— 112 — 대한고관절학회지제13권제2호
Vol. 13, No. 2, June, 2001
무시멘트형 비구컵을 이용한 재치환 성형술 (Cementless Acetabular Revision Arthroplasty)
박이상이원
고려대학교 의과대학 정형외과학교실
비구컵의 재치환 성형술은 가장 힘든 수술중의 하 나이다. 비 감염성 해리, 감염, 골용해 등 여러 원인 에 의해 야기된 비구컵 고정의 실패는 비구부의 변 형, 골결손, 불량한 골질등이 발생되어 골반의 해부 학적 구조의 이상을 초래하게 된다. 따라서 비구컵 의 재치환 성형술의 목적은 결손된 뼈를 복원시키고 고관절의 생역학적 구조를 유지시키며 비구컵의 안 정성을 얻는데 있다. 골시멘트를 이용한 비구컵 재 치환술은 2년에서 1 4년 추시 결과 1 0 %에서 6 0 %의 실패율로 불량한 결과가 보고되고 있다3 , 9 , 1 2 , 1 5 ). Amstutz 등1 )은 시멘트형 비구컵의 재치환술시 2년 에 1 0 %의 실패율을, Sloof 등1 8 )은 5년에 1 1 . 4 %의 실패율을 보고하였다. 또한 threaded cup과 같은
무시멘트 비구컵 재치환술 역시 불량한 결과가 보고 되고 있다1 3 ). 그러나 미세포말형 무시멘트 비구컵의 재치환성형술의 단기 및 중장기 결과는 시멘트형 비 구컵 재치환술보다 더 좋다고 보고되고 있으며 따라 서 최근에는 무시멘트형 비구컵을 이용한 재치환 성 형술이 보편적으로 시행되고 있다6 , 7 , 1 0 , 1 1 , 1 3 , 1 7 ).
1. 적응증
・ 무시멘트형 비구컵의 재치환술의 기본적인 목 표는 최대한으로 건전한 숙주골(host bone)과 접촉 ( c o n t a c t )되도록 하여야 한다.
・ 따라서 비구골의 bone stock의 상태가 가장
※ 통신저자 : 박 상 원
서울특별시 성북구 안암동 5가 1 2 6 - 1 고려대학교 의과대학 정형외과학교실 Tel : 02)920-5323, Fax : 02)924-2471 E-mail : [email protected]
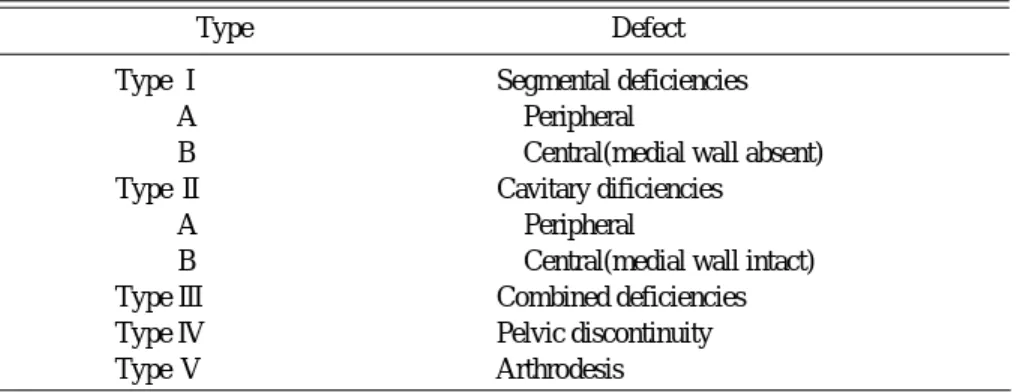
Table 1. The AAOS classification system for acetabular deficiencies
Type Defect
Type Ⅰ Segmental deficiencies
Type A Peripheral
Type B Central(medial wall absent)
Type Ⅱ Cavitary dificiencies
Type A Peripheral
Type B Central(medial wall intact)
Type Ⅲ Combined deficiencies
Type Ⅳ Pelvic discontinuity
Type Ⅴ Arthrodesis
중요하며 비구골 결손의 정확한 판정 이 필요하다.
