pISSN 2288-9272 eISSN 2383-8493 J Oral Med Pain 2019;44(4):174-178 https://doi.org/10.14476/jomp.2019.44.4.174
Non-Odontogenic Toothache Caused by the Fungal Ball of Maxillary Sinus: Case Reports
Ji-Woo Ha
1, Won Jung
2, Kyung-Eun Lee
2, Bong-Jik Suh
21
Department of Oral Medicine, School of Dentistry, Jeonbuk National University, Jeonju, Korea
2
Department of Oral Medicine, Institute of Oral Bioscience, School of Dentistry, Jeonbuk National University, Jeonju, Korea
Received November 23, 2019 Revised December 10, 2019 Accepted December 10, 2019
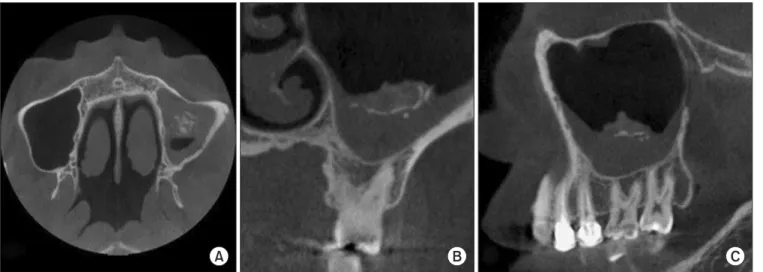
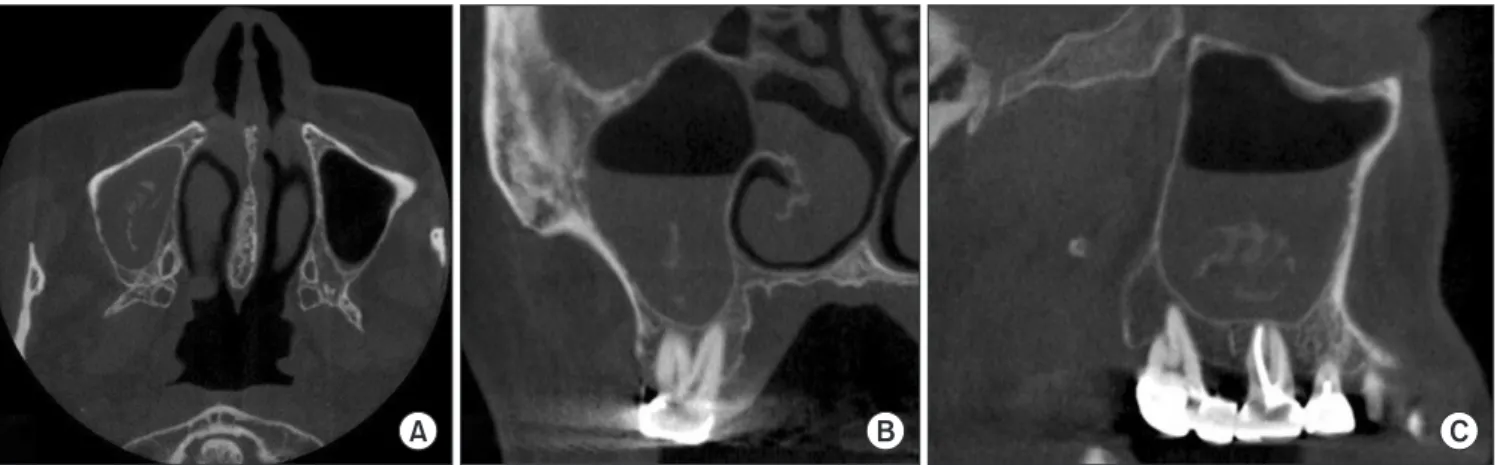
A fungal ball (FB) of the paranasal sinuses is a chronic, non-invasive fungal sinusitis defined as the accumulation of dense aggregation of fungal hyphae in a sinus cavity. A patient with FB infection in a sinus cavity has usually non-specific symptoms such as post-nasal drip, nasal congestion, headache. However, facial pain and toothache can be developed if FB infection is in maxillary sinus. The aim of this case report is to present two cases of FB of the maxillary sinus which caused toothache in the upper molar region. It is also to make dental practitioners consider the non-odontogenic origins of toothache and to pay special attention to avoid unnecessary dental treatment.
Key Words: Chronic sinusitis; Fungal ball; Non-odontogenic toothache
Correspondence to:
Bong-Jik Suh
Department of Oral Medicine, School of Dentistry, Jeonbuk National University, 567 Baekje-daero, Deokjin-gu, Jeonju 54896, Korea
Tel: +82-63-250-2060 Fax: +82-63-250-2058 E-mail: [email protected]
https://orcid.org/0000-0002-1817-4645
JOMP
Journal of Oral Medicine and PainCopyright
Ⓒ2019 Korean Academy of Orofacial Pain and Oral Medicine. All rights reserved.
CC