I. 서 론
만성폐쇄성폐질환(Chronic obstructive pulmonary disease, COPD)은 완전히 가역적이지 않은 지속적인
기류제한을 특징으로 하는 예방 및 치료가 가능한 질병 으로 정의되는데, 기류제한은 일반적으로 진행성이고 유해한 분진 또는 가스에 대한 기도 및 폐의 만성적 염 증반응의 증가와 관련이 있다(Rabe et al., 2007). 폐
https://doi.org/10.15269/JKSOEH.2019.29.2.251
광산 이직근로자의 만성폐쇄성폐질환 기류제한 중증도와 염증 및 산화스트레스
이종성*ㆍ신재훈ㆍ백진이ㆍ정지영1ㆍ최병순 근로복지공단 직업환경연구원, 1동아대학교 의약생명공학과
Inflammation and Oxidative Stress as related to Airflow Limitation Severity in Retired Miners with Chronic Obstructive Pulmonary Disease
Jong Seong Lee*ㆍJae Hoon ShinㆍJin Ee BaekㆍJi Yeong Jeong1ㆍByung-Soon Choi Institute of Occupation and Environment, Korea Workers’ Compensation & Welfare Service
1Department of Medical Biotechnology, Dong-A University
ABSTRACT
Objective: Chronic obstructive pulmonary disease(COPD) is characterized by persistent airflow limitations associated with chronic inflammatory response due to noxious particles or gases in the lung. Inflammation and oxidative stress are associated with COPD. The aim of this study was to evaluate the relationship among inflammation, oxidative stress, and airflow limitation severity in retired miners with COPD.
Methods: The levels of serum high-sensitivity C-reactive protein(hsCRP) as a biomarker for inflammation, degree of reactive oxygen metabolites(dROMs) and biological antioxidants potential(BAP) in plasma as biomarkers for oxidative stress were measured in 211 male subjects with COPD. Degree of airflow limitation severity as determined by spirometry was divided into three grades grouped according to the classification of the Global Initiatives for Obstructive Lung Disease(GOLD)(1, mild; 2, moderate; 3≤, severe or more) using a fixed ratio, post- bronchodilator FEV
1/FVC < 0.7.
Results: Mean levels of dROMs significantly increased in relation to airflow limitation severity(GOLD 1, 317.8 U.CARR vs. GOLD 2, 320.3 U.CARR vs. GOLD 3≤, 350.9 U.CARR, p=0.047) and dROMs levels were correlated with serum hsCRP levels(r=0.514, p<0.001). Mean levels of hsCRP were higher in current smokers(non- smoker, 1.47 mg/L vs. smoker, 2.34 mg/L, p=0.006), and tended to increase with degree of airflow limitation severity(p=0.071). Mean levels of BAP were lower in current smokers(non-smoker, 1873 μmol/L vs. smoker, 1754 μmol/L, p=0.006).
Conclusions: These results suggest that inflammation and oxidative stress are related to airflow limitation severity in retired miners with COPD, and there was a correlation between inflammation and oxidative stress.
Key words: chronic obstructive pulmonary disease, inflammation, oxidative stress
*Corresponding author: Jong Seong Lee, Tel: 010-2366-5075, E-mail: [email protected], 2F Incheon Labor & Welfare Complex, 478, Munemi-ro, Bupyeong-gu, Incheon 21417 Received: April 29, 2019, Revised: June 4, 2019, Accepted: June 7, 2019
Jong Seong Lee http://orcid.org/0000-0002-1672-0171 Jae Hoon Shin http://orcid.org/0000-0001-9436-6860 Jin Ee Baek https://orcid.org/0000-0002-4932-8520 Ji Yeong Jeong https://orcid.org/0000-0002-7009-1230 Byung-Soon Choi https://orcid.org/0000-0003-3551-0804
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
에서의 염증반응은 말초기관지, 폐실질 및 폐정맥의 벽 에서도 나타나며 전신순환계에도 영향을 미친다 (Agusti, 2006). 석탄분진과 결정형 유리규산 등의 무 기분진에 감수성이 있는 근로자가 노출될 경우 고전적 의미의 진폐증을 비롯하여 폐섬유화증, 폐부종, 만성기 관지염 및 COPD 등을 일으킬 수 있다(Cohen et al., 2008).
COPD의 발병 기전이 완전히 규명된 것은 아니지만, 활성산소(reactive oxygen species, ROS)와 항산화능 간의 불균형으로 정의되는 산화스트레스가 중요한 역할 을 하는 것으로 알려져 있다(Repine et al., 1997;
MacNee, 2005; Kirkham & Barnes, 2013). 산화스 트레스는 호흡기 염증과 상호 연관성이 있고 중증의 COPD 또는 악화기간에 증가한다고 하였다(Kostikas et al., 2003; Singh et al., 2017). 염증반응에 중요한 역할을 담당하는 ROS는 석탄 및 유리규산과 같은 무기 분진으로부터 직접 생성되기도 하고, 분진으로부터 활 성화된 폐포 대식세포와 호중구 등의 염증세포에서 생 성되기도 한다. 특히 철과 같은 전이금속이 포함된 분진 은 ROS 생성을 가중시킬 수 있다(Schins & Borm, 1999).
