Received:November 13, 2017, Revised:March 14, 2018, Accepted:March 28, 2018 Corresponding to:Chang-Hee Suh http://orcid.org/0000-0001-6156-393X
Department of Rheumatology, Ajou University School of Medicine, 164 WorldCup-ro, Yeongtong-gu, Suwon 16499, Korea.
E-mail:[email protected]
Copyright ⓒ 2018 by The Korean College of Rheumatology. All rights reserved.
This is a Open Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
Pulmonary Hypertension in Connective Tissue Disease is Associated with the New York Heart Association Functional Class and Forced Vital Capacity, But Not with Interstitial Lung Disease
Ju-Yang Jung1, Chan Hee Lee2, Hyoun-Ah Kim1, Sang Tae Choi3, Joo-Hyun Lee4, Bo-Young Yoon4, Dae-Ryong Kang5, Chang-Hee Suh1
1Department of Rheumatology, Ajou University School of Medicine, Suwon, 2Department of Rheumatology, National Health Insurance Service Ilsan Hospital, Goyang, 3Department of Rheumatology, Chung-Ang University College of Medicine, Seoul, 4Division of Rheumatology, Department of Internal Medicine, Inje University Ilsan Paik Hospital, Goyang, 5Department of Medical Humanities and Social Medicine, Office of Biostatistics, Ajou University School of Medicine, Suwon, Korea
Objective. Pulmonary hypertension (PH) develops frequently in connective tissue diseases (CTD) and is an important prog- nostic factor. The aim of this study was to assess the prevalence of PH in patients with CTD by non-invasive echocardiography and analyze the potential biomarkers for helping to detect PH. Methods. All Korean patients with CTD who had dyspnea on exertion or interstitial lung disease (ILD) were screened for PH with echocardiography and clinical data were collected from four hospitals. Results. Among 196 patients with CTD, 108 (55.1%) had ILD and 21 had PH defined as >40 mmHg. Of the 21 patients with PH, 10, 4, and 3 patients had systemic sclerosis, systemic lupus erythematosus, and mixed connective tissue dis- ease, respectively. There was no difference in the incidence of PH according to the presence of ILD; 12 patients (11.1%) with ILD had PH and 9 patients (10.2%) without ILD had PH. The results of the pulmonary function test, total cholesterol, red cell volume distribution width, alkaline phosphatase, and the New York Heart Association (NYHA) functional class III or IV differed significantly according to the presence of PH. In multiple regression analysis, NYHA functional class III or IV (odd ratio [OR]=7.3, p=0.009) and forced vital capacity (OR=0.97, p=0.043) were independent predictive factors of PH. Conclusion.
PH is not associated with the presence of ILD in Korean patients with CTD. On the other hand, NYHA functional class III or IV and decreased forced vital capacity indicate the presence of PH in connective tissue disease. (J Rheum Dis 2018;25:179-187)
Key Words. Connective tissue disease, Pulmonary hypertension, Echocardiography, Interstitial lung disease, Risk factors
INTRODUCTION
Pulmonary hypertension (PH) is one of serious manifes- tations in connective tissue diseases (CTD) including sys- temic sclerosis (SSc), systemic lupus erythematosus (SLE), mixed connective tissue disease (MCTD) and rheumatoid arthritis (RA) [1]. PH is defined as an in- crease of resting mean pulmonary artery pressure (PAP)
>25 mmHg with normal pulmonary capillary wedge pressure [2]. PH is characterized by medial hypertrophy,
intimal proliferative and fibrotic changes, and adventitial thickening with perivascular inflammatory infiltrates.
CTD-associated PH is known to have different features in accordance with the types of CTD and poorer outcome compared with idiopathic PH [3]. In SSc-associated PH, profibrotic cytokines such as transforming growth factor-β play a role in leading to obliterative vasculopathy, and its prognosis is reported more aggressive than in that of idio- pathic PH [4,5].
In CTD, interstitial lung disease (ILD) and PH are the
main manifestations involving the pulmonary system and the symptoms of these two diseases are similar. Chronic lung diseases including pulmonary fibrosis lead to the el- evation of pulmonary artery pressure and right heart fail- ure [6]. CTD-associated PH is known to originate, by dif- ferent pathogenesis, from PH due to lung disease in which hypoxia induces vascular change [7]. In CTD-asso- ciated PH, autoimmune response mediates vascular hy- pertrophy and fibrosis in pulmonary artery and it ad- vances to a status without hypoxia. Consequently, CTD- associated PH has been reported to develop similarly in patients with ILD and those without, and acts as a major mortality factor independent of ILD [8,9].
The manifestations of PH are nonspecific as dyspnea with exertion, lower extremities edema, fatigue and palpitation. Usually, a patient may not feel anything until PAP highly increases [10]. There is no specific biomarker representing elevated PAP. Unless the physicians pay an attention to a possibility of pulmonary vasculature in- volvement, the diagnosis of PH might be delayed.
Recently, the new treatments for PH have been known ef- fective, so the timely detection and early intervention has been more important [5,11].
