125
영서북부지역 복강경 담낭절제술 1,211예에 대한 임상적 고찰
한림대학교 의과대학 춘천성심병원 외과학교실, 1내과학교실
정민성ㆍ김해성ㆍ류병윤ㆍ김홍기ㆍ홍성일ㆍ이정훈ㆍ김한준ㆍ전장용ㆍ김진봉
1Clinical Review of 1,211 Cases of Laparoscopic Cholecystectomy in the Northwestern Province of Gangwon-do
Min Sung Chung, M.D., Hae Sung Kim, M.D., Byoung Yoon Ryu, M.D., Hong Ki Kim, M.D., Sung Il Hong, M.D., Jung Hun Lee, M.D., Han Joon Kim, M.D., Jang Yong Jun, M.D., Jin Bong Kim, M.D.
1Departments of Surgery and
1Internal Medicine, College of Medicine, Hallym University, Chuncheon, Korea
Purpose: We have performed 1,211 cases of laparoscopic
cholecystectomy in the northwest province of Gangwon-do since 1993. This study aims to analyze our cases of laparoscopic cholecystectomy that were performed over 16 years and to evaluate the proper current treatment for gallbladder disease.Methods: A retrospective study was conducted on 1,211
patients who underwent laparoscopic cholecystectomy at Chuncheon Sacred Heart Hospital between February 1993 and February 2008. We analyzed the patients’ age, gender and chief complaints, the diagnostic methods, the preoperative diagnosis, the conversion rate, surgical complications, pathology and length of the hospital stay.Results: The mean age was 51.7±15.8 years. The
male-to-female ratio was 1:1.4. The chief complaints were right upper quadrant pain (47.6%), epigastric pain (13.1%) and abdominal pain (11.9%). Abdominal sonography and ERCP were performed in 91.9% and 82.2% of the patients, respectively, during the early ten years, but in the recent six years, MRCP often took place of these procedures (65.7%).Laparoscopic cholecystectomy was performed for gallbladder
stone (69.6%), polyp (11.7%), acute cholecystitis and empyema (5.0%). Chronic cholecystitis was the leading pathologic diagnosis (76.9%) followed by acute cholecystitis (11.3%) and polyp (6.6%). The mean operation time was 453.1±24.6 minutes. The conversion rate was 10.9% with inflammatory adhesion being the most common cause of conversion. The postoperative complication rate was 1.8%, and bile leak was the leading cause of this. Overall, the length of the hospital stay was 4.1±2.0 days.
Conclusion: With the broad application of laparoscopic
cholecystectomy, the conversion rate might not be reduced even as physicians’ experience with this procedure increases, but the proper selection of patients and the decision making for conversion when facing severe inflammation or adhesion during the laparoscopic approach is critical for safely managing patients and avoiding critical complications.
Key words: Laparoscopic cholecystectomy, Gallbladder stone,
Acute cholecystitis중심단어: 복강경 담낭절제술, 담석, 급성 담낭염
※ 통신저자:류병윤, 강원도 춘천시 교동 153 우편번호:200-704
한림대학교 춘천성심병원 외과 Tel:033-240-5179, Fax:033-243-6413 E-mail:[email protected]
서 론
복강경 담낭절제술은 1987년 Philippe Mouret1에 의해 처음 도입된 후 개복수술에 비해 통증이 적으며 회복이 빨라 입 원기간이 짧고, 창상의 미용효과가 좋아 담석증을 비롯한 양성 담낭질환에 외과적 치료의 표준 술식으로 자리잡았다.
초기 복강경 담낭절제술은 급성 담낭염, 담관결석이 상대적 금기증이었으나, 경험의 축적과 술기의 발전으로 급성 담낭 염 및 총담관 결석에서도 복강경수술이 시도되고 있으며,2 수술 합병증 및 개복수술로의 전환도 점차 감소하고 있다.