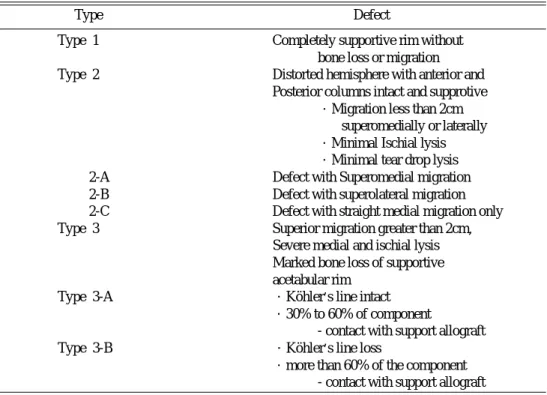
・ 비구골 결손의 분류는 A A O S에서 채택된 D’A n t o n i o의 분류4 , 5 ), Paprosky 분류 등1 4 )이 있다 (Table 1,2)
・ 무시멘트 비구컵과 접촉되는 건전한 숙주골의 범위에 대해서는 정확하게 알려져 있지는 않으나 골 동결손(cavitary defect)이 있는 경우는 건전한 숙 주골과 적어도 50% 이상 접촉되어야 하고 변연부 결손(segmental defect)이 있는 경우는 무시멘트 비구컵의 7 0 %는 숙주골로 피복되어야 한다2 , 8 , 1 4 , 1 6 , 1 9 ).
・ AAOS 분류에 의한 대부분의 공동결손( T y p e II), 변연부 결손(type I)의 일부및 혼합결손( t y p e I I )의 일부가 적응이 되며2 , 4 )
・ 또한, Paprosky분류에 의한 Type I과 Type II 가 무시멘트형 비구컵의 적응이 된다1 4 ).
・ 일반적인 무시멘트형 비구컵의 적응증은 시멘 트형 또는 무시멘트형 비구컵의 비 감염성 해리, 골 용해에 의한 비구컵 주위의 광범위한 비구골 결손, 비구컵의 불량 위치고정으로 인한 재탈구, 감염으로 인한 재치환술등이다1 3 ).
・ 무시멘트형 비구컵을 사용할 수 없는 경우는 비구컵의 50% 이상이 건전한 숙주골과 접촉을 얻을 수 없는 경우, 비구 상연부의 골 결손이 심한 경우, Köhler line이 파괴되어 비구골의 내측면의 손상이 심한 경우, 좌골의 골 용해가 진행되어 후주( p o s t . c o l u m n )의 손상이 있는 경우, pelvic discontinu- i t y가 있는 경우 등이다2 , 1 4 ).
2. 수술전 평가
수술전 평가의 궁극적인 목표는 비구골 결손의 정 도를 정확히 판정하는데 있다.
고관절부 A-P view, lateral view, oblique view(Judet view), computed tomography등이 이용된다. X-Ray사진은 선명해야 한다.
3. 수술수기
1) 수술 도달법
수술자의 선호도에 따라 다르나, 후외측 도달법이
— 113 —
무시멘트형 비구컵을 이용한 재치환 성형술
Table 2. The Paprosky’s classification for acetabular bone loss
Type Defect
Type 1 Completely supportive rim without
bone loss or migration Type 2 Distorted hemisphere with anterior and
Posterior columns intact and supprotive
・Migration less than 2cm superomedially or laterally
・Minimal Ischial lysis
・Minimal tear drop lysis Type 2-A Defect with Superomedial migration Type 2-B Defect with superolateral migration Type 2-C Defect with straight medial migration only
Type 3 Superior migration greater than 2cm,
Severe medial and ischial lysis Marked bone loss of supportive acetabular rim
Type 3-A ・Köhler’s line intact
・30% to 60% of component
- contact with support allograft
Type 3-B ・Köhler’s line loss
・more than 60% of the component - contact with support allograft
많이 이용된다.
