110
책임저자:박종민, 서울시 중구 을지로 6가 18-79
100-799, 국립의료원 외과 Tel: 02-2260-7157, Fax: 02-2269-0750 E-mail: [email protected]
접수일:2007년 7월 21일, 게재승인일:2007년 11월 13일 중심 단어: 위암, 배출구 폐색, 근치적 절제술
근치적 위절제술을 받은 위배출구 폐색증을 동반한 위암 환자의 임상 분석
국립의료원 외과
전영웅ㆍ이제희ㆍ김종흥ㆍ박종민
Clinicopathologic Analysis of Gastric Carcinoma Patients with Outlet Obstruction
Young Woong Jeon, M.D., Je Hee Lee, M.D., Jong Heung Kim, M.D. and Jong Min Park, M.D.
Department of Surgery, National Medical Center, Seoul, Korea
Purpose: This study was conducted to analyze the clinical course of patients of gastric cancer with outlet obstruction by comparing them with the gastric cancer patients without outlet obstruction.
Methods: The records of gastric cancer patients with outlet obstruction and who underwent radical gastrectomy from January 1996 to December 2005 were retrospectively re- viewed and compared with those patients with gastric cancer and who were without outlet obstruction.
Results: The number of the patients who underwent radical gastrectomy was 461. Out of 461 patients, the number of gastric cancer patients with outlet obstruction was 42 (9.1%), and they had nasogastric tube insertion for an average of 4.4 days before operation. These patients showed several significant features such as large tumor size, advanced stage, an increased the number of involved LNs, a low se- rum albumin level, a frequent antral tumor location and duo- denal invasion. There was no difference in complication rates between the two groups, but a higher mortality rate was not- ed in the gastric cancer patients with outlet obstruction than that in the other patients (P=0.038). The survival rate after the operation was significantly lower among the gastric can- cer patients with outlet obstruction (P=0.0008), whereas no difference was found in the survival rate between the above two groups at the same stage (P=0.1951).
Conclusion: The gastric cancer patients with outlet obstruc-
tion showed a comparatively poorer prognosis than those gastric cancer patients without outlet obstruction. However, there was no significant difference in the complication rate and the survival rate for both types of patients who were at the same stage. These results suggest that the patients with outlet obstruction can show the same result as the pa- tients without outlet obstruction by undergoing radical gast- rectomy. (J Korean Surg Soc 2008;74:110-114)
Key Words: Gastric cancer, Outlet obstruction, Radical gas- trectomy
서 론
위 배출구 폐색은 진행성 위암의 임상소견 중 하나이며, 위암뿐만 아니라 악성 십이지장 종양이나 췌장암에서도 나 타난다.(1) 이러한 소견을 보이는 환자들의 임상적 증상은 오심, 구토 및 이에 따른 식욕저하, 경구 섭취의 어려움, 체 중 감소 등이 있다. 배출구 폐색 환자들은 이러한 증상들로 인해 영양상태의 악화와 탈수, 체내 전해질 불균형에 의한 대사 이상 소견을 보인다.(2) 또한 위암에서의 배출구 폐색 은 오랜 기간 진행된 소견으로 인식되며, Volker 등은 배출 구 폐색 소견이 비교적 좋지 않은 예후를 나타내므로 이러 한 경우 치료자가 치료방법을 결정할 때 더욱 신중을 기해 야 한다고 보고하였다.(3)
위 배출구 폐색이 있을 때 그 치료방법으로 논의되고 있 는 것은 위공장 문합술(4) 또는 복강경적 위공장 문합술,(5) 스텐트를 이용한 내시경적 배출구 확장법(6) 등이 있는데, 이들은 주로 암의 원격전이에 의해 수술이 불가능한 상태 의 경우나, 고령과 같은 환자의 여러 상태를 고려하였을 때 근치적 수술이 불가능한 경우에서 서로 각각의 방법들의 비교정도에 국한되고 있을 뿐,(7-10) 위 배출구 폐색 환자에 서 근치적 위절제술을 시행하였을 때의 술 후 임상적 결과 에 대한 논의는 많지 않다.
