Corresponding author: Lee, Jia https://orcid.org/0000-0002-1483-0633
College of Nursing Science, Kyung Hee University, 26 Kyungheedae-ro, Dongdaemun-gu, Seoul 02447, Korea.
Tel: +82-2-961-0894, Fax: +82-2-961-9398, E-mail: [email protected] Received: Mar 29, 2020 / Revised: May 15, 2020 / Accepted: May 24, 2020
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ORIGINAL ARTICLE Open Access
Factors Associated with Mortality of Older Adults Hospitalized via Emergency Departments in Korea
Lim, Jungeun1 · Lee, Jia2
1Graduate Student, Graduate School, Kyung Hee University, Seoul, Korea
2Professor, College of Nursing Science, Kyung Hee University, Seoul, Korea
Purpose: As the rate of older people visiting Emergency Departments (EDs) increases, nurses are responsible for identifying patients at risk of poor outcomes and providing preventive interventions. The aim of this study was to identify the factors associated with the mortality of older adults hospitalized through EDs. Methods: The study design was a retrospective correlational design using the electronic medical records from a tertiary hospital in Korea. Data were collected from January 3 to March 6, 2016 through the hospital information center based on elderly patients admitted from January 1, 2011 to August 31, 2015. The study variables included general and admission character- stics, disease characteristics, and mortality of older patients visiting EDs. Results: Of the 9,896 patients, the mortality rate was 7.4%; highest in patients aged over 86 years, men, or those hospitalized from nursing homes.
Older adults arriving by private ambulance were 2.36 times more likely to die than walk-ins, and 1.38 times more likely for those using the 119 government emergency ambulance. Older patients hospitalized for more than four weeks were 2.17 times more likely to die than those hospitalized for less than a week. Conclusion: Based on the study findings ward nurses will be able to early detect older patients at risk of poor outcomes and make better clinical decisions to improve the quality of nursing care. Nurses can propose health policies such as stricter management of the private ambulance service and considering the most efficient length of hospital stay for older adults hospitalized through EDs.
Key Words: Aged; Emergency service; Hospitals; Mortality
INTRODUCTION
The population aged 60 years or over numbered 962 million worldwide in 2017, more than twice as large as it was in 1980, and the number of older persons is expected to double again by 2050 [1]. The increasing rate of older population in Korea is the fastest in the world from 6.0% in 2005 to 14.9% in 2019, and expected to reach 39.8% in 2050 [1,2]. As health issues such as chronic illness management, falls, and sudden crises have been on the rise in our aging society, the national long-term care insurance system was implemented in 2008 [3]. However, the visiting rate of old- er adults to Emergency Departments (EDs) has risen from 15.2% in 2005 [4] to 23.9% in 2016 [5]. In Australia, 22.0% of
emergency medical center users were older adults [6] while the United States had an increase of 23.3% in 2016 [7].
Approximately 90.0% of older adults have at least one chronic disease, and 51.0% have more than three [8]. More- over, the severity of disease process in older adults is rela- tively higher than that in the younger population, and their symptom characteristics are atypical, so it is not easy to identify which disease has caused the symptoms, result- ing in more complicated tests being required [9,10]. These matters result in longer stays in hospital for older patients, leading to physical and psychological hardship and poor outcomes [11]. In fact, the current in-hospital mortality rate of older patients admitted through EDs is high, ranging between 5.1% and 18.4% in Korea [12,13] and 8.9% to 11.4%
in other countries [14,15]. In-hospital overall mortality in elderly patients also varies by disease from 3.0% to 11.6%
[16,17]. Although the mortality rate of hospitalized elders in Korea does not differ much from that of Western coun- tries, the factors affecting mortality will be different be- cause the lifestyle and the health care delivery system differ.
Therefore, it is necessary to investigate the character- istics of older patients who have been hospitalized through EDs and experienced worse outcomes. Among previous studies in Korea, most have focused on specific popula- tions such as suicide attempts [18], homeless older adults [19], and older patients with trauma, [20] or clinical test re- sults related to mortality in EDs [21] rather than their pro- gnostic or disease characteristics. As elderly people are ad- mitted to hospitals through EDs due to chronic illness management or sudden accidents, and show a high mor- tality rate and medical expenses compared to younger adult patients [20,22], it is necessary to study the relation- ships between the characteristics of older patients and mortality to improve their health outcomes. Based on the literature review of previous studies on the mortality or characteristics of elderly patients in EDs, mortality-related variables were identified as 1) general characteristics of gender [14,23], age [24], and health insurance [25]; 2) ad- mission characteristics of admission process [25]; mode of arrival [9], level of consciousness [25,26], and emergency severity [9,14]; and 3) disease characteristics of main symp- tom [23,25], main diagnosis [14], treatment department [26], admission unit [26], and length of hospital stay [14].
Because older adults tend to find it difficult to communi- cate their problems directly and consider the economic sit- uation of their family more than they actively participate in their own clinical decision-making [27], ward nurses’
early identification of risk factors and appropriate respon- ses may have a positive impact on the outcome of medical treatment.
Therefore, this study was conducted to investigate the relationships between the mortality of older patients hos- pitalized via EDs and their influencing characteristics, in order to make better clinical decisions and improve the quality of nursing services.
1. Objectives
The aim of this study was to identify factors that are as- sociated with the mortality of older adults who have been hospitalized via EDs, by their general, admission, and dis- ease characteristics.
