Korean J Gastroenterol Vol. 67 No. 5, 282-285 http://dx.doi.org/10.4166/kjg.2016.67.5.282 pISSN 1598-9992 eISSN 2233-6869
IMAGE OF THE MONTH
Korean J Gastroenterol, Vol. 67 No. 5, May 2016 www.kjg.or.kr
젊은 여자에서 만성췌장염 급성 악화로 진단된 불완전 분할췌
김의주, 김연석, 조재희
가천대 길병원 소화기내과
Incomplete Pancreas Divisum Presented with Acute Exacerbation of Chronic Pancreatitis in a Young Female
Eui Joo Kim, Yeon Suk Kim, and Jae Hee Cho
Division of Gastroenterology, Department of Internal Medicine, Gachon University Gil Medical Center, Incheon, Korea
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2016. Korean Society of Gastroenterology.
교신저자: 조재희, 21565, 인천시 남동구 남동대로 774번길 21, 가천대 길병원 소화기내과
Correspondence to: Jae Hee Cho, Division of Gastroenterology, Department of Internal Medicine, Gachon University Gil Medical Center, 21 Namdong-daero 774 beon- gil, Namdong-gu, Incheon 21565, Korea. Tel: +82-32-460-3778, Fax: +82-32-460-3408, E-mail: jhcho9328@gmail.com
Financial support: None. Conflict of interest: None.
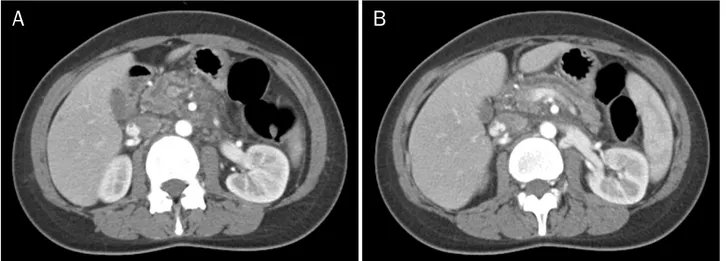
Fig. 1. Abdominopelvic CT images at the initial presentation. (A) CT image showing dilated pancreatic duct (PD) at the head portion of pancreas with atrophic parenchyme and peri-pancreatic inflammatory change. (B) CT image showing dilated PD at the body and tail portion of pancreas.
증례: 평소 특이 병력이 없던 22세 여자가 사흘 전 소량의 음주 후 이틀 전부터 시작된 상복부 통증을 주소로 내원하였 다. 복통은 식사와 무관하였고, 지속적인 양상이었다. 흡연력 은 없었으며, 1주일에 1회, 회당 소주 한두 잔 가량의 사교적 음주력이 있었다. 수술력이나 특이 과거력은 없었고, 췌장염, 췌장암 등의 가족력은 없었다. 내원 시 38.0oC의 발열 외에 혈압, 맥박을 포함한 활력 징후는 정상이었고, 상복부에 경동의
반발 압통이 관찰되었다. 키 175.1 cm에 몸무게는 65.2 kg으로 BMI는 21.3 kg/m2으로 확인되었다. 내원 시 시행한 혈액검사 에서 혈색소 12.4 g/dL, 백혈구 15,430/mm3, 총 빌리루빈 2.2 mg/dL, AST 22 IU/L, ALT 11 IU/L, ALP 65 IU/L로 확인되 었고, 아밀라아제 141 U/L, 리파아제 71 IU/L, CRP 9.83 mg/일로 상승되어 있었으며, CA 19-9와 IgG4는 각각 12.51 U/mL, 64.5 mg/일로 정상 범위 내로 확인되었다. 복부 CT에
Kim EJ, et al. Incomplete Pancreas Divisum Presented with Acute Exacerbation of Chronic Pancreatitis
283
Vol. 67 No. 5, May 2016
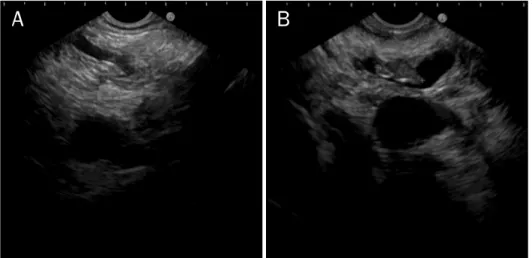
Fig. 2. Endoscopic ultrasonography.
(A) No abnormal finding at common bile duct. (B) Dilated pancreatic duct (6 mm) with sludge.