Echocardiography is a convenient and useful test to esti- mate a peak tricuspid regurgitation velocity (TRV) and pulmonary artery systolic pressure (PASP) in screening PH and to identify possible cardiac etiology [2,11-13]. In the patients with CTD having cardiac symptoms, echo- cardiography can provide essential information about the conditions that predispose to PH including pericardial ef- fusion and left sided valve changes [1,14]. Right heart catheterization (RHC) is recommended because it can confirm the diagnosis of PH as a more accurate and reli- able examination, assess the severity and test the vaso- reactivity of the pulmonary circulation [1,2,14,15].
However, RHC is an invasive procedure that can result in some complications including hemorrhage and hema- toma, with a nearly 1% incidence [16]. It is difficult to take the risk of complication for the purpose of diagnosis, as many patients with CTD have a poor condition with complicated medications. A gap between the recom- mendation and the clinical practice of rheumatologist was reported to exist in the diagnosis of CTD-associated PH [17]. In Korean registry report, a number of patients received a diagnosis of PAH on the basis of only echo- cardiography because the frequency of RHC was low [18,19]. Moreover, pulmonary vascular resistance esti- mated by echocardiography was shown to closely corre-
late with that evaluated by RHC in patients with a forced vital capacity (FVC)/lung diffusion capacity for carbon monoxide (DLCO) ratio >1.6, which means that echo- cardiography can be a reliable marker in identifying PH noninvasively [20]. Moreover, PASP measured by using echocardiography was revealed to be associated with mortality regardless of the results of RHC [21].
Therefore, we aimed to investigate the possibility for PH by using echocardiography when a CTD patient has dysp- nea on exertion or known ILD. In addition, we determined potential biomarkers of PH in patients with CTD.
MATERIALS AND METHODS
Study population and data collection
In Ajou University Hospital, National Health Insurance Service Ilsan Hospital, Chung-Ang University Hospital, Inje University Ilsan Paik Hospital, from February 2011 to October 2013, patients with CTD who had dyspnea on ex- ertion were enrolled. The patients were diagnosed CTD by the established classification criteria of each disease such as SSc by Classification criteria for SSc: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative at 2013, SLE by Systemic Lupus International Collaborating Clinics Classification Criteria for SLE at 2012 and RA by 2010 RA classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative [22-24]. Moreover, CTD patients who had ILD confirmed with chest high-resolution com- puter tomography (HRCT) were included irrespective of symptoms. All of them underwent transthoracic echo- cardiography, and most patients took pulmonary function test (PFT) with DLCO except for a few patients who could not exhale enough for the measurement. The medical re- cords and laboratory results of aspartate amino- transferase, alanine aminotransferase, total cholesterol, red cell volume distribution width (RDW), alkaline phos- phatase (ALP) and uric acid were collected. Symptom of dyspnea was described according to New York Heart Association (NYHA) functional classification.
Measurements
Echocardiography was performed at each hospital by skillful examiners. PASP was calculated from maximal tri- cuspid regurgitation velocity (TRVmax) using the sim- plified Bernoulli formula as follows: PASP=4×(TRVmax) 2+right atrial pressure (calculated with 5 mmHg as nor-
Table 1. The clinical characteristics of patients (n=196)
Clinical factor Value
Age (yr) 54.8±14.7
Gender, female:male 150:46
Disease duration (mo) 43.2±52.8 Interstitial lung disease 108 (55.1) Disease
Systemic sclerosis 62 (31.6)
Rheumatoid arthritis 54 (27.6) Systemic lupus erythematosus 43 (21.9)
Myositis 16 (8.2)
Mixed connective tissue disease 7 (3.6)
Others 14 (7.1)
NYHA functional class
I 75 (38.3)
II 105 (53.6)
III 15 (7.7)
IV 1 (0.5)
Mortality 4 (2.0)
Echocardiographic finding
TRV (m/s) 2.49±0.43
PASP (mmHg) 30.5±9.8
PFT finding (%)
DLCO 67.4±22.4
FVC 82.9±21.7
FEV1 87.0±23.2
FVC/DLCO 1.32±0.34
Laboratory finding
RDW (%) 14.4±2.1
AST (U/L) 33.8±51.4
ALT (U/L) 25.8±42.2
Total cholesterol (mg/dL) 177.1±44.4
ALP (U/L) 69.7±31.7
Uric acid (mg/dL) 4.5±1.4
Medication
Corticosteroid 135 (68.9)
Hydroxychloroquine 77 (39.3)
Azathioprine 37 (18.9)
Methotrexate 32 (16.3)
Penicillamine 13 (6.6)
Bucillamine 27 (13.8)
Sulfasalazine 14 (7.1)
Tacrolimus 26 (13.3)
Cyclophosphamide 20 (10.2)
Calcium channel blocker 34 (17.3) Endothelial receptor antagonist 9 (4.6) Prostacyclin analogues 6 (3.1)
Values are presented as mean±standard deviation, number only or number (%).
NYHA: New York Heart Association, TRV: tricuspid regurgitation velocity, PASP: pulmonary artery systolic pressure, PFT:
pulmonary function test, DLCO: lung diffusion capacity for carbon monoxide, FVC: forced vital capacity, FEV1: forced expired volume in one second, RDW: red cell volume distribution width, AST: aspartate aminotransferase, ALT:
alanine aminotransferase, ALP: alkaline phosphatase.
mal) [25]. This study was approved by the institutional review board of each hospital and informed consent was obtained from each patient (IRB no. AJIRB-MED-MDB- 10-330).