METHODS
1. Research DesignThe study used a retrospective correlational design to investigate the factors associated with the mortality of old- er patients by analyzing their general, admission, and dis- ease characteristics based on Electronic Medical Records (EMRs).
2. Study Participants
This study included the EMRs of 9,896 elderly patients who were hospitalized through the ED of a tertiary hospi- tal in Korea from January 1, 2011 to August 31, 2015. Inclu- sion criteria were patients aged 65 years or older, patients hospitalized through the ED, and patients alive before hospitalization. Older adults who were repeatedly hospi- talized were excluded to prevent the results from being af- fected by selection bias as most were cancer patients un- dergoing chemotherapy. The detailed number of patients of the accessible population was not provided by the hos- pital information center due to hospital management is- sues. The ED, which was the study site, has more than six- ty beds and around 180 patients visit daily. The post hoc power of this study was 98.9% with a total of 9,896 in the sample size.
3. Measurements
1) Admission characteristics
Admission characteristics included admission process, mode of arrival, level of consciousness, and emergency se- verity. The admission process was divided into admission from home, transfer from other hospitals or nursing homes, and admission through the outpatient department. The mode of arrival included walk-ins (own car), 119 govern- ment emergency ambulance, and private ambulance. The level of consciousness was classified into the following categories: alertness, lethargy, stupor, and unconscious- ness based on the medical records.
The emergency severity was measured by the modified version of the Emergency Severity Index (mESI) account- ing for the medical situation in Korea [28,29]. The tool clas- sifies the severity into five levels depending on the pa- tient's symptoms, vital signs, and the number of emer- gency medical resources needed. The severity of mESI is classified as 1=urgent (if there is an imminent threat to life and immediate intubation or cardiopulmonary resusci- tation is needed), 2=emergent (if resuscitation is not im-
mediately required but there is urgent need of interven- tion to improve vitality), 3=moderate-emergent (if many additional medical resources are required), 4=non-emer- gent (if only one additional medical resource is required), and 5=stable (if there is no additional health care expen- diture). The weighted kappa value of the mESI was 0.70 in the reliability evaluation between the physician and nurse groups [28].
2) Disease characteristics
Disease characteristics consisted of main symptom, main diagnosis, treatment department, admission unit, length of hospital stay, and medical outcome. The main symptom was measured by 14 items based on the Enforcement Re- gulation of Emergency Medical Service Act Article 2 no. 1 [30] and classified by legal criteria based on urgency of symptoms including eight acute symptoms: a. acute al- tered mental status, b. acute cardiopulmonary disorder, c.
acute metabolic disorder and poisoning, d. surgical emer- gency condition or serious burns, e. acute hemorrhage, f.
ophthalmological emergency symptom, g. allergy, and h.
psychiatric emergency symptom; and six subacute symp- toms: i. subacute mental change, j. subacute cardiopulmo- nary disorder, k. subacute surgical disorder and fracture, l.
subacute hemorrhage, m. childbirth or genderual abuse, and n. choking.
The main diagnosis was measured by 17 items from the 7th Korean Standard Disease Sign Classification List [31], and the contents were as below: a. Infectious or parasitic disease, b. neoplasms, c. blood-forming or immune mech- anism, d. endocrine, nutritional, and metabolic diseases, e.
mental and behavioral disorders, f. neurological diseases, g. ophthalmological diseases, h. circulatory diseases, i. res- piratory diseases, j. gastrointestinal diseases, k. skin dis- eases, l. musculoskeletal diseases, m. genitourinary dis- eases, n. congenital malformations, o. abnormal clinical and laboratory findings, p. injury or poisoning, and q. fac- tors influencing health status.
The length of hospital stay was the number of days from the date of admission to ED to the day of discharge from hospital. The medical outcome was the results of the medi- cal treatment which were divided into discharge and death based on the outcome records of the hospital discharge summary.
3) General characteristics
General characteristics included gender, age, and type of insurance. The types of insurance were national health insurance, medical aid, and private insurance.
4. Data Collection
First, we requested data which met the selection criteria from the hospital information center. The information cen- ter provided a data set collected from the EMRs of 9,896 older adults hospitalized through ED. The data set included the general and admission characteristics of the partic- ipants based on the nursing information records, and the disease characteristics and death and discharge informa- tion based on the initial medical record and discharge sum- mary.
5. Ethical Consideration
The study was approved by the Institutional Review Board (IRB) of the study hospital (IRB approval number SMC2015-08-083-001) before data collection. The study identification number was used for the participants’ medi- cal records for anonymity. All data were managed by as- signed research codes so that personal health information could not be identified. Each database group (general, ad- mission, and disease characteristics databases, and death and discharge database) was stored separately so that the personal information could not be traced. The collected data were used only for research purposes.
6. Data Analysis
Data were analyzed using SPSS for Windows version 22.0 (IBM Corp., Armonk, NY, USA). A Chi-squared test was used for the comparison of mortality and discharge rates according to general, admission, and disease charac- teristics of older adults hospitalized through ED. Factors associated with mortality of older patients were analyzed using logistic regression analysis. The model fit of the pre- diction model was assessed by performing a Hosmer-Le- meshow goodness-of-fit test. Effect size was measured us- ing the Nagelkerke R2.