ROS에 의한 영향은 주로 산화적 손상의 형태이며, ROS와 항산화제 간의 불균형이 있을 때 더욱 증가한 다. 유전자의 산화적 손상은 돌연변이를 일으키는 개시 자의 역할 뿐만 아니라, 세포의 성장을 유도하는 유전자 를 자극하여 세포의 증식을 촉진시키는 역할을 한다고 알려져 있다(Sun, 1990). ROS와 관련된 질병을 예방하 고 관리하기 위해서는 직접 생체 내의 ROS를 평가하는 것이 좋지만, ROS는 반감기가 극히 짧기 때문에 생체 시료에서 ROS를 직접 평가하기는 매우 어렵다. 따라서 산화스트레스 연구에는 일반적으로 항산화제 및 산화적 손상에 의해 생성된 손상지표 등이 이용되고 있다. 최근 혈장 중의 hydroperoxide와 같은 활성산소의 대사물 질 수준(degree of reactive oxygen metabolites, dROMs)과 생체 항산화력(biological antioxidants potential, BAP) 등을 이용하여 생체 산화스트레스를 평가하는 방법이 보고되었다(Hirose et al., 2009; Fukui et al., 2011; Morimoto et al., 2016).
혈중 C-reactive protein(CRP)은 생체의 염증 또는 조직손상을 반영하는 급성기 반응물질로 염증성 cytokine 과 연관되어 간에서 합성된다(Pepys & Hirschfield,
2003). COPD 환자의 전신염증지표에 관한 메타분석 에서 COPD 환자의 CRP 농도는 대조군보다 일관성 있 게 증가한다고 하였으며(Gan et al., 2004; Chen et al., 2016; Su et al., 2016), Tkacova et al.(2007)은 급성 COPD 악화환자에서 COPD의 기류제한 중증도 가 심할수록 CRP농도가 증가하고 산화스트레스와 관련 성이 있다고 하였다.
흡연이 COPD의 가장 주요한 원인으로 알려져 있지만 (Strassmann et al., 2009; Lamprecht et al., 2011), 무기분진은 흡연과 무관하게 COPD의 위험요인이고, 특 히 석탄광부 등은 COPD의 위험직종이라고 하였다 (Meijers et al., 1997; Coggon & Anthony, 1998;
Bergdahl et al., 2004). 그러나 COPD의 주요한 영향요 인인 직업적 노출을 고려한 연구는 많이 없고, COPD 환자 를 대상으로 dROMs 등과 같은 최신의 생체지표를 이용한 산화스트레스 연구는 매우 적은 실정이다. 따라서 이 연구 는 광물성 분진에 노출경험이 있는 COPD 환자를 대상으 로 기류제한 중증도에 따른 염증과 산화스트레스 지표의 농도변화와 생체지표 간의 관련성을 보고자 하였다.
Ⅱ. 대상 및 방법
1. 연구대상
연구대상자는 과거 석탄 또는 석재분진 등에 노출경험 이 있는 이직근로자로서 COPD의 업무상 질병여부 진단 을 위해 ○○연구원에 내원한 수진자 중 COPD로 진단된 남자 211명이었다. 이 연구는 ○○연구원 기관생명윤리 위원회(No. 2017-02-02, 2016.11.24)의 연구계획 승 인 및 연구대상자의 자발적 서면동의를 획득한 후 수행하 였다.
2. 연구방법
1) 연구대상자의 일반적 특성 및 연구집단 구분
연구대상자의 나이, 체질량지수(body mass index, BMI), 분진 노출기간 및 흡연여부 등의 일반적 특성은 면접조사를 통해 조사하였다.
폐기능은 미국흉부학회/유럽호흡기학회에서 권장하는 방법(Miller et al., 2005)을 준용하여 폐기능 검사기 (Vmax22, sensorMedics, USA)로 검사하였다. 노력성 폐활량(forced vital capacity, FVC) 및 노력성 일초간 호기량(forced expiratory volume in one second,
FEV1)을 측정한 후, 한국인 예측식(Choi et al., 2005) 으로 각각의 예측치를 계산하였다. COPD의 진단은 대 한결핵 및 호흡기학회에서 정하고 있는 기준(KATRD, 2005)에 따라 속효성 β2-기관지 확장제를 흡입한 후 검사한 FEV1이 200 mL 및 12% 미만으로 증가하고 일 초율(%FEV1/FVC)이 70% 미만인 경우로 하였다.
COPD 환자의 기류제한 중증도에 따른 연구집단의 구분은 Global Initiatives for Obstructive Lung Disease(GOLD)의 기준(Vogelmeier et al., 2017)에 따라 %FEV1 예측치가 80% 이상인 경우 GOLD 1(경 증), 50% 이상 80% 미만인 경우 GOLD 2(증등증) 그 리고 50% 미만인 경우 GOLD 3≤(중증 이상)으로 하 였다.
2) 생체시료 분석
혈중 산화도 지표인 dROMs와 항산화력 지표인 BAP 분석은 Morimoto et al.(2016)의 방법을 준용하 여 생체 자유라디칼 분석기(FREE CARRIO 200, Diacron International, Italy)의 방법에 따라 분석하 였다. dROMs의 분석은 헤파린 항응고제로 처리한 혈 장에 들어있는 hydroperoxide를 alkoxy radical 또 는 peroxide radical로 변환시키고 발색시약(N,N- diethyl- p-phenylenediamine)을 첨가한 후, 흡광분 석으로 정량하였다. dROMs의 단위는 carratelli unit (U.CARR)로 표기하였으며, 1 U.CARR은 0.08 mg/dL 의 과산화수소(hydrogen peroxide, H2O2)에 해당한다.