Statistical analysis
Group comparisons divided by the presence of PH and ILD were conducted by using independent t-tests for con- tinuous data and the Mann-Whitney U-test for non- parametric data. Logistic regression analysis was per- formed to determine the variables associated with an in- creased risk for PH. Univariate regression analysis was conducted with age, sex, the presence of ILD, DLCO, FVC, forced expired volume in one second (FEV1), aspar- tate aminotransferase, alanine aminotransferase, total cholesterol, RDW, ALP, uric acid and NYHA functional class (FC) III or IV as independent variables. Six variables had statistical significance, and those were adjusted in multivariate analysis. In Hosmer-Lemeshow good- ness-of-fit statistic, their p-value was 0.872, and their var- iance inflation factors showed they had no multicoll- inearity. A two-tailed p-value <0.05 was used to indicate statistically significant differences. All computations were performed using the SPSS statistics version 22.0 (IBM Co., Armonk, NY, USA) and MedCalc version 14.10.2 (MedCalc software, Ostend, Belgium).
RESULTS
Clinical characteristics of patients with CTD One-hundred ninety-six patients were recruited (female, 150 patients), with a mean age was 54.8±14.7 years and mean disease durations of 43.2±52.8 months (Table 1).
The common underlying diseases were SSc in 62 patients, RA in 54 patients, and SLE in 43 patients. The mean TRV was 2.49±0.43 m/sec and estimated PASP was 30.5±9.8 mmHg. One-hundred eight patients had ILD that was confirmed by HRCT or lung biopsy. The FVC, FEV1 and DLCO were 82.9±21.7%, 87.0±23.2% and 67.4±22.4%, respectively. Most patients (180/196, 91.8%) felt mild symptom of dyspnea such as NYHA FC I or II, 15 patients were NYHA FC III and 1 patient was NYHA FC IV.
One-hundred thirty-seven patients were taking gluco- corticoids, 77 were taking hydroxychloroquine and 37 were taking azathioprine. As the treatment for PH, 9 pa- tients were taking endothelial receptor antagonists and 6 patients were taking prostacyclin analogue. During 32 months, the period of this study conducted, four patients
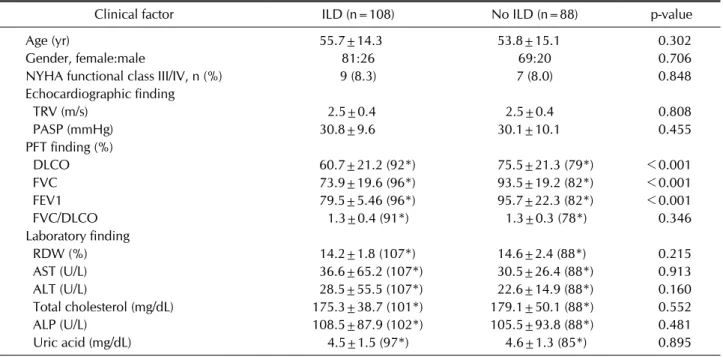
Table 2. The comparison of the patients with ILD and those without
Clinical factor ILD (n=108) No ILD (n=88) p-value
Age (yr) 55.7±14.3 53.8±15.1 0.302
Gender, female:male 81:26 69:20 0.706
NYHA functional class III/IV, n (%) 9 (8.3) 7 (8.0) 0.848
Echocardiographic finding
TRV (m/s) 2.5±0.4 2.5±0.4 0.808
PASP (mmHg) 30.8±9.6 30.1±10.1 0.455
PFT finding (%)
DLCO 60.7±21.2 (92*) 75.5±21.3 (79*) <0.001
FVC 73.9±19.6 (96*) 93.5±19.2 (82*) <0.001
FEV1 79.5±5.46 (96*) 95.7±22.3 (82*) <0.001
FVC/DLCO 1.3±0.4 (91*) 1.3±0.3 (78*) 0.346
Laboratory finding
RDW (%) 14.2±1.8 (107*) 14.6±2.4 (88*) 0.215
AST (U/L) 36.6±65.2 (107*) 30.5±26.4 (88*) 0.913
ALT (U/L) 28.5±55.5 (107*) 22.6±14.9 (88*) 0.160
Total cholesterol (mg/dL) 175.3±38.7 (101*) 179.1±50.1 (88*) 0.552
ALP (U/L) 108.5±87.9 (102*) 105.5±93.8 (88*) 0.481
Uric acid (mg/dL) 4.5±1.5 (97*) 4.6±1.3 (85*) 0.895
Values are presented as mean±standard deviation, number only or number (%).
ILD: interstitial lung disease, NYHA: New York Heart Association, TRV: tricuspid regurgitation velocity, PASP: pulmonary artery systolic pressure, PFT: pulmonary function test, DLCO: lung diffusion capacity for carbon monoxide, FVC: forced vital capacity, FEV1: forced expired volume in one second, RDW: red cell volume distribution width, AST: aspartate aminotransferase, ALT:
alanine aminotransferase, ALP: alkaline phosphatase. *The number of patients tested.
