http://dx.doi.org/10.16956/kaes.2016.16.2.51
Endocrine Surgery
The Primary Thyroid Lymphoma Treated by Surgery without Chemotherapy: Two Cases Reports
Eun Hwa Park, Ji Hoon Kim, Jae Young Kwak, Cheon Soo Park, Jin Ho Kwak
Department of Surgery, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea
Primary thyroid lymphoma (PTL) is a relatively rare disease, accounting for less than 0.5∼
5% of all thyroid malignancies. We encountered two cases of a primary thyroid lymphoma with Hashimoto`s thyroiditis; one in a 63-year-old man and the other in a 79-year-old woman. The first case was a mucosa-associated lymphoid tissue lymphoma, and the other was a diffuse large B-cell lymphoma. Both patients underwent surgery and radiotherapy after being diagnosed using fine-needle aspiration cytology (FNAC). Both patients recovered well with no recurrence throughout the study period. The role of the surgeon in the treatment and diagnosis of thyroid lymphoma has been reduced due to the development of FNAC and combination therapy with chemotherapy and radiotherapy. On the other hand, surgery can be an effective treatment option for PTL confined to the thyroid, for achieving a definitive diagnosis, and in the treatment of patients with an airway obstruction.
Key Words: Thyroid gland, Lymphoma, Large B-Cell, Thyroidectomy
Received March 31, 2016, Revised May 30, 2016, Accepted June 3, 2016 Correspondence: Jin Ho Kwak
Department of Surgery, Gangneung Asan Hospital, University of Ulsan College of Medicine, 38, Bangdong-gil, Sacheon-myeon, Gangneung 25440, Korea
Tel: +82-33-610-3224 Fax: +82-33-641-8120 E-mail: [email protected]
Copyright © 2016 Korean Association of Thyroid and Endocrine Surgeons; KATES. All Rights Reserved.
cc This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Primary thyroid lymphoma (PTL) is a rare malignancy, accounting for 0.5% to 5% of all thyroid malignancy cases and 2.5% to 7% of all extranodal lymphoma cases.(1,2) In South Korea, with the increasing detection rate of papillary thyroid microcarcinoma, its prevalence has decreased to 0.1% of all thyroid malignancy cases.(1) It usually occurs among middle-aged to elderly women, with a peak incidence in women in their late sixties. The most common histological type of PTL is diffuse large B cell lymphoma (DLBCL), followed by mucosa-associated lymphoid tissue (MALT) lymphoma.(3) Hashimoto’s thyroiditis is associated with development of PTL. The relative risk of developing thyroid lymphoma in patients with Hashimoto`s thyroiditis has been reported to be 40 to 80 times greater than that in the general population.(4,5) Patients typically present with
a rapidly growing thyroid mass and may experience hoarseness, stridor, or, less commonly, dysphagia. The rate of thyroid enlargement tends to be more rapid in patients with PTL than in those with other thyroid malignancies, with the exception of anaplastic thyroid carcinoma.(2) The treatment of thyroid lymphoma remains controversial.
Initially, surgery was used extensively for the treatment of PTL. But surgery-alone was recently found to show limited effects. More recently, the combination therapy with radiotherapy and chemotherapy has been more frequently recommended. From the surgeon’s perspective, we report two cases of PTL treated with surgery.
CASE REPORTS
1. Case 1
A 63-year-old man visited our department because of a
Fig. 1. A 63-year-old man who was diagnosed with mucosa-associated lymphoid tissue (MALT) lymphoma. (A) Thyroid ultrasonography shows about 1.8×1.9×2.3 cm sized hypoehoic mass with ill-defined margin in right thyroid gland. (B) Thyroid fine needle aspiration cytology smear (Pap stain ×400) shows diffuse polymorphous lymphoid cells of medium sized cleaved, large round, and small round nuclei. (C) histopathology of thyroid (H&E, ×200). Lymphoid cells invade and expand the thyroid follicles, forming the lymphoepithelial lesion. The lymphoid cell have cleaved centrocyte-like nuclei or small round nuclei. (D) Immumo- histochemical stain show CD20+ and (E) bcl2+.
bilateral thyroid nodule that was incidentally discovered during his routine health examinations. No abnormalities were found in the patient’s medical and familial history. He complained of a recent aggravation of hoarseness and a palpable neck mass. On physical examination, he had a firm 2 cm mass was palpable on the right side of the thyroid gland. Thyroid function test was euthyroid status, thyro- globulin antibody and anti-microsomal Ab were both measured higher than normal range. Other laboratory results were within the normal limits. Thyroid ultrasono- graphy revealed two hypoechoic nodules; a right thyroid hypoechoic nodule about 1.8×1.9×2.3 cm in size and a left thyroid hypoechoic nodule 1.6×2.0×2.2 cm in size (Fig. 1A).