RESULTS
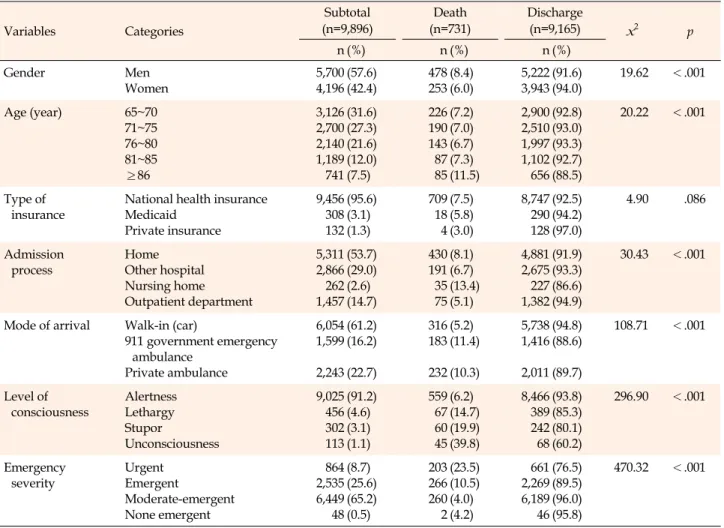
1. Mortality According to Patient Characteristics Of the 9,896 older adults hospitalized through ED, 731 (7.4%) died. The mortality rate was higher in men (x2= 19.62, p<.001) and in those aged 86 years or older (x2= 20.22, p<.001). Most patients (95.6%) had national health insurance (x2=4.90, p=.086), and there was no difference in mortality according to the type of insurance (Table 1).
In the admission characteristics, the mortality rate was
Table 1. Mortality and Discharge Rates by General and Admission Characteristics (N=9,896)
Variables Categories
Subtotal (n=9,896)
Death (n=731)
Discharge
(n=9,165) x2 p
n (%) n (%) n (%)
Gender Men
Women
5,700 4,196
(57.6) (42.4)
478 253
(8.4) (6.0)
5,222 3,943
(91.6) (94.0)
19.62 <.001
Age (year) 65~70
71~75 76~80 81~85
≥86
3,126 2,700 2,140 1,189 741
(31.6) (27.3) (21.6) (12.0) (7.5)
226 190 143 87 85
(7.2) (7.0) (6.7) (7.3) (11.5)
2,900 2,510 1,997 1,102 656
(92.8) (93.0) (93.3) (92.7) (88.5)
20.22 <.001
Type of insurance
National health insurance Medicaid
Private insurance
9,456 308 132
(95.6) (3.1) (1.3)
709 18 4
(7.5) (5.8) (3.0)
8,747 290 128
(92.5) (94.2) (97.0)
4.90 .086
Admission
process Home
Other hospital Nursing home Outpatient department
5,311 2,866 262 1,457
(53.7) (29.0) (2.6) (14.7)
430 191 35 75
(8.1) (6.7) (13.4) (5.1)
4,881 2,675 227 1,382
(91.9) (93.3) (86.6) (94.9)
30.43 <.001
Mode of arrival Walk-in (car)
911 government emergency ambulance
Private ambulance
6,054 1,599 2,243
(61.2) (16.2) (22.7)
316 183 232
(5.2) (11.4) (10.3)
5,738 1,416 2,011
(94.8) (88.6) (89.7)
108.71 <.001
Level of
consciousness Alertness Lethargy Stupor
Unconsciousness
9,025 456 302 113
(91.2) (4.6) (3.1) (1.1)
559 67 60 45
(6.2) (14.7) (19.9) (39.8)
8,466 389 242 68
(93.8) (85.3) (80.1) (60.2)
296.90 <.001
Emergency
severity Urgent
Emergent
Moderate-emergent None emergent
864 2,535 6,449 48
(8.7) (25.6) (65.2) (0.5)
203 266 260 2
(23.5) (10.5) (4.0) (4.2)
661 2,269 6,189 46
(76.5) (89.5) (96.0) (95.8)
470.32 <.001
higher for those admitted from a nursing home (x2=30.43, p<.001), using the emergency transportation systems (x2=108.71, p<.001), unconscious state (x2=296.90, p<.001), and urgent status (x2=470.32, p<.001) at admission (Table 1). In the disease characteristics, subacute surgical dis- order and fracture (27.4%) was the most frequent of the main symptoms, followed by acute cardiopulmonary dis- order (25.1%) while neoplasm (27.9%) was the most fre- quent in main diagnoses, followed by circulatory disease (26.2%). The mortality rate was higher in patients with car- diopulmonary symptoms of the main symptoms (x2= 160.41, p<.001), neoplasm of the main diagnosis (x2= 234.76, p<.001), internal medicine of the treatment depart- ment (x2=148.80, p<.001), intensive care unit of the admis- sion unit (x2=238.72, p<.001), and a hospital stay of more than two weeks (x2=120.42, p<.001) (Figure 1).
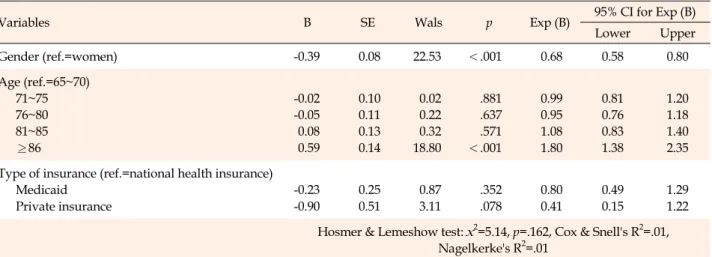
2. Factors Associated with Mortality of Older Patients Variables that were found to cause significant differ-
ences or have a significant correlation with mortality of older patients were selected as independent variables in the logistic model. Logistic regression analysis was used to examine the factors associated with mortality of older pati- ents. The Hosmer-Lemeshow test for general characteristic factors model, which included gender, age, and type of in- surance, revealed a good fit (x2=5.14, p=.162). The Nagel- kerke2 effect size was .01. Of the general characteristics, the mortality of older patients was 0.68 times lower in women than men (B=-0.39, p<.001). Patients aged 86 years or older were 1.80 times more likely to die than those aged 65~70 years (B=0.59, p<.001)(Table 2).