BAP의 분석은 3가 철염(FeCl3)에 무색의 thiocyanate 염을 첨가하여 발색시킨 후, 혈장을 첨가하여 혈장내 항산화제에 의한 환원탈색 반응을 흡광분석으로 정량 하였으며, 단위는 μ㏖/L로 표기하였다.
항응고제가 첨가되지 않은 혈액은 혈청을 분리한 후, CRP와 간 및 신장기능 지표의 농도를 자동생화학 분석기(7080 automatic analyzer, Hitachi High- Technologies Co., Japan)로 분석하였는데, CRP 농도 는 미량분석이 가능한 high-sensitivity CRP(hsCRP)로 분석하였다. 간기능은 aspartate aminotransferase (>38 IU/L), alanine aminotransferase(>44 IU/L) 또는 gamma-glutamyltransferase(>73 IU/L), 신장 기능은 blood urea nitrogen(>20 ㎎/dL) 또는 creatinine(>1.2 ㎎/dL)의 정상 참고치를 하나이상 초 과하는 경우 각각 비정상으로 분류하였다.
3) 통계분석
통계분석은 SPSS 17.0 프로그램(IBM SPSS statistics, USA)으로 수행하였다. BMI, dROMs 및 BAP 등은 정 규분포하였고, 나이는 제곱변환 후 정규분포하였으며, 분진 노출기간과 hsCRP는 로그변환 후 정규분포 하였 다. COPD 기류제한 중증도에 따른 연구집단 간의 일 반적 특성 비교는 교차분석 또는 분산분석으로 검정하 였고, 일반적 특성별 생체지표의 농도 비교는 평균분석 또는 분산분석으로 검정하였다. 기류제한 중증도에 따 른 연구집단 간의 생체지표 농도는 공변량(GOLD 분류 기준인 폐기능 제외)이었던 나이, BMI 및 분진 노출기 간 등을 통제한 공분산분석(analysis of covariance, ANCOVA)으로 검정하였다. 생체지표 간의 관련성은 상관분석으로 검정하였다. 각 분석의 통계적 유의수준 은 p<0.05로 하였다.
Ⅲ. 연구결과
1. 일반적 특성
연구대상자의 일반적 특성은 Table 1과 같다. COPD 의 기류제한 중증도에 따른 연구집단간 흡연, 간기능 및 신장기능 등은 차이가 없었으나, 나이, BMI, 분진 노출 기간 및 폐기능 등은 통계적으로 차이가 있었다.
2. 혈중 hsCRP, dROMs 및 BAP 농도
일반적 특성별 생체지표농도는 Table 2와 같다. 혈 중 hsCRP의 평균농도는 비흡연군보다 흡연군이 높았고 (1.47 mg/L vs. 2.34 mg/L, p=0.039), 누적흡연량이 증가할수록 평균농도가 증가하였다(p=0.006). dROMs 의 평균농도는 흡연군이 통계적 유의성은 없었으나 높 은 경향을 나타냈다(320.2 U.CARR vs. 340.5 U.CARR, p=0.067). BAP 평균농도는 나이가 증가할수록 BAP의 중위수 농도가 증가하였고(1839 μmol/L vs. 1900 μ mol/L vs. 1947μmol/L, p=0.048), 비흡연군에 비해 흡연군이 유의하게 낮았다(1873 μmol/L vs. 1754 μ mol/L, p=0.010). BMI, 분진노출기간, 고혈압, 간기능 및 신장기능에 따른 농도차이를 보인 생체지표는 없었다.
연구집단간 통계적 유의성이 있었던 나이, BMI 및 분진 노출기간을 통제한 공분산분석 결과, dROMs의 평균농도는 COPD 기류제한 중증도가 심할수록 유의하 게 증가하였고(GOLD 1, 317.8 U.CARR vs. GOLD
Characteristics GOLD 1 (N = 40) GOLD 2 (N = 149) GOLD 3≤ (N = 22) p values
Age (years); GM(GSD)* 72.8 (30.8) 70.0 (29.6) 71.4 (20.7) 0.045a
BMI (kg/m2) ; AM±SD 24.0 ± 3.2 23.3 ± 3.4 21.5 ± 3.7 0.018a
Exposure period, years; GM(GSD)† 16.5 (1.5) 13.6 (1.5) 14.9 (1.8) 0.039a
%FVC predicted; median(IQR) 93 (86-100) 87 (80 - 94) 84 (71 - 93) 0.001b
%FEV1 predicted; median(IQR) 84 (81 - 87) 69 (64 - 75) 44 (38 - 48) <0.001b
%FEV1/FVC ratio; median(IQR) 63.6 (58.2-66.9) 56.3 (50.9-62.8) 36.1 (30.7-44.1) <0.001b Cumulative smoking (pack-years); median(IQR) 16.3 (1.9-31.8) 18.0 (4.5-32.0) 27.0 (4.3-41.5) 0.452b
Current smoking; N(%) 2 (5.0) 25 (16.8) 2 (9.1) 0.126c
Abnormal LFT; N(%) 2 (5.0) 28 (18.8) 2 (9.1) 0.068c
Abnormal KFT; N(%) 4 (10.0) 11 (7.4) 2 (9.1) 0.194c
*Square transformed data
†Log transformed data
aCalculated by ANOVA
bCalculated by Kruskal-Wallis U test
cCalculated by χ2- test