No lymphadenopathy was observed around the thyroid gland. According to the result of a fine needle aspiration biopsy, the left thyroid nodule was diagnosed chronic lymphocytic thyroiditis and the right thyroid nodule was diagnosed with suspicion of low-grade B-cell lymphoma (Fig. 1B). The result of two months follow-up cytology for right thyroid nodule was a possibility of lymphoma cannot be completely excluded. We determined the surgery for accurate histologic diagnosis. The patient underwent total
thyroidectomy. The surgical finding was a 2.5×2.0×2.0 cm ill-defined mass in the right lobe, adhesion to the sternothyroid muscle, but no lymphadenopathy was observed around the thyroid gland. In the histopatho- logical examination, the tumor was 2.5×2.1×2.0 cm in size, and the cut surface was solid and grayish white, with focal hemorrhage. A diagnosis of malignant lymphoma, MALT type with Hashimoto’s thyroiditis, was histopatholo- gically confirmed (Fig. 1C). Immunohistochemical staining indicated that the proliferating atypical lymphoid cells were positive for CD20 and bcl2 (Fig. 1D, E), but negative for CD3 and CD5. The Ki67 labeling index was 30%. Ann Arbor stage was IE, and the International Prognostic Index score was 1 (age). The patient underwent only external beam radiotherapy but did not receive chemotherapy. The total irradiation dose was 3,000 cGy during 20 times. He was followed up annually neck computer tomography and positron emission tomography every few years. He has developed no local recurrence or systemic metastasis for 114 months.
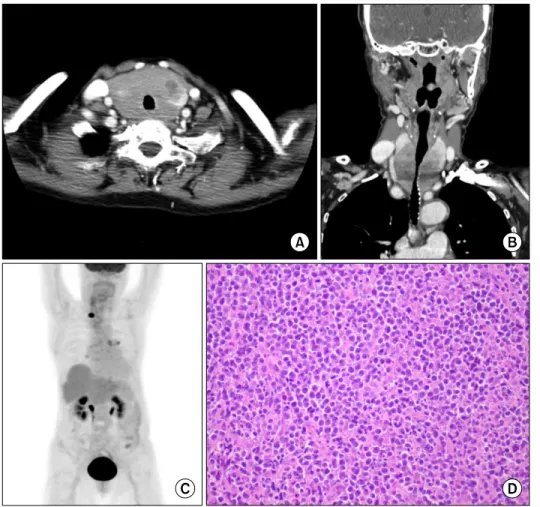
Fig. 2. A 79-year-old woman who was diagnosed with diffuse large B-cell lymphoma. (A) Preoperative CT scan shows a diffusedly enlarged thyroid gland with (B) narrowed tra- cheal diameter and extended to the thoracic inlet. (C) Pos- toperative positron emission tomography shows only a focal hyper-metabolic lesion in the right thyroid surgical bed. (D) Microscopically, there is a diffuse infiltration of large monomorphic lymphoid cells in the thyroid (H&E, ×200).
2. Case 2
A 79-year-old woman who had been previously healthy was referred to our institution with a palpable neck mass and respiratory discomfort. She complained of recent aggravation of dyspnea, odynophagia, and a palpable neck mass. She denied B symptoms (fever, night sweat and weight loss). On physical examination, a firm anterior neck mass about 10 cm in size was palpable and a wheezing sound was audible. The result of an initial thyroid function test indicated a euthyroid status, and the results of other laboratory examinations were non-specific, except a slightly elevated serum lactate dehydrogenase (LDH) level (230 U/L). The O2 saturation level in room air was 97%.
Computer tomography (CT) and ultrasonography revealed a 10×7 cm heterogeneous mass, which narrowed the tracheal diameter and even extended to the thoracic inlet (Fig. 2A, B). At first, we suspected anaplastic thyroid cancer and performed fine needle aspiration biopsy accordingly.
However, the result showed lymphocytic thyroiditis.
Unfortunately, her dyspnea rapidly worsened and respira- tory failure was imminent. We determined total thyroi- dectomy for the treatment of respiratory distress, and conventional surgical incision was performed. Both lobes of the thyroid were enlarged, and a soft, white tumor had replaced the normal thyroid tissue. Grossly, we observed extracapsular, recurrent laryngeal nerve, and tracheal invasion. Histopathological examination results confirmed DLBCL (Fig. 2D). Immunohistochemical staining results were positive for CD20, BCL-2, and BCL-6 but negative for CD 3, CD5, and CD 10. The Ki67 labeling index was 99%.
We performed a staging work up after the surgery.