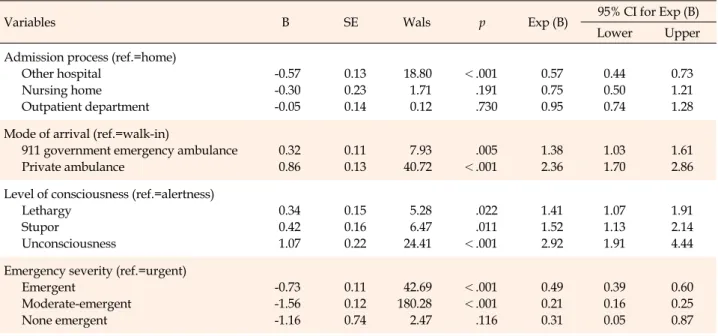
In the admission characteristic factors model, which in- cluded admission process, mode of arrival, level of con- sciousness, and emergency severity, the Hosmer-Leme- show test also revealed a good fit (x2=4.31, p=.229), and the Nagelkerke2 effect size was .12. Among the admission characteristics, patients arriving from other hospitals were 0.57 times less likely to die than those from home (B=-0.57, p<.001). Patients who arrived by private ambulance were
Figure 1. Mortality and hospital discharge rate by disease characteristics.
Table 2. General Characteristic Factors Associated with Mortality in Older Patients (N=9,896)
Variables B SE Wals p Exp (B) 95% CI for Exp (B)
Lower Upper
Gender (ref.=women) -0.39 0.08 22.53 <.001 0.68 0.58 0.80
Age (ref.=65~70) 71~75 76~80 81~85
≥86
-0.02 -0.05 0.08 0.59
0.10 0.11 0.13 0.14
0.02 0.22 0.32 18.80
.881 .637 .571
<.001
0.99 0.95 1.08 1.80
0.81 0.76 0.83 1.38
1.20 1.18 1.40 2.35 Type of insurance (ref.=national health insurance)
Medicaid Private insurance
-0.23 -0.90
0.25 0.51
0.87 3.11
.352 .078
0.80 0.41
0.49 0.15
1.29 1.22 Hosmer & Lemeshow test: x2=5.14, p=.162, Cox & Snell's R2=.01,
Nagelkerke's R2=.01
B=unstandardized beta; CI=confidence interval; Exp (B)=exponentiation of the B coefficient; ref.=reference group; SE=standard error.
2.36 times more likely to die than walk-ins (B=0.86, p<
.001), while those who arrived via the 119 government emergency ambulance were 1.38 times more likely to die (B=0.32, p=.005). Patients in an unconscious state at ad-
mission were 2.92 times more likely to die than those who were alert (B=1.07, p<.001), while those in stupor were 1.52 times (B=0.42, p=.011) and those in lethargy were 1.41 times (B=0.34, p=.022) more likely to die. Patients in an
Table 3. Admission Characteristic Factors Associated with Mortality in Older Patients (N=9,896)
Variables B SE Wals p Exp (B) 95% CI for Exp (B)
Lower Upper
Admission process (ref.=home) Other hospital
Nursing home Outpatient department
-0.57 -0.30 -0.05
0.13 0.23 0.14
18.80 1.71 0.12
<.001 .191 .730
0.57 0.75 0.95
0.44 0.50 0.74
0.73 1.21 1.28 Mode of arrival (ref.=walk-in)
911 government emergency ambulance Private ambulance
0.32 0.86
0.11 0.13
7.93 40.72
.005
<.001
1.38 2.36
1.03 1.70
1.61 2.86 Level of consciousness (ref.=alertness)
Lethargy Stupor
Unconsciousness
0.34 0.42 1.07
0.15 0.16 0.22
5.28 6.47 24.41
.022 .011
<.001
1.41 1.52 2.92
1.07 1.13 1.91
1.91 2.14 4.44 Emergency severity (ref.=urgent)
Emergent
Moderate-emergent None emergent
-0.73 -1.56 -1.16
0.11 0.12 0.74
42.69 180.28 2.47
<.001
<.001 .116
0.49 0.21 0.31
0.39 0.16 0.05
0.60 0.25 0.87 Hosmer & Lemeshow test: x2=4.31, p=.229, Cox & Snell's R2=.05,
Nagelkerke's R2=.12
B=unstandardized beta; CI=confidence interval; Exp (B)=exponentiation of the B coefficient; ref.=reference group; SE=standard error.
emergent status at admission were 0.49 times less likely to die than those in urgent state (B=-0.73, p<.001), while those in the moderate-emergent category were 0.21 times less likely to die (B=-1.56, p<.001)(Table 3).
