132
Copyrights © 2014 The Korean Society of RadiologyINTRODUCTION
Primary renal osteosarcoma is extremely rare and only 27 cases have been reported (1). Most cases show bizarre calcifica- tions within the renal contour (2, 3). To our knowledge, there have been no cases of primary osteosarcoma presenting as hy- dronephrotic kidney.
Hence, we report the first such case with CT findings and a literature review.
CASE REPORT
A 76-year-old man with a six-month history of left lower ab- dominal pain and weight loss was presented to the outpatient ward of our hospital. His medical history was unremarkable.
Aside from a higher than normal serum alkaline phosphatase level of 262 IU/L (normal range: 40−129 IU/L), blood test re-
sults were within the normal range. The serum levels of tumor markers carcinoembryonic antigen, CA 19-9, and CA 72-4 were under the respective limits. A urinalysis showed microscopic hematuria, though the urine was sterile on culture and urine cy- tology yielded no malignant cells. Bone scan and skeletal survey results were normal, as was a chest radiograph.
On physical examination, a huge palpable mass was detected by the urology surgeon in the left lower quadrant of the abdo- men.
Initial simple abdominal radiography indicated a soft tissue density mass with some calcifications, as well as lateral displace- ment of the adjacent bowel loops (Fig. 1A).
Three-dimensional kidney multidetector CT imaging (Light- Speed VCT; GE Healthcare, Milwaukee, WI, USA) was per- formed. On precontrast scans, there were dense amorphous or nodular calcifications and irregular solid components in the large mass (Fig. 1B, C). On postcontrast axial scans, irregular
Case Report
pISSN 1738-2637 / eISSN 2288-2928 J Korean Soc Radiol 2014;71(3):132-135 http://dx.doi.org/10.3348/jksr.2014.71.3.132
Received April 8, 2014; Accepted July 10, 2014 Corresponding author: You Me Kim, MD
Department of Radiology, Dankook University Hospital, Dankook University College of Medicine, 201 Manghyang-ro, Dongnam-gu, Cheonan 330-715, Korea.
Tel. 82-41-550-6921 Fax. 82-41-552-9674 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
This study was done in accordance with a research protocol approved by the Institutional Review Board of Dankook University Hospital and waived the requirement for informed consent because it was a retrospective study.
Primary renal osteosarcoma is an extraordinarily rare primary tumor of the kidney.
It occurs mostly in middle-aged and older individuals, and generally presents with non-specific symptoms such as abdominal pain, weight loss, palpable mass, and gross hematuria. Radiographically bizarre renal calcifications are often indicative of this uncommon neoplasm. Herein we report a case of primary osteosarcoma in a hydronephrotic kidney of a 76-year-old man, who developed lung metastasis soon after a radical nephrectomy. To the best of our knowledge, this is the first computed tomography based report of a patient with the hydronephrotic form of primary re- nal osteosarcoma.
Index terms
Primary Renal Osteosarcoma Kidney
Multidetector Computed Tomography
Primary Renal Osteosarcoma Presenting as Hydronephrotic Kidney:
A Case Report with Imaging Findings and a Literature Review
1 수신증으로 발현된 원발성 신장 골육종: 증례 보고1Jae Wook Lee, MD
1, Ji Hae Koo, MD
2, You Me Kim, MD
1Departments of 1Radiology, 2Pathology, Dankook University Hospital, Dankook University College of Medicine, Cheonan, Korea
Jae Wook Lee, et al
133
jksronline.org J Korean Soc Radiol 2014;71(3):132-135
We performed a left radical nephrectomy with left hemicolec- tomy due to adhesion. The resected specimen measured 20 × 16
× 4 cm. A pathologic specimen revealed marked dilation of the left kidney and irregular solid masses with multiple calcifications in the dilated lower portion. The left ureter could not be identi- fied grossly or pathologically probably due to severe destruction and adhesion. The left colon that was adherent to the kidney showed severe adhesion but no evidence of invasion. Histopath- ologic and immunohistochemical analysis of specimens revealed the characteristic pattern of classic osteosarcoma with immature neoplastic osteoids and sarcomatoid stroma (Fig. 1F). The final diagnosis was primary renal osteosarcoma in the lower portion enhancing solid areas were noted along the peripheral and cen-
tral portion of the mass with focal fat obliteration between the mass and left descending colon (Fig. 1D). A reformatted coronal scan clearly revealed the marked hydronephrosis, calcifications and irregular enhancing solid areas in the lower portion of the left kidney (Fig. 1E). No evidence of hepatic metastasis or re- gional lymphadenopathy was found.