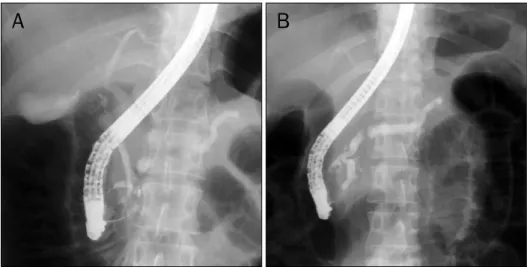
Fig. 3. ERCP images. (A) Pancreatogram showing dilated pancreatic duct (6 mm) with multiple large amounts of sludge. (B) Endoscopic image showing retracted pancreatic sludge via minor papilla with endoscopic basket after endoscopic sphincterotomy. (C) Post ERCP fluoroscopic image showing an endoscopic retrograde bile duct drainage stent and an endoscopic retrograde pancreatic duct drainage stent.
서 췌관의 확장 및 췌장 주변의 염증을 관찰할 수 있었으나, 담낭 및 담관, 췌관 내 결석은 관찰되지 않았다(Fig. 1). 환자 는 내원 2일째 췌장염의 원인 감별을 위해 내시경 초음파검사 (EUS)를 시행하였다(Fig. 2). EUS에서 담낭, 담관 내 결석은 관찰되지 않았으나, 위축된 췌장 실질과 더불어 미만성 췌관 확장이 관찰되었고, 췌관 내에 CT로는 보이지 않았던 다량의 오니(sludge)를 확인할 수 있었다. EUS elastography에서 strain ratio는 head에서 4.18, body에서 4.50으로 정상치보 다 높게 측정되었다. 이후 내시경 역행성 담췌관조영술 (ERCP)을 시행하여, 대유두부로 췌관 삽관을 시도하였으나 원활히 진행되지 않아 소유두부를 침형 유두절개도(needle- knife papillotome)로 절개한 후 성공적으로 췌관 삽관을 진 행하였다. 췌관 조영술에서 췌관 내 다량의 오니를 관찰할 수 있었고, 배측 췌관과 복측 췌관의 연결을 확인하여 불완전 분
할췌로 인한 만성췌장염을 진단하였다. 이후 Hurricaine bal- loon (diameter 8 mm; Boston Scientific, Cork, Ireland)을 이용하여 두 차례에 걸쳐 각각 30초간 내시경적 소유두부 유 두괄약근 풍선확장술을 추가로 시행하고 풍선도관(retrieval balloon)과 바스켓(Dormia basket)을 이용하여 다량의 췌관 내 오니(sludge)를 제거하였다. 이후 소유두부와 대유두부를 통해 플라스틱 췌관 스텐트(straight type 7 fr 10 cm, 5 cm;
Cook Ireland Ltd., Limerick, Ireland)를 십자형으로 삽입하 였다(Fig. 3). 이후 복통을 포함한 임상 증상과 혈액검사를 포 함한 임상 소견의 호전 양상이 관찰되어 퇴원하였고, 3개월 추적 복부 CT 촬영 및 ERCP에서 췌장염과 췌관 확장의 호전 을 확인하고 췌관 스텐트를 제거하였다. 현재는 퇴원 9개월째 로 외래에서 특이 합병증 없이 추적관찰 중이다(Fig. 4).
284
김의주 등. 만성췌장염의 급성 악화로 진단된 불완전 분할췌The Korean Journal of Gastroenterology
Fig. 4. Follow-up (ERCP). (A) Cholan- giopapncreatography showing dorsal pancreatic duct crossing over the common bile duct. (B) Pancreato- gram showing dorsal pancreatic duct communicating with main pancreatic duct and ventral pancreatic duct.
진단: 불완전 분할췌(incomplete pancreas divisum)로 인한 만성췌장염
분할췌는 발생학적인 이상으로, 기본적으로 췌장은 원시앞 창자(primitive foregut)에서 시작된 두 개의 싹으로부터 발생 하여 두 싹이 융합하는 과정을 거쳐 하나의 장기로 변화하는 과정을 거치게 된다. 두 개의 싹이 융합에 실패할 경우 배측과 복측의 췌장(dorsal and ventral pancreas)이 동시에 존재하 게 되며, 각각 배측췌관은 부유두부로, 복측췌관은 주유두부 로 췌액을 배출하는 췌관을 따로 갖게 되는 분할췌가 된다.