2) 비구골의 상태 판정
・ 후주(posterior column)의 상태가 가장 중요 하며 비구골 후연의 결손은 무시멘 트형 비구컵 재 치환술 실패의 원인이 된다.
・ 비구골 상연부의 결손이 있는 경우에는 h i g h hip center 위치로 비구컵을 고정 하거나 b u l k g r a f t를 사용한다.
・ 무시멘트형 비구컵은 적어도 상연( d o m e )과 후 벽(posterior wall)에 고정시킬수 있어야 한다.
3) 비구부의 확공( r e a m i n g )
확공의 목적은 경화된 뼈를 갈아주는데 있다. 가 능한 한 후주 및 후연의 확공은 피하 는 것이 좋다.
4) 골이식
・ 골이식에는 자가골, 저온동결 동종골, 동결 건 조 동종골, 또는 혼합골등이 사용될 수 있으며 사용 되는 골의 종류는 크게 영향을 미치지 않는다
・ 골동결손에는 주로 분쇄 동종골이나 자가골을 사용하며 분절 결손에는 구조적 동종골 이식을 주로 시행한다.
・ 무시멘트 비구컵의 30% 이상이 구조적 자가골 또는 동종골(Bulk graft)로 이식 되면 실패율이 높 으므로 피해야 한다1 0 ).
・ 구조적 동종골로 이식한 경우는 숙주골과 동종골 접촉 경계부는 자가망상골로 이식을 해주는 것이 좋다.
5) 비구컵의 삽입
・ 비구컵의 삽입 위치는 일차적 비구컵의 삽입과 마찬가지로 4 0 ~ 5 0도 외전 및 2 0도 전경의 위치로 삽입한다.
・ 비구컵의 삽입 방법은 비구골의 골질의 상태, 골결손의 종류에 따라 압박 고정이나 선상 고정 방 법을 사용할 수 있으나 부가적으로 2 ~ 3개의 나사못 으로 고정해주는 것이 좋다.
6) 수술후 처치
수술후 체중부하는 비구컵 고정의 정도, 골이식의 종류에 따라 결정한다. 일반적으로 처음 6 ~ 8주간은
비체중부하 목발 보행을 시키고 전체중부하는 이식 골의 유합에 따라 결정되나 적어도 3개월 후에 허용 한다. 구조적 골이식을 시행한 경우는 적어도 3 ~ 6 개월간 2개의 목발을 이용한 보행을 행한다.
4. 무시멘트형 비구컵 재치환술의 결과
・ 무시멘트형 비구컵을 이용한 재치환술의 중장 기 결과는 시멘트형 비구컵을 이용한 재치환술에 비 해 만족스런 결과가 보고되고 있다1 0 , 1 1 , 1 3 , 1 7 ).
・ Lepold 등1 1 )은 HGP acetabular cup으로 재 치환술을 시행한 1 3 1명( 1 3 8례)에서 평균 1 0 . 5년 추 시결과 9 8 %의 생존율과 1 . 8 %의 비감염성 해리, 1 7 %의 골용해를 보고하였고, Lachiewicz와 P o o n1 0 )은 HGP acetabular cup으로 재치환술을 시행한 5 5명( 5 7례)에서 평균 7년 추시 결과 한례도 재치환술을 시행하지 않았다고 보고하였다.
・ 그러나 보다 더 장기간의 결과에 대한 관찰이 필요하며, 특히 골반골 용해의 발생 은 시간이 경과 함에 따라 증가되고 있으며 무시멘트 비구컵 재치환 술의 가장 큰 문제점으로 대두되고 있다1 1 , 1 3 ).
5. 결 론
무시멘트형 비구컵 재치환술이 성공하기 위해서는 비구컵은 적어도 7 0 %가 건전한 숙주골과 안정적인 접촉이 이루어져야 하고, 비구변연부 특히 후연과 상연부의 결손 범위가 중요하므로 수술전 또는 수술 시에 비구골 결손의 종류와 비구골 골질의 판정이 중요하다고 사료된다.