Table 3. The prevalence of increased PASP according to ILD pattern in CTD
ILD pattern Total (n=108) PH (n=12)
Usual interstitial pneumonia 42 5 (11.9)
Nonspecific interstitial pneumonia 36 5 (13.9)
Undifferentiated interstitial lung disease 21 1 (4.8)
Bronchiolitis obliterans organizing pneumonia 9 1 (11.1)
Values are presented as number only or number (%).
PASP: pulmonary artery systolic pressure, ILD: interstitial lung disease, CTD: connective tissue disease, PH: pulmonary hypertension, pulmonary artery systolic pressure >40 mmHg.
died and two of them had PH. The causes of deaths were respiratory failure due to aggravation of ILD (two pa- tients), sepsis (one patient) and cardiogenic shock due to progressed aplastic anemia (one patient).
Comparison of ILD and non-ILD patients
Among 196 patients with CTD, 108 patients (55.1%) had ILD which confirmed by HRCT or lung biopsy (Table 2). There was no difference in the incidence of patients with PH according to the presence of ILD; in the patients with ILD, 12 patients had PH (12/108, 11.1%), and in those without ILD, 9 patients had PH (9/88, 10.2%).
Between the two groups which divided according to the
presence of ILD, the patients’ age, sex, TRV and PASP were not different; however, FVC, FEV1 and DLCO showed significant differences (Table 2). In addition, oth- er clinical variables including RDW, liver function, total cholesterol, uric acid and NYHA FC were similar. Usual interstitial pneumonia was most common with 42 pa- tients, followed by nonspecific interstitial pneumonia was following with 36 patients (Table 3).
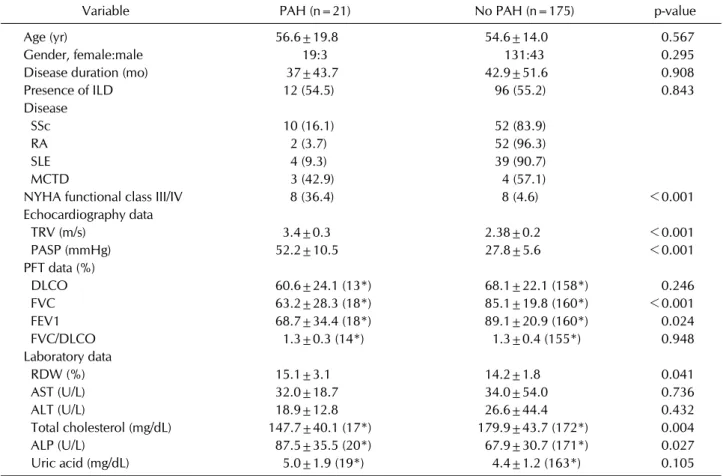
Clinical characteristics of patients with PH With the defining PH as estimated PASP >40 mmHg measured by echocardiography, 21 patients were de- termined to have PH with mean PASP 52.2±10.5 mmHg
Table 4. The clinical characteristics in the patients with PAH
Variable PAH (n=21) No PAH (n=175) p-value
Age (yr) 56.6±19.8 54.6±14.0 0.567
Gender, female:male 19:3 131:43 0.295
Disease duration (mo) 37±43.7 42.9±51.6 0.908
Presence of ILD 12 (54.5) 96 (55.2) 0.843
Disease
SSc 10 (16.1) 52 (83.9)
RA 2 (3.7) 52 (96.3)
SLE 4 (9.3) 39 (90.7)
MCTD 3 (42.9) 4 (57.1)
NYHA functional class III/IV 8 (36.4) 8 (4.6) <0.001
Echocardiography data
TRV (m/s) 3.4±0.3 2.38±0.2 <0.001
PASP (mmHg) 52.2±10.5 27.8±5.6 <0.001
PFT data (%)
DLCO 60.6±24.1 (13*) 68.1±22.1 (158*) 0.246
FVC 63.2±28.3 (18*) 85.1±19.8 (160*) <0.001
FEV1 68.7±34.4 (18*) 89.1±20.9 (160*) 0.024
FVC/DLCO 1.3±0.3 (14*) 1.3±0.4 (155*) 0.948
Laboratory data
RDW (%) 15.1±3.1 14.2±1.8 0.041
AST (U/L) 32.0±18.7 34.0±54.0 0.736
ALT (U/L) 18.9±12.8 26.6±44.4 0.432
Total cholesterol (mg/dL) 147.7±40.1 (17*) 179.9±43.7 (172*) 0.004
ALP (U/L) 87.5±35.5 (20*) 67.9±30.7 (171*) 0.027
Uric acid (mg/dL) 5.0±1.9 (19*) 4.4±1.2 (163*) 0.105
Values are presented as mean±standard deviation, number only or number (%).