이는 췌장과 관련된 가장 흔한 발생학적 변이로, 서양의 기존 보고에서는 전체 인구의 약 8-10%가 분할췌를 갖고 있는 것 으로 알려져 있으나, 한국인을 대상으로 한 국내 다기관 연구 에서는 0.49%로 보고된 바 있으며, 일본의 결과에서도 분할 췌는 1% 이하로 보고되고 있어 동양에서는 서양에 비하여 분 할췌의 유병률이 낮은 것으로 생각된다.1-3
이 중 일부에서 췌장염이 반복적으로 재발하여 만성췌장염 으로 진행할 수 있으며, 이것은 분할췌에서 상대적으로 더 많 은 양의 췌액이 직경이 작은 소유두부를 통하여 배액되면서 췌장액의 저류가 유발되기 때문인 것으로 여겨진다. 따라서 분할췌에서 발생한 췌장염은 소유두부 절개술(minor papil- lotomy)을 통하여 배측 주췌관의 배액을 원활하게 해줌으로 써 치료하게 되는데, 분할췌로 인한 급성 재발성 췌장염 환자 의 80%에서 치료효과를 갖는 것으로 알려져 있다.4 그러나 이 미 만성췌장염 및 만성 통증이 동반된 환자에서 급성 악화가 병발하였을 때에는 이미 해부학적인 변화가 초래되어 있기 때 문에 이보다는 치료효과가 떨어지는 것으로 보고되고 있다.5 재발성 급성췌장염과 만성췌장염의 원인으로는 대표적으 로 담석과 음주, 고중성지방혈증, 고칼슘혈증과 같은 대사 이 상이 있으며, 이러한 대표적인 원인에 해당되지 않는 경우 해 부학적 변이, 자가면역 췌장염이나 유전적 요인에 의한 췌장 염을 고려해볼 수 있다.6 젊은 여성에서 발생할 수 있는 만성
췌장염의 원인으로 PRSS1 gene mutation, SPINK1 gene mutation, CFTR gene mutation을 포함한 hereditary pan- craitits의 가능성을 고려해 볼 수 있으며,7-9 이 증례의 경우 여건상 환자에게서 유전학적 검사를 하지 못했으나 췌장염의 가 족력이 없고 분활췌 소견이 관찰되어 선천성 기형(congenital anomaly)으로 인한 만성췌장염으로 진단할 수 있었다.
분할췌에 의한 췌장염은 해부학적 변이에 의한 췌장염 중 가장 흔한 원인이며, 이 경우 소유두부 절개를 통하여 좋은 치료 결과를 얻을 수 있다. 특히 이번 증례와 같이 젊은 환자 의 경우 향후 만성췌장염의 악화와 반복적인 췌장염 발생을 예방할 수 있기 때문에, 젊은 연령의 췌장염 환자의 진단과 치료에 있어서는 분할췌에 대한 감별이 반드시 필요하다.
REFERENCES
1. Burtin P, Person B, Charneau J, Boyer J. Pancreas divisum and pancreatitis: a coincidental association? Endoscopy 1991;23:
55-58.
2. Kasugai T, Kuno N, Kobayashi S, Hattori K. Endoscopic pan- creatocholangiography. I. The normal endoscopic pancreato- cholangiogram. Gastroenterology 1972;63:217-226.
3. Kim MH, Lim BC, Park HJ, et al. A study on normal structures, var- iations, and anomalies of the Korean pancreaticobiliary ducts:
cooperative multicenter study. Korean J Gastrointest Endosc 2000;21:624-632.
4. Lans JI, Geenen JE, Johanson JF, Hogan WJ. Endoscopic therapy in patients with pancreas divisum and acute pancreatitis: a pro- spective, randomized, controlled clinical trial. Gastrointest Endosc 1992;38:430-434.
5. Lehman GA, Sherman S, Nisi R, Hawes RH. Pancreas divisum:
results of minor papilla sphincterotomy. Gastrointest Endosc 1993;39:1-8.
6. Cho DH, Song TJ. Evaluation and treatment of recurrent acute pancreatitis. Korean J Pancreas Biliary Tract 2016;21:1-10.
7. Rho ES, Kim E, Koh H, Yoo HW, Lee BH, Kim GH. Two cases of
Kim EJ, et al. Incomplete Pancreas Divisum Presented with Acute Exacerbation of Chronic Pancreatitis
285
Vol. 67 No. 5, May 2016 chronic pancreatitis associated with anomalous pancreati-
cobiliary ductal union and SPINK1 mutation. Korean J Pediatr 2013;56:227-230.
8. Oh HC, Lee TY, Kwon S, et al. SPINK1 N34S mutation as a possi- ble cause of chronic pancreatitis in a patient with familial
background. Korean J Gastroenterol 2007;49:384-389.
9. Chen JM, Férec C. Genetics and pathogenesis of chronic pan- creatitis: the 2012 update. Clin Res Hepatol Gastroenterol 2012;36:334-340.