강원 영서 북부 지역에서는 1993년 2월 본원에서 처음 도 입된 이후 2008년 2월까지 1,211예의 복강경 담낭절제술을 시행하였다. 이에 저자들은 16년간 시행된 복강경 담낭절 제술 1,211예를 분석하여 문헌 고찰과 함께 보고하는 바이다.
대상 및 방법
1993년 2월부터 2008년 2월까지 16년간 복강경 담낭절제 술을 시행한 1,211명의 환자를 대상으로 후향적 연구를 시 행하였다. 저자들은 의무기록을 기준으로 대상 환자들의 주소, 수술 전 진단 방법, 수술 전 진단, 개복수술로의 전환, 합병증, 병리조직검사 및 재원기간 등에 대하여 조사하였다.
수술방법은 기본적인 4공식을 채택하였으며 CO2 기복 하에 3인조로 수술 팀을 구성하여 복강경 담낭절제술을 시 행하였다. 비위관과 도뇨관은 수술전 삽입 후 수술 직후 제 거하였다.
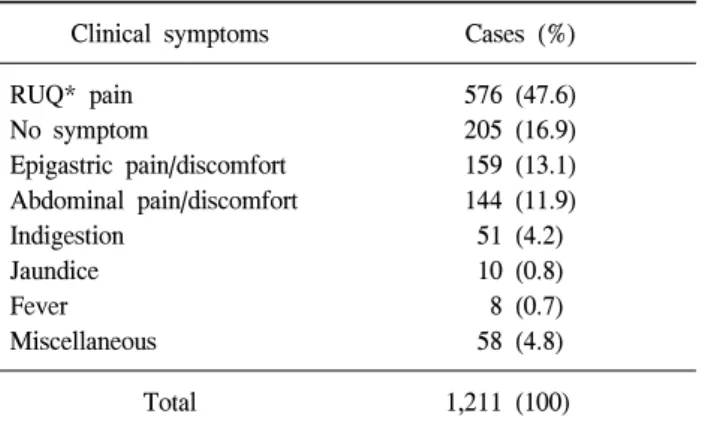
Table 1. Chief complaints of patients undergoing laparoscopic
cholecystectomyClinical symptoms Cases (%)
RUQ* pain No symptom
Epigastric pain/discomfort Abdominal pain/discomfort Indigestion
Jaundice Fever Miscellaneous
576 (47.6) 205 (16.9) 159 (13.1) 144 (11.9) 51 (4.2) 10 (0.8) 8 (0.7) 58 (4.8)
Total 1,211 (100)
*RUQ = right upper quadrant.
Fig. 1. Age and sex distribution.
Table 2. Preoperative diagnosis
Preoperative diagnosis Number (%) GB* stone
GB* polyp
GB*+Common bile duct stone Acute cholecystitis
Adenomyomatosis Acalculous cholecystitis Others
843 (69.6) 142 (11.7) 78 (6.4) 61 (5.0) 23 (1.9) 22 (1.8) 42 (3.6)
Total 1,211 (100)
*GB = gallbladder.
Fig. 2. Preoperative diagnostic work-up.
결 과 1) 연령, 성별 및 임상 양상
평균 연령은 51.7±15.8세(11∼92)이었다. 510예, 여자 701 예로 남녀의 성비는 1:1.4였다(Fig. 1).
수술 전 증상으로 우상복부 동통이 576예(47.6%)로 가장 많았으며 자각 증상이 없는 담석 또는 용종성 질환이 205예 (16.9%), 심와부 동통이나 불편함이 159예(13.1%), 복부 전 반의 동통이나 불편함이 144예(11.9%), 소화불량이 51예 (4.2%), 황달이 10예(0.8%), 고열이 8예(0.7%)였다(Table 1).
2) 수술 전 영상 검사
초기 진단을 위하여 복부 초음파를 시행하였다. 담낭관 및 담도의 이상 유무, 담도결석확인을 확인하는 방법으로 10년간 내시경적역행성담췌관조영술을 선별적으로 시행하 였고 2003년 이후부터 자기공명담도촬영술을 시행하였다.
