health Organization; (1998).
25. Kafwabulula M, Ahmed K, Nagatake T. et al. Evaluation of PCR-based methods
for the diagnosis of tuberculosis by identification of mycobacterial DNA in urine
samples. Int J Tuberc Lung Dis 6(8):732-737 (2002).
26. Bang H, Park S, Hwang J, Jin H, Cho E, Kim DY, et al. Improved rapid molecular
diagnosis of multidrug-resistant tuberculosis using a new reverse
hybridization assay, REBA MTB-MDR. J Med Microbiol ;60:1447–54 (2011).
27. Shamputa IC, Lee J, Allix-Beguec C, Cho EJ, Lee JI, Rajan V, et al. Genetic
diversity of Mycobacterium tuberculosis isolates from a tertiary care
tuberculosis hospital in South Korea. J Clin Microbiol ;48:387–94 (2010).
28. Zakham F, Lahlou O, Akrim M, et al. Comparison of a DNA based PCR approach
with convetional methods for the detection of Mycobacterium tuberculosis in
Morocco. Mediterr J Hematol Infect Dis ; 4: e2012049 (2012).
29. Choi Y, Jeon BY, Shim TS. et al. Development of a highly sensitive one-tube
nested real-time PCR for detecting Mycobacterium tuberculosis Diagnostic
Microbiology and Infectious Disease 80 ; 299-303 (2014)
30. Peter J, Green C, Hoelscher M et al. Urine for the diagnosis of tuberculosis:
current approaches, clinical applicability, and new developments. Curr Opin Pulm Med. May; 16(3): 262-270 (2010).
31. Broger T, Sossen B, Toit E et al. Novel lipoarabinomannan point-of care
tuberculosis test for people with HIV: a diagnostic accuracy study. Lancet Infect
Dis. Aug;19(8):852-861 (2019).
32. Vollenhoven P, Heyns C, Beer P et al. Polymerase chain reaction in the diagnosis
of urinary tract tuberculosis. Urol Res ; 24: 107-111 (1996).
33. Heydari AA, Movahhede Danesh MR, Ghazvini K. Urine PCR evaluation to
diagnose pulmonary tuberculosis Jundishapur J Microbiol. Mar;7(3):e9311
(2014).
34. Armand S, Vanhuls P, Delcroix G. et al Comparison of the Xpert MTB/RIF test
with an IS6110-TaqMan real-time PCR assay for direct detection of
Mycobacterium tuberculosisin respiratory and nonrespiratory specimens. J Clin
Microbiol 49:1772-6 (2011).
35. Cousins DV, Wilton SD, Francis BR. Et al. Use of polymerase chain reaction for
rapid diagnosis of tuberculosis. J Clin Microbiol 30:255-8 (1992).
36. Tortoli E, Tronci M, Tosi CP. Et al. Multicenter evaluation of two commercial
amplification kits Amplicor, Roche and LCx, Abbott) for direct detection of Mycobacterium tuberculosis in pulmonary and extrapulmonary specimens.
Diagn Microbiol Infect Dis 33:173-9 (1999).
37. Torrea G, Perre P, Ouedraogo M. el al. PCR-based detection of the Mycobacterium tuberculosis complex in urine of HIV-infected and uninfected
pulmonary and extrapulmonary tuberculosis patients in Burkina Faso. J Med
Microbiol. Jan;54:39-44 (2005).
38. Peter J, Theron G, Muchinga T et al. The diagnostic accuracy of urine-based
Xpert MTB/RIF in HIV-infected hospitalized patients who are smear-negative
or sputum scarce. PLoS One. 7(7):e39966. (2012).
39. Lapausa M, Saldana A, Asensio A Extrapulmonary tuberculosis: an overview Rev
Esp Sanid Penit 17:3-11 (2015).
40. Mehta PK, Raj A, Singh N, Khuller GK. Diagnosis of extrapulmonary tuberculosis
by PCR. FEMS Immunol Med Microbiol. Oct;66(1):20-36 (2012).