PAH: pulmonary arterial hypertension, ILD: interstitial lung disease, SSc: systemic sclerosis, RA: rheumatoid arthritis, SLE: systemic lupus erythematosus, MCTD: mixed connective tissue disease, NYHA: New York Heart Association, TRV: tricuspid regurgitation velocity, PASP: pulmonary artery systolic pressure, PFT: pulmonary function test, DLCO: lung diffusion capacity for carbon monoxide, FVC: forced vital capacity, FEV1: forced expired volume in one second, RDW: red cell volume distribution width, AST:
aspartate aminotransferase, ALT: alanine aminotransferase, ALP: alkaline phosphatase. Pulmonary hypertension: pulmonary artery systolic pressure >40 mmHg. *The number of patients tested.
(Table 4). Among the patients with PH, 10 had SSc, 4 had SLE and 3 had MCTD. There was no difference in the age, sex, disease duration and presence of ILD between pa- tients with PH and those without. More than one-third of patients with PH had functional limitation due to dysp- nea (NYHA FC III or IV), which was significantly more severe than those without PH (8 [36.4%] vs. 8 [4.6%], p<
0.001). While the values of DLCO were a little different between these patients, FVC and FEV1 were significantly lower in patients with PH (63.2±28.3% vs. 85.1±19.8%, p<0.001; 68.7±34.4% vs. 89.1±20.9%, p=0.024, re- spectively). From a previous study, a FVC/DLCO ratio of
>1.6 was reported to be a diagnostic marker for PH in SSc [24], but it was not related with PH in this study. RDW means a variability in the size of circulating red blood cells and RDW was higher in the patients with PH than in
those without (15.1±3.1% vs. 14.2±1.8%, p=0.041).
Patients with PH had significantly lower total cholesterol than those without (147.7±40.1 mg/dL vs. 179.9±43.7 mg/dL, p=0.004). The level of ALP in patients with PH was significantly more elevated (87.5±35.5 U/L vs.
67.9±30.7 U/L, p=0.027).
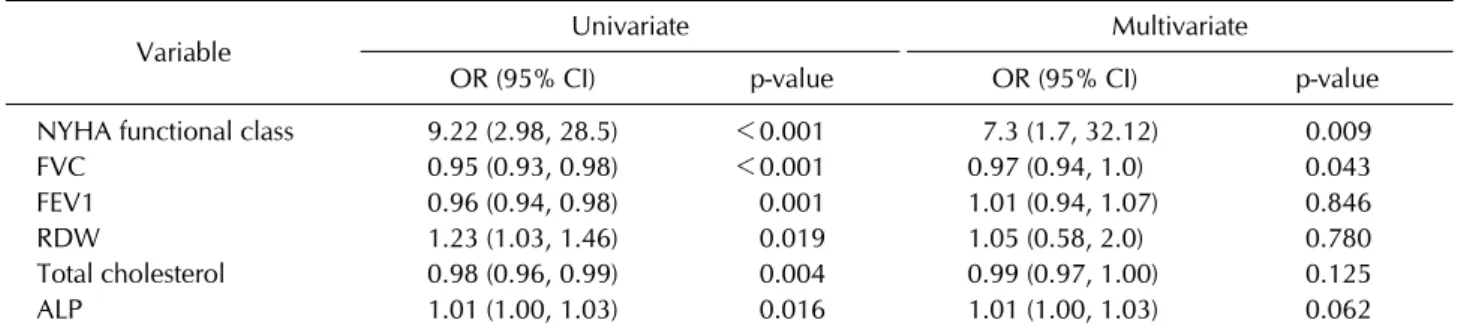
Predictors of PH development in patients with CTD
On univariate regression analysis with the variables which were different between CTD patients with PH and those not, NYHA FC III/IV, FVC, FEV1, RDW, total cho- lesterol and ALP were correlated with the presence of PH in CTD (Table 5). On multiple regression analysis, NYHA FC III or IV (odds ratio [OR]=7.3, p=0.009) and FVC (OR=0.97, p=0.043) were found to be related with PH.
Table 5. The logistic regression analysis for PAH in connective tissue disease
Variable Univariate Multivariate
OR (95% CI) p-value OR (95% CI) p-value
NYHA functional class 9.22 (2.98, 28.5) <0.001 7.3 (1.7, 32.12) 0.009
FVC 0.95 (0.93, 0.98) <0.001 0.97 (0.94, 1.0) 0.043
FEV1 0.96 (0.94, 0.98) 0.001 1.01 (0.94, 1.07) 0.846
RDW 1.23 (1.03, 1.46) 0.019 1.05 (0.58, 2.0) 0.780
Total cholesterol 0.98 (0.96, 0.99) 0.004 0.99 (0.97, 1.00) 0.125
ALP 1.01 (1.00, 1.03) 0.016 1.01 (1.00, 1.03) 0.062
PAH: pulmonary arterial hypertension, OR: odds ratio, CI: confidence interval, NYHA: New York Heart Association, FVC: forced vital capacity, FEV1: forced expired volume in one second, RDW: red cell volume distribution width, ALP: alkaline phosphatase.
Figure 1. Receiver operating characteristic to predict pulmo- nary hypertension by echocardiography in connective tissue disease. The area under curve (AUC) of receiver operating characteristic by final model with New York Heart Association functional class III or IV and forced vital capacity was 0.767.
Area under curve (AUC) of receiver operating character- istic determined by NYHA FC III or IV and FVC was 0.767 (Figure 1).