Abbreviation: AM, arithmetic mean; BMI, body mass index; FVC, forced vital capacity; FEV1, forced expiratory volume in one second;
GM, geometric mean; GOLD, global initiatives for obstructive lung disease; GSD, geometric standard deviation; IQR, interquartile range;
KFT, kidney function test; LFT, liver function test; SD, standard deviation
Subjects were grouped by airway flow limitation severity in COPD(FEV1/FVC < 0.7) according to GOLD classification;
GOLD 1(mild), FEV1 ≥ 80% predicted
GOLD 2(moderate), 50% ≤ FEV1 < 80% predicted GOLD 3≤(severe or more), FEV1 < 50% predicted
Table 2. Mean levels of biomarkers as related to general characteristics
Characteristics No. of patients hsCRP* (mg/L) dROMs (U.CARR) BAP (μmol/L)
Age (years)† -69 94 1.56 (109.9) 321.0(109.9) 1839 ( 94.9)
70-79 98 1.56 (104.1) 317.5( 99.8) 1900 (113.2)
80- 19 1.00 ( 96.5) 329.0(119.0) 1947 (123.9)
(p= 0.630) (p = 0.325) (p = 0.048)
BMI (kg/m2)‡ ≥ 25 146 1.55 (3.18) 322.8 ± 54.4 1866 ± 250
< 25 65 1.60 (2.88) 323.5 ± 58.3 1836 ± 189
(P = 0.863) (p = 0.935) (p = 0.384)
Exposure period (years)‡ - 9 33 1.66 (3.04) 319.1 ± 64.5 1891 ± 216
10-19 133 1.56 (3.14) 323.0 ± 55.9 1843 ± 241
20- 45 1.52 (2.98) 325.9 ± 47.7 1872 ± 222
(P = 0.944) (p = 0.869) (p = 0.496)
Current smoking‡ No 182 1.47 (3.07) 320.2 ± 54.8 1873 ± 223
Yes 29 2.34 (2.91) 340.5 ± 57.4 1754 ± 272
(p = 0.039) (p = 0.067) (p = 0.010)
Cumulative smoking, Never 29 1.11 (2.87) 303.2± 45.8 1872± 223
Pack-years‡ 0.1-20.0 89 1.37 (3.02) 324.4± 50.9 1864± 217
20.1-40.0 56 1.65 (3.21) 324.5± 49.0 1802± 273
40.1- 37 2.65 (2.73) 332.9± 76.7 1907± 205
(p= 0.006) (p = 0.173) (p = 0.168)
Liver function‡ Normal 179 1.60 (3.09) 325.3± 54.5 1859± 223
Abnormal 32 1.41 (3.02) 310.3± 60.1 1843± 288
(p = 0.567) (p = 0.162) (p = 0.728)
Kidney function† Normal 194 1.50 (104.4) 320.5(106.1) 1881(106.4)
Abnormal 17 1.90 (124.8) 317.0(104.7) 1941(101.6)
(p = 0.186) (p = 0.924) (p = 0.756)
*Log transformed data
†Calculated by Mann-Whitney H test or Kruskal-Wallis U test, median (mean rank)
‡Calculated by t-test or ANOVA, AM ± SD or GM(GSD)
Abbreviation: AM, arithmetic mean; BAP, biological antioxidants potential; BMI, body mass index; dROMs, degree of reactive oxygen metabolites; COPD, chronic obstructive pulmonary diseases; GM, geometric mean; GSD, geometric standard deviation ; hsCRP, high-sensitivity C-reactive protein
Table 1. General characteristics of the study subjects(N=211)
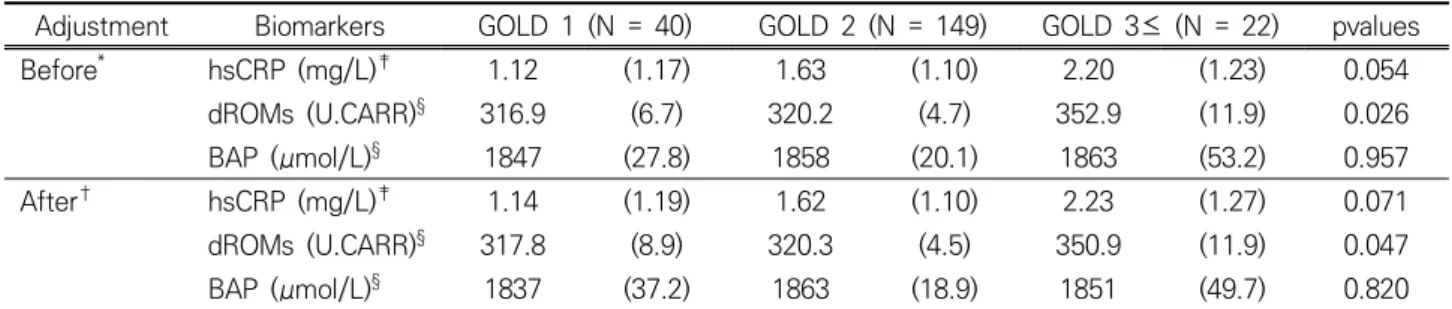
2, 320.3 U.CARR vs. GOLD 3≤, 350.9 U.CARR, p=0.047), hsCRP의 평균농도는 통계적 유의성은 없었 으나 기류제한 중증도가 심할수록 증가하는 경향을 나 타냈다(1.14 mg/L vs. 1.62 mg/L vs. 2.23 mg/L, p=0.071)(Table 3). 혈중 hsCRP 농도와 dROMS 농도 간에는 양의 상관성이 있었다(r=0.514, p<0.001).