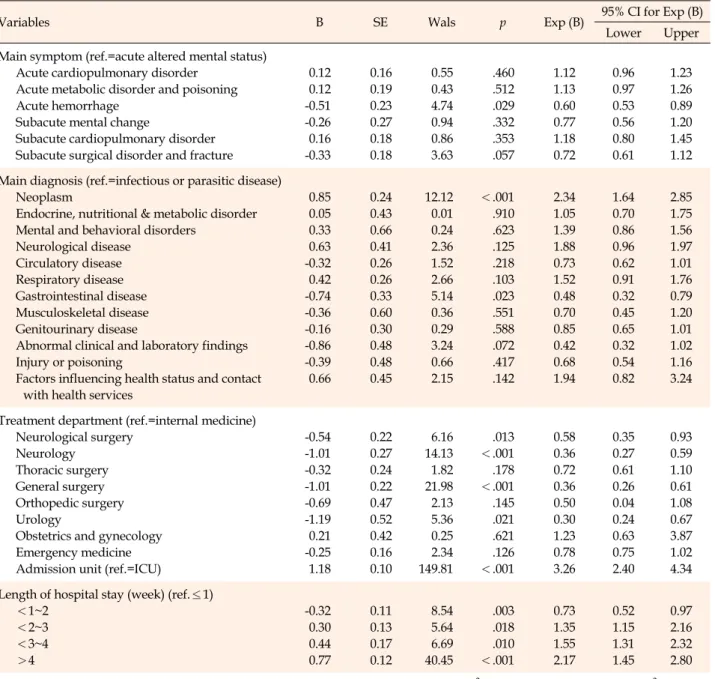
In the disease characteristic factors model, which in- cluded main symptom, main diagnosis, treatment depart- ment, admission unit, and length of hospital stay, although the Hosmer-Lemeshow test did not reveal a good fit (x2=26.10, p<.001), the sample size was sufficient [32] with 99.9% of post hoc power in this study. The Nagelkerke2 ef- fect size was .16. Older patients with a main symptom of acute hemorrhage were 0.60 times lower likely to die than those with acute altered mental status (B=-0.51, p=.029).
Patients with neoplasms as a main diagnosis were 2.34 times more likely to die than those with infectious diseases (B=0.85, p<.001), while those with gastrointestinal dis- eases were 0.48 times less likely to die (B=-0.74, p=.023).
Older patients treated from the department of internal medicine were more likely to die than those from neurol- ogy, general surgery, or urology. Patients admitted to the intensive care unit were 3.26 times more likely to die (B=
1.18, p<.001); patients hospitalized for more than four weeks were 2.17 times more likely to die than those hospi- talized for less than a week (B=0.77, p<.001), while those hospitalized for 3~4 weeks were 1.55 times higher (B=0.44, p=.010), and those for 2~3 weeks were 1.35 times higher (B=0.30, p=.018) (Table 4).
DISCUSSION
Identifying older adults at risk of poor outcomes as well as establishing preventive strategies for improving the quality of nursing care is important for those hospitalized through ED. The risk factors of their mortality identified in this study will help nurses predict changes in the con- dition of the elderly and plan preventive care.
In terms of the characteristics of the study participants, among the 9,896 older adults hospitalized through ED the most frequent main symptom was subacute surgical dis- order and fracture (27.4%) followed by acute cardiopul- monary disorder (25.1%). In a previous study approx- imately 28.7% of older adults reported falling at least once, and 37.5% of those who fell reported being hospitalized at least once [33]. Therefore, our study findings suggest that programs to prevent falls resulting in fractures for older adults are very urgent.
The highest risk factors from the general and admission characteristics in this study were men, the oldest, private ambulance use, unconscious state at admission, and ur- gent status of severity on admission. In a previous retro- spective study of older patients in ED, factors associated with mortality were highest for men, neoplasms, and am- bulance utilization [34]. In this study, the mortality of old- er patients arriving by private ambulance was the highest among the identified factors. In Korea, the total number of
Table 4. Disease Characteristic Factors Associated with Mortality in Older Patients (N=9,896)
Variables B SE Wals p Exp (B) 95% CI for Exp (B)
Lower Upper Main symptom (ref.=acute altered mental status)
Acute cardiopulmonary disorder Acute metabolic disorder and poisoning Acute hemorrhage
Subacute mental change
Subacute cardiopulmonary disorder Subacute surgical disorder and fracture
0.12 0.12 -0.51 -0.26 0.16 -0.33
0.16 0.19 0.23 0.27 0.18 0.18
0.55 0.43 4.74 0.94 0.86 3.63
.460 .512 .029 .332 .353 .057
1.12 1.13 0.60 0.77 1.18 0.72
0.96 0.97 0.53 0.56 0.80 0.61
1.23 1.26 0.89 1.20 1.45 1.12 Main diagnosis (ref.=infectious or parasitic disease)
Neoplasm
Endocrine, nutritional & metabolic disorder Mental and behavioral disorders
Neurological disease Circulatory disease Respiratory disease Gastrointestinal disease Musculoskeletal disease Genitourinary disease
Abnormal clinical and laboratory findings Injury or poisoning
Factors influencing health status and contact with health services
0.85 0.05 0.33 0.63 -0.32 0.42 -0.74 -0.36 -0.16 -0.86 -0.39 0.66
0.24 0.43 0.66 0.41 0.26 0.26 0.33 0.60 0.30 0.48 0.48 0.45
12.12 0.01 0.24 2.36 1.52 2.66 5.14 0.36 0.29 3.24 0.66 2.15
<.001 .910 .623 .125 .218 .103 .023 .551 .588 .072 .417 .142
2.34 1.05 1.39 1.88 0.73 1.52 0.48 0.70 0.85 0.42 0.68 1.94
1.64 0.70 0.86 0.96 0.62 0.91 0.32 0.45 0.65 0.32 0.54 0.82
2.85 1.75 1.56 1.97 1.01 1.76 0.79 1.20 1.01 1.02 1.16 3.24
Treatment department (ref.=internal medicine) Neurological surgery
Neurology Thoracic surgery General surgery Orthopedic surgery Urology
Obstetrics and gynecology Emergency medicine Admission unit (ref.=ICU)
-0.54 -1.01 -0.32 -1.01 -0.69 -1.19 0.21 -0.25 1.18
0.22 0.27 0.24 0.22 0.47 0.52 0.42 0.16 0.10
6.16 14.13 1.82 21.98 2.13 5.36 0.25 2.34 149.81
.013
<.001 .178
<.001 .145 .021 .621 .126
<.001
0.58 0.36 0.72 0.36 0.50 0.30 1.23 0.78 3.26
0.35 0.27 0.61 0.26 0.04 0.24 0.63 0.75 2.40
0.93 0.59 1.10 0.61 1.08 0.67 3.87 1.02 4.34 Length of hospital stay (week) (ref.≤1)
<1~2
<2~3
<3~4
>4
-0.32 0.30 0.44 0.77
0.11 0.13 0.17 0.12
8.54 5.64 6.69 40.45
.003 .018 .010
<.001
0.73 1.35 1.55 2.17
0.52 1.15 1.31 1.45
0.97 2.16 2.32 2.80 Hosmer & Lemeshow test: x2=26.10, p<.001, Cox & Snell's R2=.06
Nagelkerke's R2=.16