본 연구에서는 위 배출구 폐색증을 보이는 환자들의 술 전 임상적 소견들과 근치적 위절제술을 시행 후의 임상적 결과 및 생존율을 위 배출구 폐색증이 없는 환자들의 임상
Table 1. Comparison of clinicopathologic characteristics between patients with and without gastric outlet obstruction
Patients Patients
without with
Characteristics outlet outlet P-value
obstruction obstruction (n=419) (n=42)
Sex 0.858
Male 298 (71.1) 31 (73.8)
Female 123 (28.9) 11 (26.2)
Age (years) 59.5±11.3 61.3±11.5 0.332
Albumin (g/dl) 3.8±0.6 3.3±0.6 0.0001
Tumor location 0.001
Antral 207 (49.4) 32 (76.2)
Non-antral 212 (50.6) 10 (23.8)
Histology 1.000
Differentiated 184 (43.9) 18 (42.9) Undifferentiated 235 (56.1) 24 (57.1) Largest diameter (mm) 52.2±30.8 78.4±44.6 0.001
Macroscopic finding 0.001
EGC 162 (38.6) 0
Borrmann type I, II 35 (8.4) 4 (9.5) Borrmann type III, IV, V 222 (53.0) 38 (90.5)
Duodenal invasion 0.0001
No 376 (89.7) 14 (33.3)
Yes 43 (10.3) 28 (66.7)
Length of distal margin (mm) 53.3±49.3 19.0±15.9 0.0001 No of LN examined 24.2±12.5 32.1±14.7 0.0001 No of metastatic LN 3.8±7.2 8.6±7.5 0.0001
Stage 0.0001
Ia∼II 265 (63.4) 6 (14.3)
IIIa∼IV 153 (36.6) 36 (85.7)
Gastrectomy 0.420
Subtotal 332 (79.2) 36 (85.7)
Total 87 (20.8) 6 (14.3)
Major complications 0.960
No 368 (87.3) 37 (88.1)
Yes 51 (12.2) 5 (11.9)
Operative mortality 4/419 (1.0) 2/42 (4.8) 0.038 경과와 비교함으로써, 배출구 폐색을 동반한 위암 환자의
임상경과를 분석하고자 한다.
방 법
1996년 1월부터 2005년 12월까지 10년간 국립의료원 외 과에서 위암으로 근치적 위절제술을 받은 위암 환자들 중 위배출구 폐색증을 동반한 위암(이하 폐색형 위암)으로 진 단되었던 예를 대상군으로 하였다. 위배출구 폐색증은 문 진, 이학적 소견, 내시경 검사, 복부 단순 사진 및 복부 전산 화 단층 사진 기록 등을 통해 병변에 의한 기계적 폐색이나 위암 병변에 의한 위벽의 침윤으로 연동 운동 장애가 있어 구토, 경구 음식물 섭취 곤란, 8시간 이상의 금식 후 실시한 내시경 검사 소견상 위 내 음식물 정체 및 위 팽만 등의 소 견이 있는 경우로 정의하였다.(11) 위암 환자들의 기본 자 료가 기록되어 있는 Visual FoxPro (Microsoft Corporation, version 6.0) 자료 파일에서 본 연구의 대상인 근치적 위절제 술례들을 선별하여, 각종 통계 처리를 위하여 Windows용 SPSS (Release 10.07, SPSS Inc.) 파일로 전환하여 분석하였 다. 분석에 포함된 항목들은 성별, 연령, 위배출구 폐색 유 무, 입원 시 알부민 수치, 비위관 삽입여부, 위암의 위치, 위 암의 크기, 육안적 분류, 위벽 침윤도, 림프절 전이, 조직학 적 분류, 십이지장 침윤 유무, 원위부 절단면 길이, 위절제 범위, 병기, 환자의 추적 결과 등이다. 모든 항목은 대한위 암학회의 위암 기재사항을 위한 설명서에 따라 기재하였으 나, 위암의 위치는 위암의 주 점거부위가 전정부인가를 기 준으로 전정부/비전정부, 육안적 분류는 위암 경계부가 뚜 렷한가를 기준으로 Borrmann I, II/III, IV, V, 조직학적 분류 는 Nakamura의 분류법에 따라 분화형/비분화형, 병기는 Ia