Ⅳ. 고 찰
COPD의 발병과 진행의 주요한 위험요인은 흡연이지 만(Strassmann et al., 2009), Balmes et al.(2003)은 COPD 환자의 10-20%가 직업적 노출에 의해 발병하며, Hnizdo et al.(2002)은 비흡연 COPD 환자의 31.1%가 직업적 노출로 인해 발병한다고 추정하였다. 분진과 같은 유해인자 노출은 기도 상피세포에 직접적인 손상을 일으 켜 호중구, 대식세포 및 림프구 등이 관여하는 기도염증 을 유발한다. 이와 같은 활성화된 염증세포로부터 기인한 ROS 및 단백질 분해효소의 생성이 증가할 수 있는데 (Repine et al., 1997), 항산화제 및 항단백질 분해효소 에 의해 충분히 균형이 잡히지 않는 산화스트레스는 더 많은 손상을 일으킬 수 있다(Larsson, 2007). COPD 환 자는 비흡연군 및 흡연 대조군에 비해 폐에서의 산화스트 레스가 증가한다고 하였다(MacNee, 2005).
생체 내에서 생성되는 주요한 ROS는 superoxide radical, hydroxy radical 또는 과산화수소(hydrogen peroxide) 등이 있는데, 이러한 ROS는 반감기가 극히 짧아 생체지표로는 부적절하다. 따라서 혈액 등 생체시 료를 이용한 산화스트레스 연구에는 주로 항산화 효소,
ROS scavenger, 지질 과산화물 및 DNA 손상지표 등 이 이용되고 있다(Gulumian et al., 2006). 그러나 최 근 COPD의 산화스트레스 연구에 dROMs와 같은 혈장 중의 총 산화도 또는 BAP와 같은 혈장 내의 항산화력 등 의 생체지표를 이용한 연구가 보고되었다. Stanojkovic et al.(2013)는 COPD 악화기의 산화도가 안정기 또는 정상 대조군에 비해 증가한다고 하였고, Foschino Barbaro et al.(2007) 및 Markoulis et al.(2006)는 COPD 환자의 dROMs 농도가 대조군보다 증가한다고 하였다. Singh et al.(2017)은 COPD 환자에서 산화스 트레스가 증가하고 질병의 중증도에 비례한다고 하였 다. 이번 연구에서도 dROMs의 평균농도는 COPD 기 류제한 중증도가 심할수록 통계적으로 유의하게 증가하 였는데(GOLD 1, 317.8 U.CARR vs. GOLD 2, 320.3 U.CARR vs. GOLD 3≤, 350.9 U.CARR, p=0.047), 이러한 결과는 산화스트레스가 COPD의 중증도가 심할 수록 증가된다는 선행연구들의 결과와 같았다.
COPD와 항산화제에 관한 선행연구에서 COPD 환 자의 항산화능(total antioxidants capacity)이 대조 군에 비해 감소한다고 보고하고 있는데(Rahman et al., 2000; ben Anes et al., 2014), 이는 ROS에 의해 항산화제의 소비가 증가하기 때문이라고 추론하였다 (Hanta et al., 2006). 그러나 Mak(2008)는 glutathione peroxidase의 농도는 감소하고 superoxide dismutase 와 glutathione(GSH)의 농도는 증가한다고 하였다. 이 러한 결과들로 볼 때, 선행연구들에서 COPD 환자의 항산화능이 일관성 있게 감소한다는 결과를 나타내지는 않는 것으로 보인다. 이번 연구에서 혈장 BAP 농도는
Adjustment Biomarkers GOLD 1 (N = 40) GOLD 2 (N = 149) GOLD 3≤ (N = 22) pvalues
Before
*hsCRP (mg/L)
‡1.12 (1.17) 1.63 (1.10) 2.20 (1.23) 0.054
dROMs (U.CARR)
§316.9 (6.7) 320.2 (4.7) 352.9 (11.9) 0.026
BAP (μmol/L)
§1847 (27.8) 1858 (20.1) 1863 (53.2) 0.957
After
†hsCRP (mg/L)
‡1.14 (1.19) 1.62 (1.10) 2.23 (1.27) 0.071
dROMs (U.CARR)
§317.8 (8.9) 320.3 (4.5) 350.9 (11.9) 0.047
BAP (μmol/L)
§1837 (37.2) 1863 (18.9) 1851 (49.7) 0.820
*
Calculated by ANOVA
†
Calculated by analysis of covariance (ANCOVA) adjusted by age, BMI, and exposure period
‡
Log transformed data, geometric mean (geometric standard error)
§
Arithmetic mean (arithmetic standard error)
Abbreviation: BAP, biological antioxidants potential; dROMs, degree of reactive oxygen metabolites; GOLD, global initiatives for obstructive lung disease; hsCRP, high-sensitivity C-reactive protein
Table 3. Covariate-adjusted levels of biomarkers among the study groups
비흡연군보다 흡연군이 낮았으나(1873 μ㏖/L vs.
