유리비골피부피판을 이용한 두경부 재건 시 CT Angiography를 통한 천공지의 확인
장택진·김은기·최종우
울산대학교 의과대학 서울아산병원 성형외과학교실
Purpose: Fibular osteocutaneous free flap is the procedure of choice for mandibular reconstruction. However, the anatomic consistency and the reliability of the skin paddle have been considered to be questionable and the utilization of the fibular osteocutaneous free flap can be challenging for the inexperienced surgeon. Preoperative computed tomography (CT) angiography can support revolutionary help with the operator design of the fibular osteocutaneous flap. The purpose of this article is to share the valuable experience of support with preoperative CT angiography.
Methods: Three consecutive patients, who needed mandibular reconstruction, were treated with fibular osteocutaneous free flap. Each of the patients had undergone lower extremity CT angiography before the surgery. The CT angiographies were scrupulously investigated to calculate the locations and the tracts of the peroneal artery perforators. We compared the findings of the CT angiography with those of the real operation.
Results: The information about the perforators was sufficiently matched with the findings of the operation. With the use of preoperative CT angiography, we were able to achieve confident performance during operation, shortening of operation time, and fine outcomes with a no flap failure.
Conclusion: The CT angiography of lower extremity can provide reliable information of the perforators of the fibular osteocutaneous free flap.
Keywords: Preoperative CT angiography, Fibular osteocutaneous free flap
Preoperative Identification of Perforator Using CT Angiography in Fibular Osteocutaneous Free Flap Head and Neck Reconstruction
Tack-Jin Chang, Eun Key Kim, Jong Woo Choi
Department of Plastic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
서 론
두경부 종양의 광범위 절제 시 하악골의 결손이 생기는 경우, 이를 재건하기 위해 유리비골피부피판술이 널리 사
용되고 있다. 유리비골피판술은 1975년 Taylor 등1에 의해 처음 소개되었고, Chen과 Yan2이 유리비골피부피판술로 발전시킨 뒤 점차 그 이용이 널리 퍼지게 되었다.3 그러나 유 리비골피부피판술은 요측전완유리피판술이나 전방외측 대퇴유리피판술 등에 비해 피부판의 불안정성이 문제시되 어 왔던 것이 사실이다. 따라서 수술 전에 천공지의 위치 및 경로, 크기 등을 미리 파악할 경우 수술에 큰 도움이 될 수 있으며, 그 동안 해부학과 영상을 통해 이를 파악하기 위한 노력이 이루어져 왔다. Yu 등4이 해부학적인 연구를 통해 유
Correspondence: Eun Key Kim
Department of Plastic Surgery, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea
Tel: +82-2-3010-3600 / Fax: +82-2-476-7471 / E-mail: [email protected] Received February 10, 2012 / Revised March 19, 2012 / Accepted March 20, 2012
Original Article
리비골피부피판의 천공지의 분포를 통계적으로 분석한 것 도 이러한 노력의 일환으로, 천공지 분포 빈도수가 높은 부 위를 A, B, C로 나누었다.한편, 전산화단층촬영 혈관조영 술(computed tomography [CT] angiography)을 이용해 심하 복벽천공지유리피판술이나 전방외측대퇴천공지유리피판 술에서 천공지를 술 전에 미리 파악하려는 노력 또한 여러 문헌을 통해 이뤄지고 있다.5–8 본 논문에서 저자들은 술 전 에 CT angiography를 시행하여 유리비골피부피판의 천공 지의 위치 및 주행경로를 파악함으로써 개별화된 수술 계 획 수립과 실제 혈관 박리 시에 도움을 얻고자 하였다.