∼II/IIIa∼IV로 각각 단순화하여 분류하였다.(12) 폐색증 유 무에 따른 여러 임상병리학적 인자들의 평균치 비교는 t test로, 교차 분석은 Chi-square test나 Fisher's exact test로 하 였다. 수술 합병증 분석 시에는 입원 기간의 연장이나 재수 술이 필요한 경우 또는 환자의 생존을 위협할 수 있는 중증 합병증들만을 포함시켜 분석하였는데, 한 합병증의 속발성 으로 발생한 합병증(예: 십이지장 단단부 누출에 속발하여 발생한 복강 내 농양)은 분석대상에 포함시키지 않았다. 생 존율 분석 시의 추적완료시점은 2006년 12월 31일이었으 며, 각 집단별 생존율의 비교분석 시에는 추적 중단 예, 추 적 시점까지 생존한 예 및 위암의 재발이 아닌 다른 사인으 로 사망한 예 등은 중도절단 예로 처리하여 생존율을 비교 하였다. 각 집단별 생존율은 Kaplan-Meier법으로 구하여 Log rank test를 이용하여 비교하였다. 모든 통계처리는 P값 이 0.05 미만인 경우 유의하다고 판정하였다.
결 과
1996년 1월부터 2005년 12월까지 만 10년간 위암으로 위 절제술을 받은 환자 509명 중 잔류암이 없는 근치적 절제술 을 받은 환자는 461명이었고, 그 중 폐색형 위암 환자는 42 명으로 근치적 위절제술 예의 9.1%였다. 모든 폐색형 위암 환자에서 첫 내시경 검사 후 금식 및 경정맥 영양 요법을 하였으며 내시경 검사를 다시 하였는데 34예서는 비위관 삽관으로 위내용물을 제거하여야 하였다. 이들의 술 전 평 균 비위관 삽관기간은 4.4일이었다. 폐색형 위암환자군과 비폐색형 위암환자군의 임상병리학적 특징은 Table 1에 요
Table 2. Comparison of major postoperative complications and op- erative mortality between patients with and without gas- tric outlet obstruction
Patients Patients
without with
Complications
outlet outlet
obstruction obstruction
Pneumonia 15 (1) 4
Wound dehiscence 5
Leaking, duodenal stump 5 1 (1)
Leaking, esophagojejunostomy 1
Intraabdominal abscess 7 (1)
Intraabdominal bleeding 4
Intraluminal bleeding 2
Chylous ascites 4
Acute pancreatitis 3 (2)
Stricture, esophagojejunostomy 3
E loop syndrome 3
A loop syndrome 1
Gastric atony 4
Serious arrhythmia 2
Heart failure 1
Acute myocardial infarction 1 1 (1)
Figures in parenthesis refer to number of operative mortality.
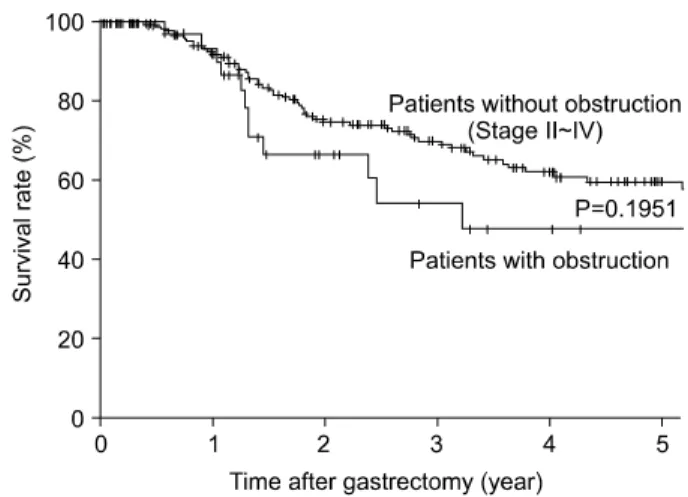
Fig. 1. Comparison of Survival rates between Patients with malig- nant gastric outlet obstruction and stage II∼IV patients without malignant gastric outlet obstruction.