1754 μ㏖/L, p=0.010), COPD의 기류제한 중증도에 따른 차이는 없었다(p=0.820). 이러한 원인으로는 BAP 의 분석원리가 혈장 내에 존재하는 albumin, bilirubin, 환원형 GSH, uric acid 등의 내인성 항산화제와 비타 민 C, 비타민 E, polyphenol과 같은 외인성 항산화제 에 의한 항산화력을 3가 철에 대한 환원력을 이용하는 것이므로, ROS에 의한 항산화제의 감소효과 이외에 식 이, 영양상태 및 다른 질병상태 등의 영향요인으로 인해 일관성 있는 BAP 감소효과를 반영하지 못하는 것으로 판단된다. 이번 연구에서 나이가 증가할 때 BAP의 농 도가 유의하게 증가하는 것으로 나타났다(p=0.048). 그 러나 황달 또는 통풍 등의 질병이 있는 경우에도 항산 화제인 bilirubin 또는 uric acid 등의 혈중농도가 증 가할 수 있기 때문에(Gutteridge, 1995; Anderson &
Cockayne, 2003), 나이와 BAP 간의 명확한 관련성 여부에 대해서는 추후 연구가 필요하였다.
혈청 CRP 농도는 COPD가 악화할 경우 대부분의 선행 연구에서 증가한다고 보고하고 있고(Karadag et al., 2008; Chen et al., 2016), COPD의 중증도가 심할수록 혈청 CRP 농도가 증가한다고 하였다(Tkacova et al., 2007). 이번 연구에서 혈청 hsCRP의 농도는 통계적 유의 성은 없었으나 COPD의 기류제한 중증도가 심할수록 평균 농도가 증가하는 경향이 있었고(GOLD 1, 1.14 mg/L vs.
GOLD 2, 1.62 mg/L vs. GOLD 3≤, 2.23 mg/L, p=0.071), dROMs 농도와 hsCRP 농도 간에는 양의 상관 성이 있었다(r=0.514, p<0.001). 이러한 결과로 볼 때, 염 증지표인 hsCRP의 농도는 COPD 기류제한 중증도가 심할 수록 증가하는 경향이 있고, hsCRP의 농도 증가와 dROMs 농도 증가 간에는 양의 관련성이 있는 것으로 판단된다.
담배 연기와 같은 입자를 흡입하면 호흡기의 염증세 포가 자극을 받거나 염증으로 인해 ROS 생성매개인자 가 활성화될 수 있다(Babior, 1999). 또한 담배연기에 는 가스상과 미립자 물질에 다량의 산화제를 포함하고 있고, ROS의 생성을 가중시킬 수 있는 철이 포함되어 있기 때문에 흡연은 COPD의 발병에 있어 가장 중요한 병인학적 요인이 될 수 있다(Pryor, 1997). Sethi &
Rochester(2000)는 COPD 발병률과 누적흡연량 간에 는 용량-반응의 관계가 있다고 하였다. 이번 연구에서 hsCRP의 평균농도는 비흡연군에 비해 흡연군이 높았고 (1.47 mg/L vs. 2.34 mg/L, p=0.039), 누적흡연량이 증 가할수록 평균농도가 증가하였다(p=0.006). 또한 dROMs
평균농도는 통계적 유의성은 없었으나 비흡연군에 비해 흡연군이 높은 경향을 보였다(320.2 U.CARR vs. 340.5 U.CARR, p=0.067). dROMs와 누적흡연량 간의 관련 성에 대한 선행연구는 없으나, Gao et al. (2017)은 현 재흡연 및 누적흡연량이 혈중 산화스트레스 지표인 8-isoprostane과 관련성을 나타낸다고 보고한 것으로 볼 때, 누적흡연량도 혈중 산화도와 관련이 있는 것으로 보인다. 즉, 염증지표인 hsCRP의 농도는 흡연군 및 누 적흡연량이 많을수록 증가하였고 염증과 산화도 지표 간 에 상관성이 있었으며, 통계적 유의성은 없었으나 흡연 군에서 산화도가 증가하는 경향이 있었다.
Ⅴ. 결 론
석탄 등의 광물분진에 노출경험이 있는 이직근로자에 서 발병한 COPD 집단을 대상으로 기류제한 중증도, 염 증 및 산화스트레스 지표 간의 관련성을 분석한 결과, 기 류제한 중증도가 심할수록 dROMS의 농도가 증가하였 고, hsCRP의 농도는 증가하는 경향을 나타냈다. 흡연군 은 비흡연군보다 hsCRP와 dROMs 농도가 증가하는데 비해 BAP의 농도는 감소하였고, 누적흡연량이 증가할수 록 hsCRP 농도가 증가하였으며, 혈중 hsCRP 농도와 dROMs 농도 간에는 상관성이 있었다. 이러한 결과로 볼 때, 광물성 분진 노출경험이 있는 COPD 환자에서 기류제한 중증도가 심하거나 흡연은 염증과 산화도 지표 의 농도 증가와 관련이 있고, 혈중 염증과 산화도 지표농 도 간에 상관성이 있었다. 이 연구는 흡연 이외에 직업적 분진노출로 인한 COPD 환자의 염증 및 산화스트레스 에 대한 기초연구로 활용될 수 있을 것으로 판단된다.