Based on the radiological findings, our initial diagnosis was transitional cell carcinoma, arising from longstanding hydrone- phrosis likely due to ureteropelvic junction (UPJ) stricture. Sar- cormatoid renal cell carcinoma was included in the differential diagnosis.
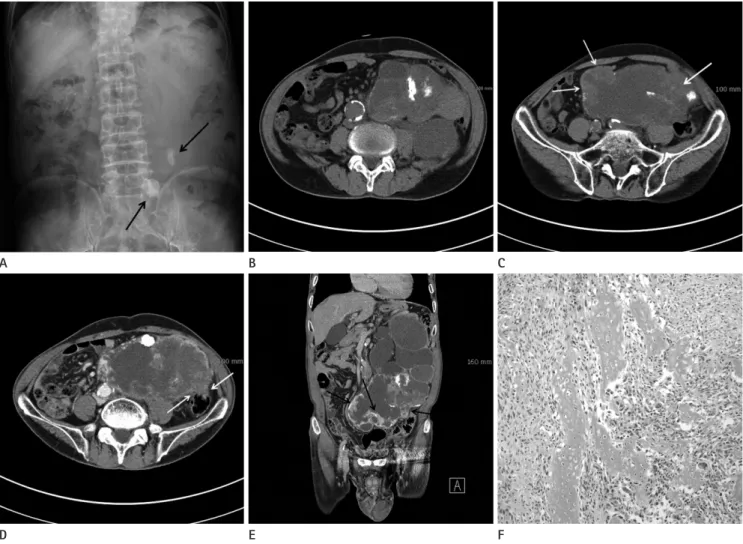
Fig. 1. A 76-year-old man with primary renal osteosarcoma.
A. Simple radiography shows soft tissue density mass on the left side of abdomen with calcifications (arrows).
B, C. Precontrast CT scans show amorphous or nodular calcifications and irregular soft tissue components (arrows) within the mass.
D. Postcontrast axial CT scan shows irregular enhancing solid areas along the peripheral and central portion of the mass with focal fat oblitera- tion between the mass and left descending colon (arrows).
E. Postcontrast coronal reformatted CT scan shows irregular enhancing solid areas with calcifications in the lower portion of marked hydrone- phrotic left kidney (arrows).
F. Photomicrograph of specimen shows immature neoplastic osteoids and sarcomatous stroma (H&E, × 100).
E B
D A
F C
Primary Renal Osteosarcoma Presenting as Hydronephrotic Kidney
134
J Korean Soc Radiol 2014;71(3):132-135 jksronline.orgto a pleuriopotent mesenchyme, that can differentiate into os- teoblasts (5, 8). The typical microscopic findings are pleomor- phic spindle cell and multinucleate giant tumor cell with diffuse calcified osteoids (5).
Various treatment approaches including radical nephrectomy, partial or total resection of contiguous organs, radiation therapy, and polychemotherapy have been pursued, but due to osteosar- coma’s aggressiveness and usually advanced stage at diagnosis, the prognosis characteristically is poor (4, 5).
In our case, we initially thought that it had arisen from the hy- dronephrotic kidney due to the mass’s aggressive imaging feature with hydronephrosis. Considering the prevalence of the renal mass, it could have been mistaken for a transitional cell carcino- ma with UPJ stricture or a renal cell carcinoma with sarcomatoid change.
Unlike other previously reported primary renal osteosarco- mas, the enhancing solid portions that were proven to be osteo- sarcomatous foci were located centrally rather than in the pe- ripheral portion adjacent to the renal capsule. Additionally, the upper portion of the markedly hydronephrotic kidney showed no tumor infiltration. The left ureter could not be identified in the surgical field grossly or as a pathologic specimen.
In summary, we have presented a pathologically confirmed case of primary renal osteosarcoma presenting as hydronephrot- ic kidney depicted on CT imaging. Primary renal osteosarcoma could be differentially diagnosed in the case of a tumor arising from a hydronephrotic kidney associated with calcifications, al- though a primary renal osteosarcoma is a rare disease.