약되어 있다. 종양의 크기, 전이된 림프절의 수 등에서 통계 적으로 의미있는 차이를 보여 폐색형 위암이 비폐색형 위 암보다 진행된 병기의 비율이 많았다. 또, 위전정부에 위치 하고 십이지장을 침윤한 위암의 빈도가 비폐색형에 비해 유의하게 높아 내강이 좁은 전정부에 위치하거나 유문륜을 침범한 진행성 위암에 의한 기계적 폐색증이 위배출구 폐 색증의 주요 원인임을 보여 주고 있었다. 그러나, 전정부 이 외의 곳에 위치한 위암도 폐색형 위암의 23.8% (10/42)에서 관찰되었다. 이들의 평균 최장경은 126.3 mm (95∼230 mm) 이며 육안 소견은 Borrmann III형 4예, IV형 6예로 위벽의 넓은 범위에 걸친 침윤성 병변에 의한 기능성 폐색증을 일 으킨 경우들로 판단된다.
근치적 절제술을 받은 461명 중 56명(12.1%)에서 주요 합 병증이 발생하였는데, 비폐색형 위암 419명 중 51예(12.2%) 에서 16가지, 폐색형 위암 42명 중 5예(11.9 %)에서 3가지의 주요 합병증이 각각 발생하여 양 군 간 발생 빈도의 차이는 없었으나, 합병증 발생으로 인한 사망률은 비폐색형 위암 4예(1.0%), 폐색형 위암 2예(4.8%)로 양 군 간 유의한 차이 를 관찰할 수 있었다(P=0.038). 술 후 합병증은 주로 폐렴, 십이지장 단단부 누출, 복강 내 농양 등이었으며, 술 후 사 인은 급성 췌장염, 폐렴, 급성 심근경색 등이었다(Table 2).
근치적 위절제술을 받은 461예의 5년 생존율은 71.7%였 으며, 비폐색형 위암 419예와 폐색형 위암 42예의 5년 생존
율은 각각 73.8%, 47.7%로 이 두 군 간에는 유의한 생존율 의 차이를 보였다(Logrank test, P=0.0008). 그러나, 폐색증례 가 없는 제 IA, IB 병기 환자 198예를 제외한 폐색증을 동반 하지 않은 II∼IV 병기 환자 221예의 생존율 59.8%와의 비 교시에는 폐색증 예의 생존율이 역시 낮으나 통계적으로 유의한 차이는 아니었다(Logrank test, P=0.1951)(Fig. 1).
고 찰
폐색형 위암은 임상적으로 오심, 구토, 경구섭취의 어려 움으로 인한 탈수, 영양상태의 이상, 전해질 이상을 동반한 다.(2) 따라서 술 전 이에 대한 교정이 우선적으로 필요하며 대부분의 경우가 높은 병기의 형태로 진행되어 술기적으로 더 섬세하고 광범위한 위 절제술을 필요로 한다.
술 전 영양상태에 대한 평가는 이 연구에서 총체적으로 다루어지지 않았지만 비교적 흔한 판단기준으로 쓰이는 알 부민 수치를 비교해 보았을 때 폐색형 위암환자에서 유의 하게 낮아 폐색형 위암환자의 술 전 영양상태의 저하를 알 수 있었다.(13) 그리고 음식물의 배출 지연으로 인해 반복 된 내시경상에서도 음식물의 위 내 정체가 관찰되어 비위 관 삽관을 하여 위 내용물을 제거하였다. 배출구 폐색에 의 한 음식물의 위내 저류와 광범위한 암 침윤으로 인한 연동 운동의 저하가 구토와 흡수장애를 유발하여 술 전 전해질 이상과 영양상태의 저하를 일으키는 것을 알 수 있었다.