B=unstandardized beta; CI=confidence interval; Exp (B)=exponentiation of the B coefficient; ICU=intensive care unit; ref.=reference group;
SE=standard error.
119 government emergency systems was 1,384 with 9,103 trained staff while private ambulance services were 892 with 1,161 trained staff in 2017 [35]. Moreover, in the study of the emergency response abilities of ambulance staff from private ambulance services, the scores were low at 66.09 of 100 points in emergency treatment, 63.75 points in consciousness confirmation, 69.33 points in airway man- agement, 59.44 points in respiratory, and 64.00 points in circulation [36]. Based on current evidence, the emergency
care training programs for private ambulance employees need to be stricter to improve their emergency response capabilities and, for the safety of patients, legal control over the transfer of patients or expansion of the 119 gov- ernment emergency system should also be improved. It is also proposed that medical personnel accompany patients in private ambulances used for transfer to other hospitals.
The significant risk factors from the disease character- istics in this study were patients with acute altered mental
status, and those with neoplasms, affiliated to internal medicine, transferred to intensive care unit, and hospi- talized for more than four weeks. The average length of hospital stay across Organization for Economic Coopera- tion and Development (OECD) countries was around eight days, whereas Korea had the longest stays with over 16 days [37]. The reason for this may be that the national health insurance covered most medical costs. In this study 98.7% of older adults had national health insurance or Medicaid. In a study of older patients, increasing length of stay in Intensive Care Unit (ICU) is associated with higher mortality within a year for both mechanically ventilated and non-mechanically ventilated patients [38]. The evi- dence of the present study suggests that clinical deci- sion-making for older patients needs to consider the evi- dence that a longer stay in hospital with aggressive medi- cal treatment may not reduce their mortality rate. There- fore, it is recommended that the condition and quality of life of elderly patients is considered rather than continuing ICU treatment over a protracted period.
As nurses play an important role in patient assessment, it is necessary to accurately understand elderly patients and predict their prognosis in order to plan professional nursing services based on the study findings.
The study has several limitations. First, as there is a dif- ference in the severity of patients by the size and level of the ED, the results of the study may apply more to tertiary hospitals. For future study, hospitals of various sizes and locations should be included. Second, the study used ret- rospective data from EMRs which could not measure pro- spective changes in patients' outcomes by nursing inter- ventions that consider the risk factors of mortality. There- fore, we propose a prospective study of older patients hos- pitalized through ED for further studies. Nevertheless, this study contributed to the planning of strategies which will reduce the mortality rate of older adults by identify- ing the current problems in the emergency care system.
Third, as discharge included cases transferring to other hospitals such as long-term care or rehabilitation hospi- tals, those may have been relieved in an emergency status, but still treated. Finally, the study data was relatively old based on the current emergency care system, although the contents of training and transportation systems outlined in the Emergency Medical Service Act have not been changed for more than ten years.
CONCLUSION
The study findings provide important prognostic in- formation regarding the association between character-
istics of older patients hospitalized through EDs and their mortality. Among the general and admission character- istics, the mortality rate was the highest in men, older adults aged over 86 years, and those who arrived via pri- vate ambulance service. Among the disease character- istics, the mortality rate was greatest in older patients with neoplasms, and those who had been hospitalized for more than four weeks. Nurses are at the forefront of identifying changes in patients’ health conditions. Based on the results of this study, ward nurses will be able to identify older pa- tients at risk of poor outcomes and make better clinical de- cisions to improve the quality of nursing care. Nurses may use the study findings to develop tools to assess elderly patients admitted via ED and develop clinical protocols.
In addition, the results of the study suggest stricter man- agement of private emergency services, and future studies for the most efficient length of hospital stay for older pa- tients hospitalized through EDs.
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
AUTHORSHIP
Study conception and design acquisition - LJA; Data collection - LJE; Analyzing the data - LJE and LJA; Drafting and critical re- vision of the manuscript - LJE and LJA.