DISCUSSION
This is an observational study that investigated the clin- ical features of PH among patients with CTD in Korea and the purpose was to determine the characteristics of CTD patients with PH.
We defined PH as PASP >40 mmHg on echo- cardiography. PH was categorized as moderate if PASP is
>55 mmHg and mild if PASP is 40 to 54 mmHg [26]. In addition, echocardiographic TRV ≥3 m/sec and/or PASP
≥40 mmHg were used as thresholds indicating possible PH [27]. While some studies defined possible PH if a PASP was >35 mmHg, PASP >40 mmHg as definition of PH
was more reliable in a study conducted without RHC [28].
PH is combined 7%∼27% in patients with SSc, which is characterized by the presence of vasculopathy and fib- rosis of multiple organs due to autoimmune imbalance [29]. With lung fibrosis, PH is a typical disorder with lung involvement and a poor prognostic factor with higher mortality in patients with SSc. SSc-associated PH seems to be more aggressive and shows poorer outcomes than idiopathic PH or other CTD-associated PH [3]. In pa- tients with SLE, the prevalence of PH was reported with variety from 0.5% to 14% [30], although PH is not com- mon compared with other manifestations. Although SLE was recently reported the most common underline dis- ease in Chinese patients with CTD associated PH [31], our study showed similar prevalence (9.3%) to western data. PH is known to be rare in patients with RA; how- ever, the mean pulmonary artery pressures measured by echocardiography were reported to be elevated and the prevalence of PH was higher in the patients with RA than in healthy controls (21% vs. 4%, respectively) [32]. In this study, 2 of 52 patients with RA had PH, and the devel- opment of PH in patients with RA was lower than in those with SSc, SLE or MCTD. MCTD is an autoantibody (anti- ribonucleoproteins (RNP) antibody)-mediated disease with Raynaud’s phenomenon, arthritis, sclerotic change of skin, serositis, myositis and pulmonary fibrosis.
Although MCTD is a rare disease and is almost impos- sible to study because the small number of cases, the prevalence of PAH had been estimated as 50%∼60%
[10]. In this study, seven patients with MCTD were en- rolled and four of them had PH. We suggest performing echocardiography frequently in patients with MCTD.
PFT is a basic diagnostic tool that determines the type of pathophysiology of lung disease, e.g. the presence or ab- sence of an obstructive or a restrictive pattern, and PFT
with DLCO has been used in diagnosis of and monitoring for ILD and PH [33]. On the basis of the change of the al- veolar capillary membrane and ventilation/perfusion ra- tio, DLCO was reported to be decreased in CTD-asso- ciated PH, especially in SSc [34]. DLCO was reported as a most reliable marker for progression of PAH in SSc, and FVC/DLCO >1.6 was suggested as a useful marker in the diagnosis of PH in patients with SSc [26], but it was not different according to the presence of PH among our pa- tients with CTD and SSc. DLCO was not different, but FVC and FEV1 were significantly different in the patients with PH compared to those not. In addition, low FVC was associated independently with the presence of PH in pa- tients with CTD, while FEV1 was not.
NYHA FC was originally developed for evaluation of car- diac disease and it was adopted to access the limitation of physical activity of PH by the World Health Organization.
Despite the sizeable interrater variation in the NYHA FC, studies showed that patients with FC III or IV had a worse prognosis than those with FC I or II [35,36]. Further- more, NYHA FC is a key predictor of diagnosis for PH and regulatory approval of PH therapy [37]. In the present study, more than one-third of patients with PH had NYHA FC III or IV, which was significantly more frequent than those without PH. In addition, NYHA FC III or IV was independently associated with PH.
RDW is a quantitative measure of the variability in size of the circulating erythrocytes and it becomes elevated when ineffective red cells are produced. The tentative mechanisms between RDW and such heart problems are anemia from poor circulation, inflammatory stress, nutri- tional deficiencies and insufficient production of eryth- ropoietin [38]. RDW was increased in chronic throm- boembolic pulmonary hypertension and was identified to reflect poor prognosis in patients with PH [39]. In here, RDW was elevated in patients with PH than those not.
ALP is synthesized in liver and bone, and its elevation is predominantly due to its increased synthesis in hep- atocyte and consequent release into circulation in extra- hepatic biliary obstruction. ALP and γ–glutamyl trans- ferase was increased in patients with PH, and it may be caused by cardiac congestion and elevated right atrial pressure [40]. In CTD associated PH, ALP was reported as a predictor for mortality [32]. Significantly elevated ALP was noted in patients with PH, but not associated with PH independently.
Combination of NYHA FC III or IV and FVC were re- garded as a reliable predictive marker for PH in CTD
(AUC=0.767). Although NYHA functional classification is a marker including subjective part in defining dyspnea, the symptom severities of patients with NYHA III or IV will be different those with NYHA I or II. During fol- low-up, aggravated dyspnea and reduction of FVC in pa- tients with CTD might suggest development of PAH re- gardless of DLCO or ILD.