References
Agusti A. Thomas a. Neff lecture. Chronic obstructive pulmonary disease-a systemic disease. Proc Am Thorac Soc 2006;3:478-481(DOI:10.1513/pats.
200603-058MS)
Anderson SC & Cockayne S. Clinical Chemistry. Concepts
& applications. New York, The McGraw-Hill Co.;
2003. P.298, p.378-380
Babior BM. NADPH-oxidase: an update. Blood, 1999;93(5):1464-1476(PMID:10029572)
Balmes J, Becklake M, Blanc P, Henneberger P, Kreiss K et al. American Thoracic Society Statement:
Occupational contribution to the burden of airway
disease. Am J Respir Crit Care Med 2003;167(5):
787-797(DOI:10.1164/rccm.167.5.787)
ben Anes A, Fetoui H, Bchir S, ben Nasr H, Chahdoura H et al. Increased oxidative stress and altered levels of nitric oxide and peroxynitrite in Tunisian patients with chronic obstructive pulmonary disease:
correlation with disease severity and airflow obstruction. Biol Trace Elem Res 2014;161(1):
20-31(DOI:10.1007/ s12011-014-0087-4)
Bergdahl IA, Tore´n K, Eriksson K, Hedlund U, Nilsson T et al. Increased mortality in COPD among construction workers exposed to inorganic dust. Eur Respir J 2004;23:402–406(DOI:10.1183/09031936.
04.00034304)
Chen YW, Leung JM, Sin DD. A systematic review of diagnostic biomarkers of COPD exacerbation. PLoS One 2016;11(7):e0158843(DOI:10.1371/journal.pone.
0158843)
Choi JK, Paek DM, Lee JO. Normal predictive values of spirometry in Korean population. Tuberc Respir Dis.
2005;58:230-242(DOI:http://dx.doi.org/10.4046/
trd.2005.58.3.230)
Coggon D & Anthony Newman TA. Coal mining and chronic obstructive pulmonary disease: a review of the evidence. Thorax 1998;53:398–407(PMID:9708233) Cohen RAC, Patel A, Green FHY. Lung disease caused by
exposure to coal mine and silica dust. Semin Respir Crit Care Med 2008;29:651-661(DOI:10.1055/s- 0028-1101275)
Foschino Barbaro MP, Carpagnano GE, Spanevello A, Cagnazzo MG, Barnes PJ. Inflammation, oxidative stress and systemic effects in mild chronic obstructive pulmonary disease. Int J Immunopathol Pharmacol 2007;20(4):753-763(DOI:10.1177/0394 63200702000411)
Fukui T, Yamauchi K, Maruyama M, Yasuda T, Kohno M et al. Significance of measuring oxidative stress in lifestyle-related diseases from the viewpoint of correlation between d-ROMs and BAP in Japanese subjects. Hypertens Res 2011;34(9):1041-1045 (PMID:19403985)
Gan WQ, Man SFP, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax 2004;59:574-580(DOI:10.
1136/thx.2003.019588)
Gao X, Gào X, Zhang Y, Breitling LP, Schöttker B et al.
Associations of self-reported smoking, cotinine levels and epigenetic smoking indicators with oxidative stress among older adults: a population- based study. Eur J Epidemiol 2017;32(5):443-456
(DOI:10.1007/s10654-017-0248-9)
Gulumian M, Borm PJA, Vallyathan, Castranova V, Donaldson K et al. Mechanistically identified suitable biomarkers of exposure, effect, and susceptibility for silicosis and coal-worker's pneumoconiosis: a comprehensive review. J Toxicol Environ Health, Part B 2006;9:357-395(DOI:10.1080/ 152873905 00196537)
Gutteridge JM. Lipid peroxidation and antioxidants as biomarkers of tissue damage. Clin Chem, 1995;
41(12 Pt 2):1819-28(PMID:7497639)
Hanta I, Kocabas A, Canacankatan N, Kuleci S, Seydaoglu G. Oxidant-antioxidant balance in patients with COPD. Lung 2006;184(2):51-55(DOI:10.1007/s00408- 005-2561-4)
Hirose H, Kawabe H, Komiya N, Saito I. Relations between serum reactive oxygen metabolites(ROMs) and various inflammatory and metabolic parameters in a Japanese population. J Atheroscler Thromb 2009;16 (2):77-82(PMID:19403985)
Hnizdo E, Sullivan PA, Bang KM, Wagner G. Association between chronic obstructive pulmonary disease and employment by industry and occupation in the US population: A study of data from the Third National Health and Nutrition Examination Survey. Am J Epidemiol 2002;156(8):738-746(PMID:12370162) Karadag F, Kirdar S, Karul AB, Ceylan E. The value of
C-reactive protein as a marker of systemic inflammation in stable chronic obstructive pulmonary disease. Eur J Intern Med 2008;19(2):104-108(DOI:
10.1016/ j.ejim.2007.04.026)
KATRD(Korean academy of tuberculosis and respiratory diseases). Guideline for COPD and asthma. Seoul:
Seoul Medcus; 2005. p. 26-27
Kirkham PA & Barnes PJ. Oxidative stress in COPD. Chest 2013;144(1):266-27( DOI:10.1378/chest.12-2664) Koechlin C, Couillard A, Cristol JP, Chanez P, Hayot M et
al. Does systemic inflammation trigger local exercise- induced oxidative stress in COPD? Eur Respir J 2004;23(4):538-544(PMID:15083751)
Kostikas K, Papatheodorou G, Psathakis K, Panagou P, Loukides S: Oxidative stress in expired breath condensate of patients with COPD. Chest 2003;
124(4):1373-1380(PMID:14555568)
Larsson K. Aspects on pathophysiological mechanisms in COPD. J Intern Med 2007;262(3):311-340 (DOI:10.1111/j.1365-2796.2007.01837.x)
Lamprecht B, McBurnie MA, Vollmer WM, Gudmundsson
G, Welte T et al. COPD in never smokers: results
from the population-based burden of obstructive
lung disease study. Chest 2011;139(4):752-763
(DOI:10.1378/chest.10-1253)
MacNee W. Pulmonary and systemic oxidant/antioxidant imbalance in chronic obstructive pulmonary disease.