Thereby, we determined the Ann Arbor stage as 1E and the International Prognostic Index score as 2 (age and LDH level). Positron emission tomography revealed only a focal hyper-metabolic lesion in the right thyroid surgical bed (Fig. 2C). Treatment of choice was combined radiation and chemotherapy, but the patient and her family refused chemotherapy because of her old age and general condition weakness. Sequential radiotherapy was recommended
after multidisciplinary discussions. A total irradiation dose of 5,040 cGy was administered in 28 equal fractions without any complications. She achieved complete remission at the 1 month and 13 month follow-up physical examination, and neck and chest CT scans every three months revealed no evidence of recurrence.
DISCUSSION
Primary thyroid lymphoma (PTL) is a rare malignancy.
However, the distinction of thyroid lymphoma from other thyroid malignancies, especially anaplastic thyroid carci- noma, is crucial in relation to management strategies. PTL is more common in women (3:1 predominance) between the age of 50 and 80 years, with a peak incidence in their late 60s.(3) Patients typically present with a rapidly growing thyroid mass and may experience hoarseness, stridor, or less commonly, dysphagia. The rate of thyroid enlargement tends to be more rapid in patients with PTL than in those with other thyroid malignancies, with the exception of anaplastic thyroid carcinoma.(2) Class B symptoms of fever, night sweat and weight loss are less common. Most patients are euthyroid.
Our cases had no B symptoms and euthyroid status.
PTL can be classified according to histological subtype.
The most common PTL subtypes are diffuse large B-cell lymphoma (DLBCL), marginal zone B-cell lymphoma of the mucosa-associated lymphoid tissue (MALT) lymphoma, and follicular lymphoma.(6) Hodgkin’s lymphoma, small lymphocytic lymphoma and T-cell lymphoma are relatively rare subtypes.(6) DLBCL is the most common subtype (70%) and most aggressive, with almost 60% of cases diagnosed with dissemination, whereas MALT lymphomas (6∼27%) have a relatively indolent course.(7) In some patients, DLBCL may arise from a preexisting MALT lymphoma, and a component of MALT lymphoma can be seen in one-third of thyroid DLBCL cases.(2)
PTL typically develops in patients with a background of Hashimoto’s thyroiditis. Because the normal thyroid gland has no native lymphoid tissue, thyroid lymphoma is thought to develop from lymphocytic tissue acquired during the course of chronic inflammation or an auto- immune process such as that in Hashimoto’s thyroiditis.(1)
It has been postulated that the chronic antigenic stimu- lation and proliferation of lymphoid tissue in Hashimoto’s thyroiditis created cells that are susceptible to neoplastic transformation, which lead to PTL.(1,2) The incidence of Hashimoto’s thyroiditis in patients with PTL has been reported in previous studies to be 27% to 100%. Hwang et al. reported that 57% of patients with PTL have clinical or histological evidence of Hashimoto’s thyroiditis.(1) Although MALT lymphoma were more frequently associated with Hashimoto’s thyroiditis, the incidence of Hashimoto’s thyroiditis did not significantly differ between DLBCL and MALT lymphoma. In terms of cellular immunophenotype, thyroid DLBCLs are CD20 positive, and most are B-cell lymphoma (Bcl)-6 positive. Approximately half are Bcl-2 positive, and most are negative for CD5, CD10, and CD23.(8) MALT lymphomas have an immunoglobulin light chain, and are CD20 and Bcl-2 positive, but are negative for CD5, CD10, and CD23.(2) In addition, the Ki-67 labeling index of the cell proliferation maker was measured to be 30% in MALT lymphoma and 99% in DLBCL, in our patients.
Fine needle aspiration cytology (FNAC) is an excellent diagnostic tool for thyroid disorders, as it is minimally invasive and can be performed in the clinic. Unfortunately, the FNAC test has a low reported accuracy for the diagnosis of PTL because of the pathological similarities between thyroid lymphoma and Hashimoto’s thyroiditis. In one report,(1) PTL was accurately diagnosed by using the FNAC test in only 59% of patients, who were later proven to have the malignancy. For both of our patients, the FNAC test result indicated lymphocytic thyroiditis. The lack of marked nuclear atypia in PTL makes the cytological differentiation between the lymphoid infiltrate of Hashimoto’s thyroiditis and lymphoma difficult.(1,9) Takano et al.(9) proposed a new diagnostic method to detect B-cell monoclonality that combines digestion with restriction enzymes and vecto- rette polymerase chain reaction for aspiration biopsy- nucleic acid diagnosis of thyroid malignant lymphoma.
Despite advances in FNAC testing and adjunctive techni- ques, differentiation of PTL from Hashimoto’s thyroiditis by using the FNAC test may be difficult, especially when the thyroid lymphoma is of a low-glade histology such as MALT lymphoma. Therefore, confirmatory procedures such
as tissue biopsy or surgery are strongly recommended when PTL is suspected in the FNAC test. Open surgical biopsy is still required in many cases, particularly when treatment strategies differ according to histological subtype (MALT vs.
diffuse or mixed large cell) or the diagnosis is still in question.