41. Fortun J, Martin-Davila P, Gomez-Mampaso E, et al. Extra-pulmonary
tuberculosis: differential aspects and role of 16S-rRNA in urine. Int J Tuberc
Lung Dis. Apr;18(4):47-85 (2014).
42. da Cruz HL, de Albuquerque Montenegra R, de Arujo Lima JF. Et al. Evaluation of a nested-PCR for mycobacterium tuberculosisdetection in blood and urine
samples. Braz J Microbiol. Jan;42(1):321-9 (2011).
43. Jamshidi Makiani M, Davoodian P, Baghershiroodi M. et al. Urine-based nested
PCR for the diagnosis of Mycobacterium tuberculosis: A comparative study
between HIV-positive and HIV-negative patients. Jundishapur J Microbiol. Jul
26;9(8):e35634 (2016).
44. Nakiyingi L, Moodley VM, Manabe YC, et al. Diagostic accuracy of a rapid urine
lipoarabinomannan test for tuberculosis in HIV-infected adults. J Acquir
Immune Defic Syndr 66:370-9 (2014).
45. Talbot E, Munseri P, Teixeira P. et al. Test characteristics of urinary
lipoarabinomannan and predictors of mortality among hospitalized HIV-
infected tuberculosis suspects in Tanzania. PLoS One 7:e32876 (2012)
46. The use of lateral flow urine lipoarabinomannan assay (LF-LAM) for the
diagnosis and screening of active tuberculosis in people living with HIV. Policy
guidance. Geneva, Switzerland: WHO Press; (2015).
47. Paris L, magni R, Zaidi F, et al. Urine lipoarabinomannan glycan in HIV-negative
patients with pulmonary tuberculosis correlates with disease severity. Sci Transl med. Dec 13;9(420):eaal2807 (2017)
48. Patel K, Nagel M, Wesolowski M. et al. Evaluation of a urine-based rapid
molecular diagnostic test with potential to be used at point-of-care for
pulmonary tuberculosis: Cape Town Cohort. J Mol Diagn. Mar;20(2):215-224
(2018).
49. Labugger I, Heyckendorf J, Dees S, et al. Detection of transrenal DNA for the
diagnosis of pulmonary tuberculosis and treatment monitoring. Infection
45:269-276 (2017)
국문요약
연구 배경: 결핵은 세계적으로 높은 발병률과 사망률을 가지는 중요한 전염성 질 환으로 발병률과 사망률을 낮추기 위해서는 조기에 결핵을 진단할 수 있는 신속 하고 특이적이며 민감한 검사법이 매우 중요하다. 하지만 전통적으로 사용되고 있는 검사실 진단 방법인 객담 검체를 이용한 항산균 도말검사는 민감도가 낮으 며 항산균 배양검사는 오랜 시간이 소요되는 단점이 있다. 게다가 여성이나 어린 이, HIV 환자의 경우 객담을 잘 받지 못하며, 폐외결핵의 경우 침범장기에서 검체 를 얻으려면 침습적인 방법을 사용하여야만 한다. 따라서 비침습적이고 쉽게 채 취할 수 있는 검체를 사용한 민감한 검사법에 대한 연구가 이루어져왔다. 최근 들어 폐에서 결핵균이 파괴되면서 분리된 핵산이 다시 혈액을 통해 신장으로 이 동하여 신장의 사구체망을 거쳐 소변으로 배출되는 결핵균 특이 transrenal 유전 자에 대한 연구가 활발하게 이루어지면서 이를 중합효소연쇄반응과 같은 분자생 물학적 방법을 이용하여 결핵을 진단하는 방법이 각광을 받고 있다. 하지만 메타 분석에 따르면 결핵균 특이 transrenal 유전자의 결핵 및 폐외결핵에 대한 민감 도는 3.8-79%로 다양하게 보고되고 있다.
연구 목적: 본 연구에서는 소변 검체를 이용하여 빠르고 정확한 결핵균 검출을 위해 기존의 실시간 중합효소연쇄반응보다 특이도와 민감도를 향상시기기 위하 여 2개의 유전자를 사용하고(duplex), 한 튜브 안에 넣어 증폭시키는 이중 중합 효소연쇄반응(one-tube nested PCR)을 이용하여 새로운 결핵 진단법을 개발하고 자 하였다.