Proc Am Thorac Soc 2005;2(1):50-60(DOI:10.1513/
pats.200411-056SF)
Mak JC. Pathogenesis of COPD. Part II. Oxidative- antioxidative imbalance. Int J Tuberc Lung Dis 2008;12(4):368-374(PMID:18371260)
Markoulis N, Gourgoulianis KI, Moulas A, Gerogianni E, Molyvdas AP. Reactive oxygen metabolites as an index of chronic obstructive pulmonary disease severity. Panminerva Med 2006;48(4):209-213 (PMID:17215792)
Meijers JM, Swaen GM, Slangen JJ. Mortality of Dutch coal miners in relation to pneumoconiosis, chronic obstructive pulmonary disease, and lung function.
Occup Environ Med 1997;54(10):708-713 (PMID:
9404317)
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R et al. Standardisation of spirometry. Eur Respir J 2005;26:319-338(DOI:10.1183/09031936.05.
00034805)
Morimoto M, Satomura S, Hashimoto T, Ito E, Kyotani S.
Oxidative stress measurement and prediction of epileptic seizure in children and adults with severe motor and intellectual disabilities. J Clin Med Res 2016;8(6):437-444(DOI:10.14740/jocmr2534w) Pepys MB & Hirschfield GM. "C-reactive protein: a critical
update". J Clin Invest 2003;111(12):1805-1812 (DOI:10.1172/JCI18921)
Pryor WA. Cigarette smoke radicals and the role of free radicals in chemical carcinogenicity. Environ Health Perspect 1997;105(4):875-882 (DOI:10.1289/ehp.
97105s4875)
Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA et al.
Global initiative for chronic obstructive lung disease.
Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 2007;176(6):532-555(DOI:10.1164/rccm.
200703-456SO)
Rahman I, Swarska E, Henry M, Stolk J, MacNee W. Is there any relationship between plasma antioxidant capacity and lung function in smokers and in patients with chronic obstructive pulmonary disease? Thorax 2000;55(3):189-193(PMID:10679536)
Repine JE, BAST A, Lankhorst I, The Oxidative stress study group. Oxidative stress in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1997;156(2 Pt 1):341-357(DOI:10.1164/ajrccm.
156.2. 9611013)
Schins RPF & Borm PJA. Mechanisms and mediators in coal dust induced toxicity: A review. Am Occup Hyg 1999;43(1):7-33(PMID:10028891)
Sethi JM & Rochester CL. Smoking and chronic obstructive pulmonary disease. Clin Chest Med 2000;21(1):67-86(PMID:10763090)
Singh S, Verma SK, Kumar S, Ahmad MK, Nischal A et al.
Evaluation of oxidative stress and antioxidant status in chronic obstructive pulmonary disease. Scand J Immunol 2017;85(2):130-137(DOI:10.1111/ sji.12498) Stanojkovic I, Kotur-Stevuljevic J, Spasic S, Milenkovic B,
Vujic T et al. Relationship between bone resorption, oxidative stress and inflammation in severe COPD exacerbation. Clin Biochem 2013;46(16-17):1678- 1682(DOI:10.1016/j.clinbiochem.2013.08.003) Strassmann R, Bausch B, Spaar A, Kleijnen J, Braendli O
et al. Smoking cessation interventions in COPD: a network meta-analysis of randomised trials. Eur Respir J 2009;34: 634-640(DOI:10.1183/09031936.
00167708)
Su B, Liu T, Fan H, Chen F, Ding H et al. Inflammatory markers and the risk of chronic obstructive pulmonary disease: A systematic review and meta- analysis. PLoS One 2016;11(4):e0150586 (DOI:
10.1371/journal.pone.0150586)
Sun Y. Free radicals, antioxidant enzymes, and carcinogenesis. Free Radical Biol Med 1990;8:
583-599 (PMID:2193855)
Tkacova R, Kluchova Z, Joppa P, Petrasova D, Molcanyiova A. Systemic inflammation and systemic oxidative stress in patients with acute exacerbations of COPD. Respir Med 2007;101(8):1670-1676 (DOI:
10.1016/j.rmed.2007.03.005)
Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 Report: GOLD executive summary. Eur Respir J 2017; 49: 1700214(DOI:
10.1183/13993003.50214-2017)
<저자정보>
이종성(직업환경연구원 연구위원), 신재훈(직업환경연 구원 책임연구원), 백진이(직업환경연구원 전임연구원), 정지영(동아대학교 박사과정 대학원생), 최병순(직업환경 연구원 원장)