In this study, there was no difference between the pa- tients with ILD and those without in terms of the devel- opment of PH. A study with large number of the patients with CTD associated PH (n=641) showed that an accom- panying mild ILD on HRCT was more frequent in patients with CTD than in patients with idiopathic PH [3]; how- ever, the correlation of ILD and PH in patients with CTD was not analyzed. The relation between ILD and PH in pa- tients with CTD has been rarely studied, and our data show that PH in CTD may occur independent of ILD. The patients with CTD should be checked for the presence of PH even if they do not have ILD.
This study has several limitations. PH was not diag- nosed in current practical recommendation, most of pa- tients were diagnosed PH by echocardiography without confirmation with RHC. The reports demonstrated the estimated pulmonary pressure by echocardiography was correlated with that measured by RHC and associated with mortality [13,19,20]. The small sample size of each CTD made it impossible to identify more characteristics according to each disease. We hope to conduct a pro- spective study with RHC in Korean patients with CTD in near future.
CONCLUSION
Among total 196 patients with CTD, 21 patients had a diagnosis of CTD-associated PH, which was defined as a PASP >40 mmHg measured by echocardiography. There was no difference in the prevalence of PH in CTD patients with ILD and those without. NYHA FC III or IV and de- creased forced vital capacity suggested the presence of PH in connective tissue disease (76.7%).
ACKNOWLEDGMENTS
We gratefully acknowledge the contribution of Handok for research funding and the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant no.
HI14C1731 and HI16C0992).
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Khanna D, Gladue H, Channick R, Chung L, Distler O, Furst DE, et al. Recommendations for screening and detection of connective tissue disease-associated pulmonary arterial hypertension. Arthritis Rheum 2013;65:3194-201.
2. Task Force for Diagnosis and Treatment of Pulmonary Hypertension of European Society of Cardiology (ESC);
European Respiratory Society (ERS); International Society of Heart and Lung Transplantation (ISHLT), Galiè N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J 2009;34:1219-63.
3. Chung L, Liu J, Parsons L, Hassoun PM, McGoon M, Badesch DB, et al. Characterization of connective tissue dis- ease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest 2010;138:1383-94.
4. Shahane A. Pulmonary hypertension in rheumatic diseases:
epidemiology and pathogenesis. Rheumatol Int 2013;33:
1655-67.
5. Vachiéry JL, Coghlan G. Screening for pulmonary arterial hypertension in systemic sclerosis. Eur Respir Rev 2009;
18:162-9.
6. Zangiabadi A, De Pasquale CG, Sajkov D. Pulmonary hyper- tension and right heart dysfunction in chronic lung disease.
Biomed Res Int 2014;2014:739674.
7. Launay D, Sobanski V, Hachulla E, Humbert M. Pulmonary hypertension in systemic sclerosis: different phenotypes.
Eur Respir Rev 2017;26:170056.
8. Launay D, Mouthon L, Hachulla E, Pagnoux C, de Groote P, Remy-Jardin M, et al. Prevalence and characteristics of mod- erate to severe pulmonary hypertension in systemic scle- rosis with and without interstitial lung disease. J Rheumatol 2007;34:1005-11.
9. Trad S, Amoura Z, Beigelman C, Haroche J, Costedoat N, Boutin le TH, et al. Pulmonary arterial hypertension is a ma- jor mortality factor in diffuse systemic sclerosis, in- dependent of interstitial lung disease. Arthritis Rheum 2006;54:184-91.
10. Ahmed S, Palevsky HI. Pulmonary arterial hypertension re- lated to connective tissue disease: a review. Rheum Dis Clin North Am 2014;40:103-24.
11. Galiè N, Manes A, Negro L, Palazzini M, Bacchi-Reggiani ML, Branzi A. A meta-analysis of randomized controlled tri- als in pulmonary arterial hypertension. Eur Heart J 2009;
30:394-403.
12. Barst RJ, McGoon M, Torbicki A, Sitbon O, Krowka MJ, Olschewski H, et al. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2004;43(12 Suppl S):40S-7S.
13. Er F, Ederer S, Nia AM, Caglayan E, Dahlem KM, Semmo N,
et al. Accuracy of Doppler-echocardiographic mean pulmo- nary artery pressure for diagnosis of pulmonary hypertension.
PLoS One 2010;5:e15670.
14. Gladue H, Altorok N, Townsend W, McLaughlin V, Khanna D. Screening and diagnostic modalities for connective tissue disease-associated pulmonary arterial hypertension: a sys- tematic review. Semin Arthritis Rheum 2014;43:536-41.
15. McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol 2009;53:1573-619.
16. Avouac J, Huscher D, Furst DE, Opitz CF, Distler O, Allanore Y; EPOSS group. Expert consensus for performing right heart catheterisation for suspected pulmonary arterial hypertension in systemic sclerosis: a Delphi consensus study with cluster analysis. Ann Rheum Dis 2014;73:191-7.
17. Khanna D, Tan M, Furst DE, Hill NS, McLaughlin VV, Silver RM, et al. Recognition of pulmonary hypertension in the rheumatology community: lessons from a Quality Enhance- ment Research Initiative. Clin Exp Rheumatol 2014;32(6 Suppl 86):S-21-7.
18. Jeon CH, Chai JY, Seo YI, Jun JB, Koh EM, Lee SK; pulmo- nary hypertension study group of Korean College of Rheumatology. Pulmonary hypertension associated with rheumatic diseases: baseline characteristics from the Korean registry. Int J Rheum Dis 2012;15:e80-9.