연구 방법: 본 연구에서 개발한 키트는 결핵균 특이 유전자인 IS6110 유전자와
rpoB 유전자를 동시에 표적으로 삼아 각 유전자에 특이적인 두 쌍의 시발체들
을 하나의 튜브안에 넣어 각각의 유전자에 대해 이중으로 중합효소연쇄반응을 수행하도록 하도록 설계되었으며 이를 위해 시발체 농도 및 증폭횟수를 변화시 켜 타당성을 검증하고 최적화하는 과정을 수행하였다. 결핵균 표준균주인 H37Rv DNA를 10ng 에서 10fg까지 10배 계대희석하여 실시간 중합효소연쇄반응의 주 형 유전자로 사용하였다.
연구 결과: 결핵균 검출을 위해 rpoB 유전자와 IS6110 유전자 각각의 단일 실시 간 중합효소연쇄반응과 단일 튜브 이중 실시간 중합효소연쇄반응의 민감도를 비 교분석한 결과 10pm 시발체의 농도를 사용하였을 때 10ng 에서 10fg까지의 감 지 시작 주기(cycle threshold) 값을 비교하였다. rpoB 단일 실시간 중합효소연쇄
반응, IS6110 단일 실시간 중합효소연쇄반응, rpoB 단일 튜브 이중 실시간 중합효
소연쇄반응, IS6110 단일 튜브 이중 실시간 중합효소연쇄반응, rpoB+IS6110 단일 튜브 이중 실시간 중합효소연쇄반응의 감지 시작 주기값은 각각 17.36에서 37.18, 14.95에서 34.88, 8.44에서 27.92, 5.83에서 26.36, 4.99에서 24.99 였다. 이 중 가
장 민감한 rpoB+IS6110 단일 튜브 이중 실시간 중합효소연쇄반응의 민감도를 상
승시키기 위해 10, 40주기에서 15, 25 주기로 변경하여 수행한 결과 10fg에서 1fg
까지의 민감도를 확인할 수 있었다. 위의 결과를 종합하였을 때 rpoB 유전자와
IS6110 유전자 모두를 표적으로 시발체농도를 10pm 로 사용하여 15주기를 선행 한 뒤 25주기를 수행하는 두 유전자 단일 튜브 이중 실시간 중합효소연쇄반응을 수행하였을 때 민감도가 가장 높은 것을 확인할 수 있었다. 새로 개발된 검사법 의 민감도와 특이도를 확인하기 위해 예비연구로 항산균 배양검사 양성인 활동 성 폐결핵 확진 환자의 임상검체 (객담 26검체, 소변 45검체)를 채취하고 정상인 임상검체 (객담 108검체, 소변 30검체)와 비교하여 검사를 시행하였다. 결핵환자 의 객담을 대상으로 한 실험은 기존에 상용화되어 있는 Real MTB-ID (M&D, Korea) 단일 실시간 중합효소연쇄반응 검사와 본 연구에서 개발한 검사법의 민 감도를 비교했을 때 각각 46.2% 와 100%로 새로 개발된 검사법이 더 높게 나타
났다. 결핵환자의 소변을 대상으로 한 실험은 기존에 상용화되어있는
AdvanSureTMTB/Nontuberculous mycobacterium (LG Lifescience, Korea) 단일 실시 간 중합효소연쇄반응 검사와 새로 개발된 검사법의 민감도를 비교하였으며, 각각 6.7% 와 51.1%로 새로 개발된 검사법이 더 높았다.
결론: 본 연구에서 개발된 IS6110 과 rpoB 의 두 유전자를 동시에 표적으로 수
행하는 두 유전자 단일 튜브 이중 실시간 중합효소연쇄반응 검사는 기존 상용화 되어 있는 검사법들보다 향상된 민감도로 소변 검체에서 결핵균을 검출하는데 성공하였다.