담도결석이 확인된 환자는 내시경적역행성담췌관조영술을
통한 유문절개술로 결석을 제거 후 복강경 담낭절제술을 시행하였다.
복부 초음파는 930예(76.8%)에서 시행하였으며 내시경적 역행성담췌관조영술과 자기공명담도촬영술을 각각 695예 (57.4%)와 408예(33.7%)에서 시행하였다. 담도 결석이 확인 된 115예(9.5%)는 내시경적 유문 절개술 및 담도결석 제거 후 복강경 담낭절제술을 시행하였다. 그 외 담도계 동위원 소 촬영이 428예(35.3%), 복부 컴퓨터단층촬영이 404예 (33.4%)가 시행되었다.
초기 10년간 전체 595예 중 489예(82.2%)에서 내시경적 역행성담췌관조영술을 시행하였으나 자기공명담도촬영술 이 도입된 2003년 이후부터는 616예 중 405예(65.7%)에서 자기공명담도촬영술을 시행하였다(Fig. 2).
3) 수술 전 진단
수술 전 진단은 담낭결석증이 843예(69.6%), 담낭용종이 142예 (11.7%), 총담관결석과 동반된 담석증이 78예(6.4%), 급성 담낭염 61예(5.0%), 담낭선근종증 23예(1.9%), 무결석 담낭염 22예(1.8%), 용종을 동반한 담석증 17예(1.4%) 이었 다(Table 2).
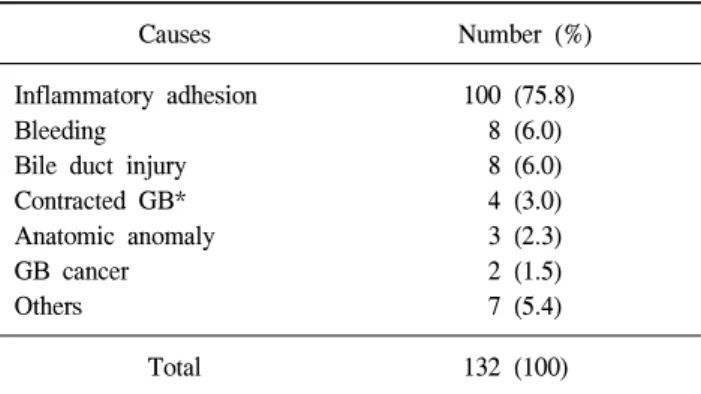
Table 3. Causes of conversion to open cholecystectomy
Causes Number (%)
Inflammatory adhesion Bleeding
Bile duct injury Contracted GB*
Anatomic anomaly GB cancer Others
100 (75.8) 8 (6.0) 8 (6.0) 4 (3.0) 3 (2.3) 2 (1.5) 7 (5.4)
Total 132 (100)
*GB = gallbladder.
Table 5. Pathologic diagnosis
Diagnosis Number (%)
Chronic cholecystitis Acute cholecystitis GB* polyp Adenomyomatosis Malignancy GB* adenoma Others
932 (77.0) 138 (11.4) 81 (6.7) 16 (1.3) 13 (1.1) 6 (0.5) 25 (2.0)
Total 1,211 (100)
*GB = gallbladder.
Table 4. Operative complication
Complication Number (%)
Bile leak Pancreatitis Port site bleeding GB* bed bleeding Wound infection
Common bile duct obstruction Miscellaneous
9 (39.1) 4 (17.4) 3 (13.0) 2 (8.7) 1 (4.3) 1 (4.3) 3 (13.2)
Total 23 (100)
*GB = gallbladder.
Fig. 3. Mean hospital stay for laparoscopic cholecystectomy.
4) 개복수술로의 전환
개복수술로 전환한 경우는 132예(10.9%)이었다. 염증 및 유착으로 담낭관 및 Calot 삼각의 박리가 어려웠던 경우가 100예(75.8%), 출혈이 8예(6.0%), 담도손상이 8예(6.0%)가 있었다(Table 3).