재료 및 방법
2011년 3월부터 2011년 12월까지 두경부 종양 절제 및 재 건을 위해 시행한 연속적인 유리비골피부피판술 3례를 대 상으로 하였다. 환자의 평균 나이는 54.7세였고 이들 세 명 은 모두 수술 전 검사로 하지 CT angiography를 시행하였 다. CT angiography 촬영은 SOMATOM Sensation 16 또는 SOMATOM Definition 64 (Siemens Medical Solutions, Er- langen, Germany)를 이용하여, AEC 모드, CARE Dose4D, 120 kV, 200 effective mAs, 0.5 Rotation time, 0.95 pitch, 16 (detector rows)×1.5 (collimation), slice thickness 3 mm, ma- trix 512 × 512로 촬영하였다. 조영제는 정주용 Iopamidol 조 영제(Pamiray 370, Dongkuk Pharm., Seoul, Korea) 140 ml를 주사하고 100 Hounsefield unit로 추적하여 동맥기와 3분 지연기 검사를 시행하였다. 3차원 영상 재구성에 의존하지 않고 2차원 CT 영상자료를 주로 참고하였다. 비골 골두와
외측 복사를 기준점으로 잡고 axial image를 연속적으로 넘 겨보아 CT 촬영 절편의 두께와 image number로부터 수직 방향의 위치를 계산할 수 있으며, 수평적인 위치는 posteri- or septum을 기준으로 이의 anatomic landmark (비골골두 와 외측복사를 잇는 선상의 뒤쪽 1–2 cm)로부터 어렵지 않 게 찾을 수 있었다. 이렇게 천공지의 3차원적인 위치를 찾 은 뒤에는 이를 Doppler로 확인하였다. 수술장에서는 상기 한 방법으로 찾아둔 천공지를 바탕으로 피판을 디자인하 여 거상하였고, 천공지의 수평적 위치는 우선 피판의 한 쪽 에 절개선을 넣은 후에는 posterior septum을 직접 눈으로 확인할 수 있어 더욱 정확성을 기할 수 있었다.
결 과
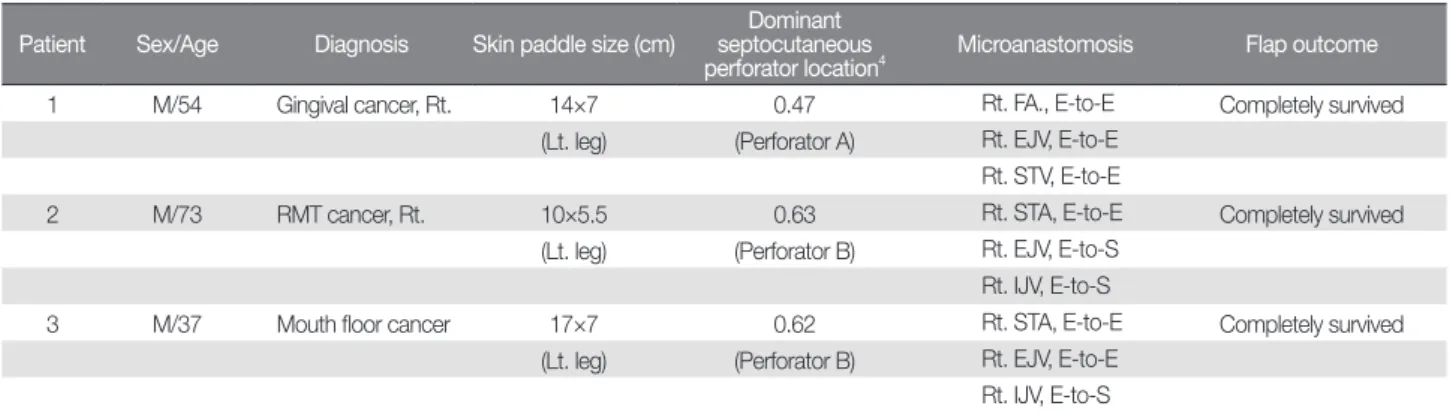
환자들은 모두 두경부 종양으로 일차수술을 받았으며, 수술 후 방사선치료를 받았다. 평균 관찰기간은 6.7개월(범 위, 5–8개월)이었다(Table I).
세 명의 환자 모두에서 하지 CT angiography를 통해 비 골피부피판의 격막(septocutaneous) 타입의 천공지를 찾을 수 있었고(Fig. 1), 이는 Doppler와 실제 수술장에서도 확인 할 수 있었다.
1.
증례 1) 환자 273세의 남자 환자로, 우측 구치후삼각부위의 편평상피 암을 진단받고 이비인후과에서 광범위절제술 및 부분 하
Table I. Patients’ Demographics
Patient Sex/Age Diagnosis Skin paddle size (cm) Dominant septocutaneous
perforator location
4Microanastomosis Flap outcome
1 M/54 Gingival cancer, Rt. 14×7 0.47 Rt. FA., E-to-E Completely survived
(Lt. leg) (Perforator A) Rt. EJV, E-to-E Rt. STV, E-to-E
2 M/73 RMT cancer, Rt. 10×5.5 0.63 Rt. STA, E-to-E Completely survived
(Lt. leg) (Perforator B) Rt. EJV, E-to-S Rt. IJV, E-to-S
3 M/37 Mouth floor cancer 17×7 0.62 Rt. STA, E-to-E Completely survived
(Lt. leg) (Perforator B) Rt. EJV, E-to-E Rt. IJV, E-to-S
RMT, retromolar trigone; FA, facial artery; E-to-E, end to end; EJV, external jugular vein; E-to-S, end to side; IJV, internal jugular vein; STA, superior thyroidal
artery; STV, superior thyroidal vein.