ACKNOWLEDGEMENT
This article is a revision of the first author's master's thesis from Kyung Hee University.
REFERENCES
1. United Nations, Department of Economic and Social Affairs, Population Division. World population ageing 2017. World Population Summary Report. New York: United Nations; 2017 December. Report No.: ST/ESA/SER.A/408.
2. Korean Statistical Information Service. Future population pro- jection [Internet]. Daejeon: Statistics Korea; 2019 [cited 2020 January 20]. Available from:
http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT _1BPA002&checkFlag=N
3. Long-term Care Insurance. Long-term care insurance system [Internet]. Wonju: National Health Insurance Service; 2018 [cited 2019 December 1]. Available from:
http://www.longtermcare.or.kr/npbs/e/e/100/htmlView?
pgmId=npee201m01s&desc=
4. Lee HM, Cho KH. Use of medical resources by the elderly pop- ulation in emergency department. Journal of Korean Geriatric Society. 2007;11(3):139-44.
5. National Emergency Medical Center. 2016 Annal of Emergency Medical Statistics. Annual Statistical Report. Seoul: National Emergency Medical Center; 2017 October. Report No.: 11-1352 000-001248-10.
6. Australian Institute of Health and Welfare. Emergency depart- ment care 2017-18: Australian hospital statistics. Annual Statistical Report. Canberra: Australian Institute of Health and Welfare; 2018 December. Report No.: HSE 216.
7. National Center for Health Statistics. Health, United States, 2017 [Internet]. Atlanta: Center for Disease Control and Prevention;
2017 [cited 2019 December 11]. Available from:
https://www.cdc.gov/nchs/hus/contents2017.htm#Figure_
013
8. Chung KH, Oh YH, Lee YK, Oh MA, Kang EN, Kim KR, et al.
2017 Survey for the elderly. Annual Survey Report. Sejong:
Korea Institute for Health and Social Affairs; 2017 November.
Report No.: 11-1352000-000672-12.
9. Oosterwold J, Sagel D, Berben S, Roodbol P, Broekhuis M. Fac- tors influencing the decision to convey or not to convey elderly people to the emergency department after emergency ambu- lance attendance: a systematic mixed studies review. BMJ Open. 2018;8(8):e021732.
https://doi.org/10.1136/bmjopen-2018-021732
10. Park E, Lee J. Symptom cluster in Korean patients with acute myocardial infarction. Journal of Korean Academy of Nursing.
2015;45(3):378-87.
https://doi.org/10.4040/jkan.2015.45.3.378
11. Hofman MR, van den Hanenberg F, Sierevelt IN, Tulner CR.
Elderly patients with an atypical presentation of illness in the emergency department. The Netherlands Journal of Medicine.
2017;75(6):241-6.
12. Kim SK, Park JH, Oh S, Park SH, Kim HJ, Kim SH, et al. Useful- ness of the neutrophil-to-lymphocyte ratio as a prognostic pre- dictor in elderly patients admitted to the intensive care unit through emergency department. Journal of the Korean Soci- ety of Emergency Medicine. 2019;30(6):555-62.
13. Kim I, Song H, Kim HJ, Park KM, Kim SH, Oh SH, et al. Use of the National Early Warning Score for predicting in-hospital mor- tality in older adults admitted to the emergency department.
Clinical and Experimental Emergency Medicine. 2020;7(1):61-6.
https://doi.org/10.15441/ceem.19.036
14. Brouns SHA, Wachelder JJ, Jonkers FS, Lambooij SL, Diele- man JP, Haak HR. Outcome of elderly emergency department patients hospitalised on weekends - a retrospective cohort study. EMC Emergency Medicine. 2018;18(9):1-7.
https://doi.org/10.1186/s12873-018-0160-y
15. Berthelot S, Lang ES, Quan H, Stelfox HT. Canadian in-hospi- tal mortality for patients with emergency-sensitive conditions:
a retrospective cohort study. BMC Emergency Medicine. 2019;
19(1):57. https://doi.org/10.1186/s12873-019-0270-1
16. Lorenzoni G, Swain S, Lanera C, Florin M, Baldi I, Iliceto S, et al. High- and low-inpatients' serum magnesium levels are as- sociated with in-hospital mortality in elderly patients: a ne- glected marker? Aging Clinical and Experimental Research.
2020;32(3):407-13.
https://doi.org/10.1007/s40520-019-01230-6
17. Groff H, Kheir MM, George J, Azboy I, Higuera CA, Parvizi J.
Causes of in-hospital mortality after hip fractures in the eld- erly. Hip International. 2020;30(2):204-9.
https://doi.org/10.1177/1120700019835160
18. Shin HW, Lee KJ, Kim H. The clinical characteristics of elderly suicide attempters visiting emergency room. Korean Journal of Psychosomatic Medicine. 2015;23(2):100-6.
19. Yoon CS, Choi H, Kim HB, Park SH, Park KH, Kwak MK.
Characteristics of emergency department visits in older home- less adults. Journal of The Korean Society of Emergency Medi- cine. 2015;26(1):128-32.
20. Seong YW, Sim MS, Lee TR, Hwang SY, Cha WC, Yoon H, et al.
A survey of emergency department health care provider on awareness of elder abuse. Journal of The Korean Society of Emergency Medicine. 2016;27(4):351-9.
21. Park J, Lee S. Mortality prediction of older adults admitted to the emergency department. Software and Data Engineering.