5) 합병증
합병증은 23예(1.8%)에서 발생하였다. 담즙 유출이 9예 (39.1%)에서 발생하였고 췌장염이 4예(17.4%), 투관침 부위 의 출혈이 3예(13.0%), 담낭 기저부의 출혈이 2예(8.7%) 있 었다(Table 4).
6) 병리 조직검사
만성 담낭염이 932예로 가장 많았고(77.0%) 급성 담낭염 이 138예(11.4%), 용종이 81예(6.7%), 선근종과 선종이 각각 16예(1.3%)와 6예(0.5%)이었다. 그 외 악성 종양도 13예 (1.1%)가 있었다(Table 5).
7) 재원기간
평균 재원기간은 4.1±2.0일이었다(Fig. 3).
고 찰
초기 복강경 담낭절제술의 적응증은 단순한 담낭질환에 불과하였다.3 그러나 복강경 수술에 대한 경험의 축적, 술기 의 향상 및 기구의 발달로 인하여 적응증의 범위가 점차 넓어지고 있다.4
Gadacz와 Talamini5는 복강경 담낭절제술에 대한 금기증 은 수술자의 숙련도와 환자의 상태에 따라 변한다고 하였 다. Lillemore6는 최근에 증상이 있었던 담낭결석증 환자의 94%가 복강경 담낭절제술의 적응이 되었다고 하며 담낭암, 담낭장관루에서만 복강경 담낭절제술의 금기가 된다고 하 였다.
급성 담낭염의 경우 복강경수술의 경험이 풍부해지면서 복강경을 통한 접근이 1차적으로 시도되고 있다. Min 등7은 복강경 담낭절제술은 급성 담낭염과 합병증을 동반한 담낭 염에서도 일차적 치료로 선택할 수 있는 매우 유용한 치료 법이라 하였고 Fabre 등8은 급성 담낭염에서 복강경 담낭절 제술의 합병증 발생율이 개복수술에 비해 큰 차이가 없다 고 하였다. 또한 Lee 등9은 급성 담낭염을 동반한 60세 이상
의 American Society of Anesthesiologists (ASA) 2, 3군의 고 위험군에서도 복강경 담낭절제술을 시행하는 것이 유용한 치료법이라 주장하였다.
저자들의 경우 담낭 축농을 포함한 급성 담낭염의 복강 경 수술 비중이 높아지고 있는데 복강경 담낭절제술의 시 행 초기인 1993년부터 2000년까지 복강경 담낭절제술 중 1.8%가 급성 담낭염이었으나 최근 8년에는 복강경 술기의 숙련으로 적응증이 확대되어 급성 담낭염에 대한 복강경 담낭절제술이 6.6%로 증가하였다. 저자들은 수술 전 담도 및 담낭관의 해부학적 구조를 확인하기 위하여 내시경적역 행성담췌관조영술과 자기공명담도촬영술을 시행하였다.
자기공명담도촬영술이 도입되기 전 복강경 담낭 절제술 595예 중 82.2%에서 내시경적역행성담췌관조영술을 시행 하였다. 이후 자기공명담도촬영술의 도입으로 역행성 담췌 관 조영술의 비중은 점차 낮아지고 있으나 초음파 검사에 서 담도계의 확장, 총담관결석이 동반된 경우, 빌리루빈 수 치의 증가, 그리고 자기공명담도촬영술에서 담도 내 충만 결손이 발견된 경우 역행성 담췌관 조영술을 시행하여 담 석이 확인되면 내시경적 괄약근절개술을 시행한 후 총담관 결석을 제거하고 복강경 담낭절제술을 시행하였다.