Ann Arbor stage classification is most widely used for PTL, with up to 90% of patients presenting with early stage disease.(3) Five year after diagnosis, disease-specific survival was 86% for stage IE (confined to the thyroid gland), 81% for stage IIE (confined to the thyroid gland and regional lymph node), and 64% for stage IIIE (involved the lymph nodes on both sides of the diaphragm)/IVE (systemic dissemination).(3) Fortunately, our patients had stage IE disease, In case 1 (MALT lymphoma) and Case 2 (DLBCLs), no recurrence was observed during 10 years and 13 months follow-up, respectively.
Appropriate treatment for patients with PTL depends on histological subtype, as the tumor grade and the efficacy of each treatment modality vary by subtype. The current treatment modalities for thyroid lymphoma include radio- therapy, chemotherapy, surgery, and combined chemo- radiotherapy.(2) The role of surgery in PTL is still contro- versial and its use for diagnosis and treatment has decreased over time. Graff-Baker et al.(3) reported that the use of surgery for PTL has declined from 81% of patients in 1973 to 1987 to 61% in 1997 to 2005 in the United States.
More recently, surgical removal has been shown to have a limited benefit. Meanwhile, non-surgical treatment, including chemotherapy and/or radiotherapy, depending on histological subtype, has become the mainstay of treatment in recent years.(6) However, surgery is generally used for palliation or diagnosis of thyroid lymphoma.
When the mass rapidly grows, compressive symptoms such as dysphagia, dyspnea, and pain can be managed with a prompt debulking surgery. A study by Sippel et al.(10) that included 27 patients with thyroid lymphoma and significant airway obstruction who underwent palliative surgery showed good long term result (overall 5-year survival, 77%) and low operative morbidity. Furthermore, surgery and/or radiotherapy improved the survival of patients with stage I and II MALT, DLBCL, and small lymphocytic histology.(3) In our cases, surgery was successful
and respiratory distress was improved after surgery. No postoperative complications such as nerve injury, bleeding, and permanent hypocalcemia, were observed.
In summary, FNAC and other current diagnostic tools, including flow cytometry and immunostaining, serve as first-line diagnostic tools for thyroid lymphoma. Since the development of FNAC and the use of radiotherapy and chemotherapy, the need for surgery has decreased. How- ever, there remains an important role for surgery in the management of thyroid lymphoma, especially for achiev- ing a definitive diagnosis when the FNAC test result is unclear, and in the treatment of patients with a rapidly growing mass and airway obstruction.
REFERENCES
1. Hwang YC, Kim TY, Kim WB, Shong YK, Yi KH, Shong M, et al.
Clinical characteristics of primary thyroid lymphoma in Koreans. Endocr J 2009;56:399-405.
2. Graff-Baker A, Sosa JA, Roman SA. Primary thyroid lymphoma:
a review of recent developments in diagnosis and histol- ogy-driven treatment. Curr Opin Oncol 2010;22:17-22.
3. Graff-Baker A, Roman SA, Thomas DC, Udelsman R, Sosa JA.
Prognosis of primary thyroid lymphoma: demographic, clinical, and pathologic predictors of survival in 1,408 cases. Surgery 2009;146:1105-15.
4. Holm LE, Blomgren H, Löwhagen T. Cancer risks in patients with chronic lymphocytic thyroiditis. N Engl J Med 1985;312:
601-4.
5. Matsuzuka F, Miyauchi A, Katayama S, Narabayashi I, Ikeda H, Kuma K, et al. Clinical aspects of primary thyroid lymphoma:
diagnosis and treatment based on our experience of 119 cases.
Thyroid 1993;3:93-9.
6. Sarinah B, Hisham AN. Primary lymphoma of the thyroid: diag- nostic and therapeutic considerations. Asian J Surg 2010;33:
20-4.
7. Yeshvanth SK, Lakshminarayana KP, Upadhyaya VS, Shetty JK.
Primary thyroid lymphoma arising from Hashimotos thyroiditis diagnosed by fine needle aspiration cytology. J Cancer Res Ther 2012;8:159-61.
8. Niitsu N, Okamoto M, Nakamura N, Nakamine H, Bessho M, Hirano M. Clinicopathologic correlations of stage IE/IIE pri- mary thyroid diffuse large B-cell lymphoma. Ann Oncol 2007;18:1203-8.
9. Takano T, Asahi S, Matsuzuka F, Hidaka Y, Yoshida H, Miyauchi A. Aspiration biopsy-nucleic acid diagnosis of thyroid malig- nant lymphoma by vectorette PCR: experience of eight cases.
Leuk Res 2008;32:151-4.
10. Sippel RS, Gauger PG, Angelos P, Thompson NW, Mack E, Chen H. Palliative thyroidectomy for malignant lymphoma of the thyroid. Ann Surg Oncol 2002;9:907-11.