위암 병변의 크기, 전이된 림프절의 수, 병기 등이 폐색형 위암에서 통계적으로 유의하게 높게 나타났다. 이와 같은 결과로 위암 환자에서의 배출구 폐색 증상은 다른 위암보 다 더욱 진행된 형태임을 예측할 수 있었다. 또한 위 전정부 나 유문륜에 위치하고, 십이지장을 침범한 예에서 폐색소 견을 더 보이는 것으로 관찰되었으나, 병기가 낮은 위암이
유문륜이나 내강이 좁은 전정부를 침범하여 폐색소견을 유 발한 경우도 있었다.
Borrmann type과 폐색유무는 통계적으로 유의한 차이는 없었다. 그러나, 비전정부에 위치한 4예의 Borrmann type III 와 6예의 Borrmann type IV 병변이 폐색을 일으키는 결과로 보아 광범위한 위암의 침윤이 위의 연동운동 저하를 유발 하여 기능적 폐색을 유발함을 알 수 있었다.
합병증 발생여부는 두 대조군 간 유의한 차이를 보이지 않았다. 이는 폐색형 위암환자들이 술 후 충분한 환자관리 및 적극적인 치료로 영양상태 이상이나 대사 이상 등의 합 병증을 유발할 수 있는 여러 요소들을 극복할 수 있음을 보여주고 있으며,(14) 폐색형 위암이라는 요소가 술 후 환 자상태에 영향을 주는 것은 아니라는 것을 알 수 있었다.
폐색형 위암 환자의 수술 술기상의 문제점은 술 전 위강 내 감압이나 위 내용물의 제거가 불충분한 경우, 절제시나 문합 시에 기술적 어려움을 유발하고, 위강 내 남아있던 내 용물이 흘러나옴으로 감염과 동반된 합병증이 나타날 수 있다. 그러나 비폐색형 위암환자와의 술 후 합병증 발생률 에 유의한 차이가 없었던 점으로 보아 술 전 비위관 삽입을 통한 감압으로 충분히 합병증 발생을 막을 수 있음을 알 수 있었다. 합병증 발생에 따른 사망률은 통계적으로 유의 한 차이를 보였다. 그러나 본 연구에서 폐색형 위암환자의 증례가 적어 좀 더 많은 대조군을 통한 사망률의 비교가 이루어진다면 폐색형 위암과 사망률의 연관성을 명확히 알 수 있을 것이다.
생존율의 단순 비교에 있어서는 두 군 사이에 유의한 차 이를 보였으나 폐색형 위암의 경우 대부분 진행된 병기였 음을 감안하여 비폐색형 위암환자에서의 II∼IV병기와 비 교하였을 때, 통계적으로 유의한 차이는 없었다. 이는 폐색 형 위암 환자의 생존율이 병기와 밀접한 연관성이 있다는 것을 의미한다.
지금까지 발표된 폐색형 위암에 관한 연구 중, 몇몇 연구 는 폐색형 위암에 대한 고식적 치료가 술 후 긍정적 결과를 보였다고 보고하고 있다.(15-17) 최근 발표된 연구에서는 폐색형 위암의 절반정도가 제 4형 병기이며, 이들 4형 병기 위암에서의 합병증을 예방한다면 위 절제술이 환자들의 생 존율을 증가시키고 좋은 예후를 보인다고 보고하고 있다.(18) 이런 결과들을 바탕으로 향후 폐색형 위암의 병기별 임상 경과 및 근치적, 고식적 치료에 대한 연구가 시행되어야 하 겠다.
결 론
폐색형 위암환자의 치료에 있어서 술 전 영양상태, 전해 질 불균형 등의 정확한 평가와 교정이 필요하며 비위관 삽 관을 통한 충분한 감압으로 근치적 수술을 시행할 수 있다 면 동일한 병기의 비폐색형 위암과 동일한 치료성적을 얻
을 수 있을 것이다.
본 연구는 폐색형 위암 환자에 대한 후향적 연구로 수술 전후의 영양상태의 평가나 술 후 합병증 발생, 생존율 비교 를 위한 환자군의 선택에 많은 제약을 가지고 있어 추가적 인 연구가 필요할 것으로 보인다. 또한 배출구 폐색을 가진 위암환자의 각 병기에 따른 근치적, 고식적 치료에 대한 연 구가 필요할 것이다.