복강경 담낭절제술의 수술시간은 국내의 경우 Jung 등10 의 보고에 의하면 1,000예를 시행한 결과 평균 56.3분이 소 요되었고 Park과 Shin11은 단일 술자에 의해 시행된 복강경 담낭절제술 1,000예에서 평균 수술시간은 57.0분이었고 후 기 500예의 경우 45.2분으로 단축되었다고 보고하였다. 저 자들의 경우 평균 53.1±24.6 분이 소요되었고 최근 5년간 평균 수술시간은 47.5±23.3분으로 수술 초기인 1993년도의 76.0±31.2분에 비해 30분 정도 단축되었다. 이는 시술자의 경험에 따라 수술시간이 단축된 것으로 사료된다.
복강경 담낭절제술과 관련된 합병증으로는 출혈, 담관손 상, 담즙 유출, 췌장염 등이 있다.12 이러한 합병증은 전체 환자의 약 5% 미만에서 보고되고 있는데 이 가운데 가장 치명적인 합병증은 담도손상으로 개복 담낭절제술에서의 발생률보다 높다.13,14 Daziel 등15에 의하면 복강경 담낭절제 술을 시행한 77,604명의 환자 가운데 담도손상(0.59%), 지 연성 담즙유출 및 출혈(0.29%), 수술 후 사망(0.04%)을 보고 하였다. 국내의 경우 Oh 등16은 1,500예의 환자 중 4.06%에 서 합병증이 발생하였고 그 중 출혈이 가장 많은 2.46%를 차지하며 담즙유출(0.46%), 담도손상(0.33%), 장관손상 (0.26%)이 발생하였다. 저자들의 경우 수술 후 합병증은 1.8%에서 발생하였다. 이 중 담도손상 및 담즙유출이 전체 환자의 0.74%, 투관침 부위의 출혈(0.24%), 담낭 기저부의 출혈(0.16%) 등이 있었다.
개복수술로의 전환은 3%에서 8%까지 보고되고 있다.17,18 Fried 등19은 압통 및 우상복부 통증 등의 급성복증이 있는 환자에게 개복수술로의 전환이 8배나 높음을 밝혀내고 이 를 가장 중요한 인자로 뽑았으며 그 외 남자, 65세 이상, 영
상검사에서 담낭벽의 비후가 주요 인자라 하였다. 국내의 경우 Kim 등20은 3,510 명의 환자 중 1.88%, Park과 Shin11은 2.5%의 전환률을 보고하였다. 외국의 경우 Sanabria 등21은 5%, Mattioli 등22은 4.16%, Lo 등23은 11%의 전환율을 보고 하였다. 저자들의 경우 개복수술로의 전환은 10.9% (132예) 로 타 보고와 큰 차이가 없었다.
평균 입원기간은 저자들의 경우 4.1±2.0일이며 최근 2007 년의 경우 3.7±1.4일로 재원기간이 점차 감소하였다(Fig. 3).
이는 국내에서 보고된 3.7∼5.0일11,24,25과 차이는 없었다.
결 론
복강경 담낭절제술은 술기의 숙달 및 기구의 개발로 복 강경수술 초기보다 합병증이 감소하고, 수술 적응증이 확 대 되었다. 저자들은 담낭관 및 담도 해부학적 구조를 수술 전 검사로 확인하여 수술합병증을 감소시킬 수 있었다. 하 지만 급성담낭염에 대한 수술 적응증의 확대로 개복술로의 전환율의 감소는 이루지 못하였다.
참고문헌
1) Mouret P. From the first laparoscopic cholecystectomy.
Digestive Surg 1987;8:124-125.
2) Muhammed AM, Hesham H, Muhammed IM. Laparoscopic common bile duct exploration: the past, the present and the future. Am J Surg 2000;179:309.
3) Gollan JL, Kalser SC, Henry AP, Strasberg SM. Preceding of the NIH consensus development conference on gallstones and laparoscopic cholecystectomy. Am J Surg 1993;165:387.
4) Beery PR, Ellison EC. Surgery in the pregnant patient. In:
Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 17th ed. Philadelphia: Elsevier. Saunders;
2004.2277.