악골절제술과 우측 변형근치적경부곽청술(modified radical neck dissection), 좌측 견갑설골근상부경부곽청술(suprao- mohyoid neck dissection)을 시행받았다. 수술 전 환자는 하 지 CT angiography를 찍었고, 이를 바탕으로 유리비골피부 피판술에 사용할 천공지를 찾아두었다. 수술장에서 Dop- pler를 통해 미리 찾아두었던 천공지를 확인한 후, 10×5.5 cm 크기의 skin paddle을 디자인하였다. 피판을 거상하면서 표 시해둔 천공지를 근육사이격막에서 찾아 이를 박리하고 비 골을 8 cm 길이로 잘라 피판에 포함시켰다. 천공지는 비골 동맥의 근위부에서 분지하여 격막을 따라 비스듬하게 주행 하는 것을 확인할 수 있었고, 이는 CT angiography를 통해 수술 전 미리 확인했던 것과 일치하였다(Figs. 2–5).
고 찰
심하복벽천공지유리피판술이나 전방외측대퇴천공지유 리피판술의 경우5–8 CT angiography를 이용하여 수술 전 사 용할 피판의 천공지를 미리 파악해둘 경우, 술자는 보다 수 술을 편하게 시행할 수 있으며, 특히 경험이 적은 술자에게 큰 도움을 줄 수 있다. 또한 수술시간을 줄일 수 있고, 수술 을 예측 가능하게 해준다.
이러한 사실은 유리비골피부피판술의 경우에도 마찬가 지여서 유리 피판술을 시행하기에 앞서 실제 이용할 천공 지를 파악하고자 하는 노력들이 이루어지고 있다. 기존에 수술 전 angiography를 촬영했던 것은 수술 후 피판 공여부 의 이환율을 줄이고자하는 것이 주된 이유였으나,9,10 최근 영상기법의 발달로 천공지를 미리 확인하고자 하는 시도 가 이루어지고 있다. 그러나 이러한 노력들은 대개 magnetic resonance angiography를 이용하는 경우가 많았으며, CT angiography를 이용하는 경우에도 3차원으로 영상을 재구 성하여 천공지의 위치를 파악하는 것이었다.11–16 본 저자들 은 2011년 한 해 동안 시행했던 연속적인 유리비골피부피 판술 3례를 고찰해 본 결과, 3차원 영상 재구성에 의존하지 않고 2차원 하지 CT angiography를 분석해봄으로써 비골 동맥으로부터 분지되어 나오는 천공지를 찾을 수 있었으며 상당히 정확히 수술 전에 위치를 확인할 수 있었다. 이와 더 불어, 본 연구에 포함됐던 3명의 환자 모두에서 비골피판의 거상 시 격막타입의 천공지가 “distal perforators”4에 속함을 확인하였다. 다만 비골동맥의 천공지는 심하복벽동맥 천공
Fig. 2. (Left) Perforators marked based on the preoperative CT angiography. (Right) Operative finding of the perforators.
Fig. 1. (Left) CT angiography of the patient 2. (Right) The part indi-
cated with red box is zoomed. The arrows are indicating the septocu-
taneous perforators of the peroneal artery. The relative locations
4of
the perforators was 0.63.
지나 전방외측대퇴피판 천공지에 비하여 angiography의 소 견이 비교적 덜 뚜렷하게 나타나는 경향이 있었으며 이는 피하지방의 두께가 얇은8 두경부종양 환자에서 더욱 그러 하였다. 천공지가 근막을 뚫고 나오는 cut이 분명히 확인되 지 않는 경우 통계적으로 천공지가 흔히 발견되는 부분16에
서 연속된 3–4개의 axial cut image를 연속적으로 보며 격막 이 갈라진 양상, 피하지방이 갈라진 양상 등을 확인하는 것 이 도움이 되었다.
결 론
유리비골피부피판술을 이용한 두경부 재건 시 수술 전 하지 CT angiography를 통하여 천공지 위치와 주행을 파악 하고 수술 계획을 수립하는데 도움을 받을 수 있다.