REFERENCES
1) Chopita N, Landoni N, Ross A, Villaverde A. Malignant gas- troenteric obstruction: therapeutic options. Gastrointest Endosc Clin N Am 2007;17:533-44, vi-vii.
2) McCauley M, Gunawardane M, Cowan MJ. Severe metabolic alkalosis due to pyloric obstruction: case presentation, evalua- tion, and management. Am J Med Sci 2006;332:346-50.
3) Kahlke V, Bestmann B, Schmid A, Doniec JM, Kuchler T, Kremer B. Palliation of metastatic gastric cancer: impact of preoperative symptoms and the type of operation on survival and quality of life. World J Surg 2004;28:369-75.
4) Stupart DA, Panieri E, Dent DM. Gastrojejunostomy for gas- tric outlet obstruction in patients with gastric carcinoma. S Afr J Surg 2006;44:52-4.
5) Khan AZ, Miles WF, Singh KK. Initial experience with lapa- roscopic bypass for upper gastrointestinal malignancy: a new option for palliation of patients with advanced upper gastro- intestinal tumors. J Laparoendosc Adv Surg Tech A 2005;
15:374-8.
6) Kim TO, Kang DH, Kim GH, Heo J, Song GA, Cho M, et al. Self-expandable metallic stents for palliation of patients with malignant gastric outlet obstruction caused by stomach cancer. World J Gastroenterol 2007;13:916-20.
7) Mittal A, Windsor J, Woodfield J, Casey P, Lane M. Matched study of three methods for palliation of malignant pylo- roduodenal obstruction. Br J Surg 2004;91:205-9.
8) Del Piano M, Ballare M, Montino F, Todesco A, Orsello M, Magnani C, et al. Endoscopy or surgery for malignant GI out- let obstruction? Gastrointestinal Endoscopy 2005;61:421-6.
9) Maetani I, Akatsuka S, Ikeda M, Tada T, Ukita T, Nakamura Y, et al. Self-expandable metallic stent placement for palliation in gastric outlet obstructions caused by gastric cancer: a com- parison with surgical gastrojejunostomy. J Gastroenterol 2005;
40:932-7.
10) Adler DG, Baron TH. Endoscopic palliation of malignant gas- tric outlet obstruction using self-expanding metal stents: expe- rience in 36 patients. Am J Gastroenterol 2002;97:72-8.
11) Vestweber KH, Troidl H, Koslowski A, Bouillon B. Gastric outlet stenosis (benign): definition, incidence, therapy? Lan- genbecks Arch Chir 1985;366:107-11.
12) Nakamura K. Structure of the Gastric Cancer. 1st ed. Tokyo:
Igaku-Shoin; 1982.
13) Rey-Ferro M, Castano R, Orozco O, Serna A, Moreno A.
Nutritional and immunologic evaluation of patients with gas- tric cancer before and after surgery. Nutrition 1997;13:878-81.
14) Ebata T, Hayasaka H. Pre- and postoperative nutritional man- agement in gastric cancer patients. Gan To Kagaku Ryoho 1988;15:820-6.
15) Watanabe A, Maehara Y, Okuyama T, Kakeji Y, Korenaga D, Sugimachi K. Gastric carcinoma with pyloric stenosis. Surgery 1998;123:330-4.
16) Sasako M, Maruyama K. Is palliative gastrectomy for linitis
plastica effective? Shoukakigeka 1996;19:1445-52.
17) Koga S, Kawaguchi H, Kishimoto H, Tanaka K, Miyano Y, Kimura O, et al. Therapeutic significance of noncurative gas- trectomy for gastric cancer with liver metastasis. Am J Surg 1980;45:1183-8.
18) Mizutami S, Shioya T, Maejima K, Yoshino M, Komine O, Bou H, et al. Significancer of gastrectomy as palliative surgery for gastric carcinoma with pyloric stenosis. J Nippon Med Sch 2007;74:241-5.