5) Gadacz TR, Talamini MA. Traditional versus laparoscopic cholecystectomy. Am J Surg 1991;161:336-338.
6) Lillemore KD. Cholecystectomyfor gallstones. 82nd annual clinical congress ACS postgraduate course. Minimal Access Surgey 1996;7:5.
7) Min SK, Han HS, Kim YW, et al. Application of laparoscopic cholecystectomy in acute cholecystitis. J Korean Surg Soc 2001;61:312-316.
8) Fabre JM, Fagot H, Domergue J, et al. Laparoscopic cholecystectomy in complicated cholelithiasis. Surg Endosc 1994;8:198-201.
9) Lee NJ, Han HS, Kim YW, Min SK, Choi YM. The safety of a laparoscopic cholecystectomy in acute cholecystitis in high risk patients older than sixty. J Korean Surg Soc 2003;64:396-401.
10) Jung JH, Park JY, Kim SH, et al. A clinical review of 1,000
cases of laparoscopic cholecystectomy. J Korean Soc Endosc Laparosc Surg 2000;3:42-50.
11) Park GJ, Shin JH. 1,000 cases of laparoscopic cholecy- stectomy by a single surgeon. J Korean Surg Soc 2004;66:
123-127.
12) Mrksic M, Cabafi Z, Feher I, Mirkovic M. Surgical trauma in laparoscopic and classical cholecystectomy. Med Pregl 2001;54:327-331.
13) Lee VS, Chari RS, Cuccchiaro G, Meyers WC. Complications of laparoscopic surgery. Am J Surg 1993;165:527.
14) Gouma DJ, Go PM. Bile duct injury during laparoscopic and conventional cholecystectomy. J Am Coll Surg 1994;253:
229-233.
15) Deziel DJ, Millikan KW, Economou SG, Doolas A, Ko ST, Airan MC. Complication of laparoscopic cholecystectomy. A national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J surg 1992;165:9-14.
16) Oh JS, Park YG, Chi KC, Lee JH, Chang IT, Kim SJ. A clinical review of 1,500 cases of laparoscopic cholecy- stectomy. J Korean Surg Soc 1995;48:508-517.
17) Cuschieri A, Dubios F, Mouriel J, et al. The European experience with laparoscopic cholecystectomy. Am J Surg 1991;161:385-387.
18) The Southern Surgeons Club. A prospective analysis of 1,581 laparoscopic cholecystectomies. N Engl J Med 1991;324:
1073-1078.
19) Fried GM, Barken JS, Sigman HH, et al. Factors determining conversion to laparotomy in patients undergoing laparoscopic cholecystectomy. Am J Surg 1994;167:35.
20) Kim YS, Chang IT, Park YG, Lee JH, Chi KC. Kim SJ.
Factors for conversion from laparoscopic cholecystectomy to open cholecystectomy. J Korean Surg Soc 2002;63:233-237.
21) Sanabria JR, Gallinger S, Croxford R, Strasberg SM. Risk factors in elective laparoscopic cholecystectomy for convert- sionto open cholecystectomy. J Amm Coll Surg 1994;179:
696-704.
22) Mattioli FP, Cagnazzo A, Razzetta F, et al. Laparoscopic cholecystectomy. An analysis of the reasons for a conversion to conventional surgery in an elective surgery department.
Minerva Chir 1999;54:471-476.
23) Lo CM, Fan ST, LiuCL, Edward CS. Early decision for conversion of laparoscopic to open cholecystectomy for treatment of acute cholecystitis. Am J Surg 1997;173:513-517.
24) Baek JH, Kwak SS. Clinical review of laparoscopic cholecystectomy. J Korean Surg Soc 2000;58:259-264.
25) Song HS, Chai KM, So BJ, Lee JK, Lee KM. A clinical analysis of 222 cases of laparoscopic cholecystectomy and the statistical analysis for pain precipitating factors. J Korean Surg Soc 1994;47:118-124.