REFERENCES
11) Amstutz HC, Ma SM, Jinnah RH, Mai L : Revision of aseptic loose total hip arthroplasties.
Clin Orthop, 170 : 21-33, 1982.
12) Bal BS, Maurer T and Harris WH : Revision of the acetabular component without cement after a previous acetabular reconstruction with use of a bulk femoral head graft in patients who had con - genital dislocation or dysplasia. J Bone Joint Surg, 81-A:1703-1706, 1999.
13) Callaghan JJ, Salvati EA, Pellicci PM, Wilson
— 114 — 박김상김원
— 115 —
무시멘트형 비구컵을 이용한 재치환 성형술
PD, Ranawat CS : Results for revision for mechan - ical failure after cemented total hip replacement, 1979-1982. A two to five year follow up. J Bone Joint Surg, 67-A:1074-1085, 1985.
14) D’Antonio JA : Periprosthetic bone loss of the acetabulum. Classification and management.
Orthop Clin North Am, 23-2:279-290, 1992.
15) D’Antonio JA, Capello WN, Borden LS et al. : Classfication and management of acetabular abnormalities in total hip arthroplasty. Clin Orthop, 243:126-137, 1989.
16) Emerson Jr RH, Head WC, Berklacich FM, Malinin TL : Non-cemented acetabular rovision arthroplasty using allograft bone. Clin Orthop, 249:30-43, 1989.
17) Engh CA, Glassman AH, Griffin WL, Mayer JG : Results of cementless revision for failed cemented total hip arthroplasty. Clin Orthop, 235:91-110, 1988.
18) Gross AE : Revision arthroplasty of the acetabu - lum with restoration of bone stock. Clin Orthop, 369: 198-207, 1999.
19) Kavanaugh BF, Ilstrup DM, Fitzgerald RH : Revision of total hip arthroplasty. J Bone Joint Surg, 67-A:517-526, 1985.
10) Lachiewich PF and Poon ED : Revision of a total hip arthroplasty with a Harris-Galante prous coated acetabular component without cement. A follow up note on the results at five to twelve years. J Bone Joint Surg, 80-A :980-984, 1998.
11) Leopold SS, Rosenberg AG, Bhatt RD, Sheinkop MB, Quigley LR and Galante JO : C e m e n t l e s s acetabular revision. Evaluation at an average of
10.5years. Clin Orthop, 369:179-186, 1999.
12) Marti RK, Schuller HM, Besselaar PP, Vanfrank Hassnoot EL : Results of revision of hip arthroplasty with cement. A five to fourteen year follow up study.
J Bone Joint Surg, 72-A:346-354, 1990.
13) Padgett DE : Cementless acetabular reconstruction In : Callaghan JJ, Rosenberg AG and Rubash HE.
The Adult Hip. Vol II. Philadelphia, Lippincott- Raven Publishers. :1413-1424, 1998.
14) Paprosky WG and Magnus RE : Principles of bone grafting in revision total hip arthroplasty.
Acetabular technique. Clin Orthop, 298:147-155, 1994.
15) Schatzker J and Wong MK : Acetabular revision.
The role of rings and cages. Clin Orthop, 369:187- 197, 1999.
16) Schüller HM, Dalstra M, Huiskes R, Marti RK : Total hip reconstruction in acetabular dysplasia. A finite element study. J Bone Joint Surg, 75-B:464- 474, 1993.
17) Silverton C, Rosenberg AG, Sheinkop MB, Kull LR, Galante JO : Revision of acetabular compo - nent without cement after total hip arthroplasty. A follow up note regarding results at seven to eleven years. J Bone Joint Surg, 78-A:1366-1370, 1996.
18) Sloof TJJH, Buma P, Schreurs BW, Schimmel JW, Huiskes R, and Gardeniers J : A c e t a b u l a r and femoral reconstruction with impacted graft and cement. Clin Orthop, 324:108-115, 1996.
19) Wolfgang GL : Femoral head autografting with total hip arthropalsty for lateral acetabular dyspla - sia. A 12 year experience. Clin Orthop, 255:173- 185, 1990.