19. Kang KY, Jeon CH, Choi SJ, Yoon BY, Choi CB, Lee CH, et al. Survival and prognostic factors in patients with con- nective tissue disease-associated pulmonary hypertension diagnosed by echocardiography: results from a Korean na- tionwide registry. Int J Rheum Dis 2017;20:1227-36.
20. Gopal DM, Doldt B, Finch K, Simms RW, Farber HW, Gokce N. Relation of novel echocardiographic measures to in- vasive hemodynamic assessment in scleroderma-associated pulmonary arterial hypertension. Arthritis Care Res (Hoboken) 2014;66:1386-94.
21. Hachulla E, Clerson P, Airò P, Cuomo G, Allanore Y, Caramaschi P, et al. Value of systolic pulmonary arterial pressure as a prognostic factor of death in the systemic scle- rosis EUSTAR population. Rheumatology (Oxford) 2015;
54:1262-9.
22. van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum 2013;65:2737-47.
23. Petri M, Orbai AM, Alarcón GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum 2012;64:
2677-86.
24. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 Rheumatoid arthritis classi- fication criteria: an American College of Rheumatology/
European League Against Rheumatism collaborative initiative. Arthritis Rheum 2010;62:2569-81.
25. Fisher MR, Forfia PR, Chamera E, Housten-Harris T, Champion HC, Girgis RE, et al. Accuracy of Doppler echo- cardiography in the hemodynamic assessment of pulmo- nary hypertension. Am J Respir Crit Care Med 2009;179:
615-21.
26. Hsu VM, Chung L, Hummers LK, Wigley F, Simms R, Bolster M, et al. Development of pulmonary hypertension in a high-risk population with systemic sclerosis in the Pulmonary Hypertension Assessment and Recognition of Outcomes in Scleroderma (PHAROS) cohort study. Semin Arthritis Rheum 2014;44:55-62.
27. Frea S, Capriolo M, Marra WG, Cannillo M, Fusaro E, Libertucci D, et al. Echo Doppler predictors of pulmonary artery hypertension in patients with systemic sclerosis.
Echocardiography 2011;28:860-9.
28. Hübbe-Tena C, Gallegos-Nava S, Márquez-Velasco R, Castillo-Martínez D, Vargas-Barrón J, Sandoval J, et al.
Pulmonary hypertension in systemic lupus erythematosus:
echocardiography-based definitions predict 6-year survival.
Rheumatology (Oxford) 2014;53:1256-63.
29. Schwaiger JP, Khanna D, Gerry Coghlan J. Screening pa- tients with scleroderma for pulmonary arterial hyper- tension and implications for other at-risk populations. Eur Respir Rev 2013;22:515-25.
30. Prabu A, Gordon C. Pulmonary arterial hypertension in SLE: what do we know? Lupus 2013;22:1274-85.
31. Hao YJ, Jiang X, Zhou W, Wang Y, Gao L, Wang Y, et al.
Connective tissue disease-associated pulmonary arterial hy- pertension in Chinese patients. Eur Respir J 2014;44:
963-72.
32. Gonzalez-Juanatey C, Testa A, Garcia-Castelo A, Garcia- Porrua C, Llorca J, Ollier WE, et al. Echocardiographic and Doppler findings in long-term treated rheumatoid arthritis patients without clinically evident cardiovascular disease.
Semin Arthritis Rheum 2004;33:231-8.
33. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948-68.
34. Sun XG, Hansen JE, Oudiz RJ, Wasserman K. Pulmonary function in primary pulmonary hypertension. J Am Coll Cardiol 2003;41:1028-35.
35. Taichman DB, McGoon MD, Harhay MO, Archer-Chicko C, Sager JS, Murugappan M, et al. Wide variation in clinicians' assessment of New York Heart Association/World Health Organization functional class in patients with pulmonary arterial hypertension. Mayo Clin Proc 2009;84:586-92.
36. Benza RL, Miller DP, Gomberg-Maitland M, Frantz RP, Foreman AJ, Coffey CS, et al. Predicting survival in pulmo- nary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hyper- tension Disease Management (REVEAL). Circulation 2010;
122:164-72.
37. Barst RJ, Chung L, Zamanian RT, Turner M, McGoon MD.
Functional class improvement and 3-year survival outcomes in patients with pulmonary arterial hypertension in the REVEAL Registry. Chest 2013;144:160-8.
38. Felker GM, Allen LA, Pocock SJ, Shaw LK, McMurray JJ, Pfeffer MA, et al. Red cell distribution width as a novel prog- nostic marker in heart failure: data from the CHARM Program and the Duke Databank. J Am Coll Cardiol 2007;
50:40-7.
39. Hampole CV, Mehrotra AK, Thenappan T, Gomberg- Maitland M, Shah SJ. Usefulness of red cell distribution width as a prognostic marker in pulmonary hypertension.
Am J Cardiol 2009;104:868-72.
40. Lau GT, Tan HC, Kritharides L. Type of liver dysfunction in heart failure and its relation to the severity of tricuspid regurgitation. Am J Cardiol 2002;90:1405-9.