2018;7(7):275-80.
https://doi.org/10.3745/KTSDE.2018.7.7.275
22. Kim CH, Lee JS, Kwon MX, Lee CM, Kwon OY, Choi HS, et al.
A study for evaluation of the validity of mortality in emer- gency department sepsis score in geriatric patients with sepsis at the emergency department. Journal of The Korean Society of Emergency Medicine. 2012;23(4):500-9.
23. Godaert L, Godard-Sebillotte C, Allard Saint-Albin L, Bou- squet L, Bourdel-Marchasson I, Fanon JL, et al. Self-rated health as a predictor of mid-term and long-term mortality in older Afro-Caribbeans hospitalised via the emergency depart- ment. Quality of Life Research. 2018;27(1):91-6.
https://doi.org/10.1007/s11136-017-1693-3
24. Drame M, Jovenin N, Novella JL, Lang PO, Somme D, Laniece I, et al. Predicting early mortality among elderly patients hospitalised in medical wards via emergency department: the SAFES cohort study. The Journal of Nutrition, Health & Aging.
2008;12(8):599-604. https://doi.org/10.1007/bf02983207 25. Dhaussy G, Dramé M, Jolly D, Mahmoudi R, Barbe C, Kanaga-
ratnam L, et al. Is health-related quality of life an independent prognostic factor for 12-month mortality and nursing home placement among elderly patients hospitalized via the emer- gency department? Journal of the American Directors Asso- ciation. 2012;13(5):453-8.
https://doi.org/10.1016/j.jamda.2011.10.002
26. Kennedy M, Enander RA, Tadiri SP, Wolfe RE, Shapiro NI, Marcantonio ER. Delirium risk prediction, healthcare use and
mortality of elderly adults in the emergency department. Jour- nal of the American Geriatrics Society. 2014;62(3):462-9.
https://doi.org/10.1111/jgs.12692
27. Komeda H, Eguchi Y, Kusumi T, Kato Y, Narumoto J, Mimura M. Decision-making based on social conventional rules by eld- erly people. Frontiers in Psychology. 2018;9(1412):1-9.
https://doi.org/10.3389/fpsyg.2018.01412
28. Sim JR, Kim YH, Kim YO, Cho EH, Choi JR, Jun YH, et al.
Clinical validity comparison study of patients severity triage system in the emergency department; Modified Emergency Severity Index (mESI) and modified Canadian Triage Acuity System (mCTAS). Journal of The Korean Society Emergency Medicine. 2012;23(6):776-83.
29. Wuerz R, Milne LW, Eitel DR, Travers D, Gilboy N. Reliability and validity of a new five-level triage instrument. Academic Emergency Medicine. 2000;7(3):236-42.
https://doi.org/10.1111/j.1553-2712.2000.tb01066.x
30. National Law Information Center. Enforcement Regulation of Emergency Medical Service Act Article 2 no. 1: Emergency symptoms and related symptoms [Internet]. Sejong: Ministry of Health and Welfare; 2016 [cited 2019 December]. Available from:
http://www.law.go.kr/lsSc.do?tabMenuId=tab18&p1=&sub Menu=1&nwYn=1§ion=&tabNo=&query=%EC%9D%91
%EA%B8%89%EC%9D%98%EB%A3%8C%EC%97%90%20%
EA%B4%80%ED%95%9C%20%EB%B2%95%EB%A5%A0%2 0%EC%8B%9C%ED%96%89%EA%B7%9C%EC%B9%99#un defined
31. Korea Informative Classification of Disease. The 7th Korean Standard Disease Sign Classification List [Internet]. Seoul:
Korea Informative Classification of Disease; 2016 [cited 2019
December 10]. Available from:
http://www.koicd.kr/2016/kcd/v7.do#0&n
32. Yu W, Xu W, Zhu L. A modified Hosmer-Lemeshow test for large data sets. Communication in Statistics-Theory and Me- thods. 2017;46(23):11813-25.
https://doi.org/10.1080/03610926.2017.1285922
33. Bergen G, Stevens MR, Burns ER. Falls and fall injuries among adults aged ≥65 years-United States, 2014. MMWR Morbidity and Mortality Weekly Report. 2016;65(37):993-8.
https://doi.org/10.15585/mmwr.mm6537a2
34. Shen Y, Tay YC, Teo EWK, Liu N, Lam SW, Ong MEH. Asso- ciation between the elderly frequent attender to the emergency department and 30-day mortality: a retrospective study over 10 years. World Journal of Emergency Medicine. 2018;9(1):
20-5. https://doi.org/10.5847/wjem.j.1920-8642.2018.01.003 35. National Emergency Medical Center. 2017 Annual report on
the emergency medical statistics. Annual Statistical Report.
Sejong: Ministry of Health and Welfare; 2018 October. Report No.: 11-1352000-001248-10.
36. Kim ST, Lee YH, Shin DM. Convergence awareness of basic emergency treatment by private ambulance drivers. Journal of the Korea Convergence Society. 2017;8(8):127-36.
https://doi.org/10.15207/JKCS.2017.8.8.127
37. OECD. Health at a glance 2017: OECD indicators [Internet].
Paris: OECD Publishing; 2018. [cited 2019 December 10]. Avail- able from: https://doi.org/10.1787/health_glance-2017-en 38. Moitra VK, Guerra C, Linde-Zwirble WT, Wunsch H. Relation-
ship between ICU length of stay and long-term mortality for elderly ICU survivors. Critical Care Medicine. 2016;44(4):655- 62. https://doi.org/10.1097/CCM.0000000000001480