REFERENCES
1. Lopez-Beltran A, Montironi R, Carazo JL, Vidal A, Cheng L.
Primary renal osteosarcoma. Am J Clin Pathol 2014;141:
747-752
2. Mortensen PH. Primary osteogenic sarcoma of the kidney.
Br J Urol 1989;63:101-102
3. Bollack C, Cinqualbre J, Warter A, Wenger JJ, Reinhardt W, Ziede E. Primary osteosarcoma of the kidney. Br J Urol 1982;54:435-436
4. Weingärtner K, Gerharz EW, Neumann K, Pflüger KH, Grüber M, Riedmiller H. Primary osteosarcoma of the kid- ney. Case report and review of literature. Eur Urol 1995;
of the kidney with marked hydronephrosis. Following surgery, the patient underwent no additional chemotherapy or radiation therapy. Just 7 weeks after surgery, multiple metastasis in the both lungs developed. The patient deteriorated over the course of several months and died 5 months after diagnosis of the pri- mary renal osteosarcoma.
DISCUSSION
Sarcomas originating from the kidney, the majority of which are leiomyosarcoma, account for only 1% of all primary renal malignancies. Metastasis from the primary skeletal osteosarco- ma to the kidney is found much more frequently than osteosar- coma originating from the kidney (4). According to the data, tu- mors occur more frequently in the sixth to seventh decades of life and the prevalence does not differ between males and fe- males (5).
The patient might complain of various, but non-specific symp- toms, including abdominal pain, flank pain, weakness, abdominal distension, weight loss, and, rarely, gross hematuria (4). Blood tests are often normal except for the serum level of alkaline phophatase, which may be normal or slightly altered.
Radiologically, demonstration of renal mass containing dense or rim-like calcification suggests the diagnosis of renal osteosar- coma. The sunburst appearance of calcifications within the renal contour, which can be detected on CT, seem to be a characteris- tic finding (6), but several other configurations also have been noted. Signs of space occupying lesions, such as pyonephrosis with permeative mass or organ displacement, might be seen on ultrasonography (7).
The differential diagnosis includes adult Wilm’s tumor, meta- static sarcoma, and sarcomatoid renal cell carcinoma.
On angiography, primary renal osteosarcoma has lesser vas- cularity than normal renal parenchyma. Renal cell carcinoma, by contrast, usually shows greater vascularity (7). Frequently, primary renal osteosarcoma shows a regional growth pattern with early infiltration of the renal capsule and adjacent struc- ture. It can metastasize to various organs such as the spleen, dia- phragm, liver, small and large bowel, bone marrow, dura, skin, and most commonly, the lung (4).
The etiology is uncertain, but it is thought to involve meta- plastic differentiation from connective tissue in the renal capsule
Jae Wook Lee, et al
135
jksronline.org J Korean Soc Radiol 2014;71(3):132-135
148
7. Puri T, Goyal S, Gupta R, Julka PK, Rath GK. Primary renal osteosarcoma with systemic dissemination. Saudi J Kidney Dis Transpl 2012;23:114-116
8. Tuttle RJ, Salama S, Matthews WR. Primary osteosarcoma of kidney with liposarcomatous elements. J Can Assoc Ra- diol 1985;36:76-78
28:81-84
5. Cioppa T, Marrelli D, Neri A, Malagnino V, Caruso S, Pinto E, et al. Primary osteosarcoma of the kidney with retro- peritoneal hemorrhage. Case report and review of the lit- erature. Tumori 2007;93:213-216
6. Zagoria RJ, Dyer RB. Computed tomography of primary renal osteosarcoma. J Comput Assist Tomogr 1991;15:146-
수신증으로 발현된 원발성 신장 골육종: 증례 보고1
이재욱
1· 구지혜
2· 김유미
1원발성 신장 골육종은 신장에 발생하는 아주 드문 종양이다. 일반적으로 중년 이후에 발생하는 것으로 알려져 있으며, 비 특이적인 증상인 복부통증, 체중감소, 복부 종괴 및 육안적 혈뇨를 보인다. 영상의학적으로는 기이한 신장 석회화가 이 질 환을 시사할 수 있는 소견으로 제시되고 있다. 우리는 76세 남성에서 수신증의 형태로 발현되었던 원발성 신장 골육종을 경험하였고, 이 환자는 근치적 신 절제술을 시행 받았으나 그 후 폐 전이가 발생하였다. 원발성 신장 골육종이 전산화단층 촬영에서 수신증의 형태로 나타난 경우는 아직까지 보고된 적이 없으며, 이에 증례 보고를 하고자 한다.
단국대학교 의과대학 단국대학교병원 1영상의학과, 2병리과