CASE REPORT
대장암으로 오인된 혈관주위상피모양세포종양 1예
조영환, 김경조, 예병덕, 변정식, 명승재, 양석균, 김진호
울산대학교 의과대학 서울아산병원 소화기내과학교실
A Case of a Perivascular Epithelioid Cell Tumor Mimicking Colon Cancer
Young Whan Cho, Kyung Jo Kim, Byong Duk Ye, Jeong Sik Byeon, Seung Jae Myung, Suk Kyun Yang and Jin Ho Kim Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Perivascular epithelioid cell tumor (PEComa) is extremely rare, which originated from mesenchymal cells in the intestine, and composed of histologically and immunohistochemically distinctive perivascular epithelioid cells. We report here on a case of PEComa in the sigmoid colon. A 62-year-old woman presented with hematochzia 10 days ago. Her abdominal computed tomography scan showed a 5 cm sized intraluminal fungating heterogeneously enhanced, high density mass, which infiltrated pericolic tissue surrounding the sigmoid colon. Colonoscopy showed a purple colored polypoid mass with lobulating contour in the sigmoid colon. She underwent laparoscopic anterior resection. On the histologic examination, the tumor consisted of polygonal epithelioid cells with sheet-like growth of nests, which looked like alveolar tissues in lung. The tumor cells were strongly positive stained with human melanoma black-45 (HMB-45). Pathologic examination was compatible with PEComa.
Sixteen months after surgery, she did well without tumor recurrence after surgery. We review the literatures concerning PEComa of the intestine focusing on endoscopic findings. (Korean J Gastroenterol 2012;60:377-381)
Key Words: Perivascular epithelioid cell tumor; Colonoscopy; Intestines
Received December 7, 2011. Revised January 16, 2012. Accepted January 30, 2012.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
교신저자: 김경조, 138-736, 서울시 송파구 올림픽로 43길 88, 울산대학교 의과대학 서울아산병원 소화기내과학교실
Correspondence to: Kyung Jo Kim, Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea. Tel: +82-2-3010-3196, Fax: +82-2-3010-8043, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
서 론
혈관주위상피모양세포종양(perivascular epithelioid cell tumor)은 중간엽에서 기원하지만 조직학적, 면역조직화학적 으로 위장관기질종양과 구분되는 혈관주위상피모양세포들로 이루어진 종양이다. 혈관주위상피모양세포종양은 혈관근지방 종, 림프관근종증, 폐의 clear cell “sugar” tumor 등을 포함 한다.1 혈관주위상피모양세포종양은 신장, 방광, 전립선, 자 궁, 난소, 폐, 췌장, 간 등에서의 발생은 다수 보고되고 있으 나,2 장관에서의 발생은 매우 드물어 국내에서는 비만곡부와 상행결장에서 발생한 2예만의 보고가 있다.3,4 그러나 현재까 지 대장내시경 소견에 초점을 맞춘 보고는 국내는 물론, 국외 에도 없는 실정이다. 이에 구불결장에서 발생한 혈관주위상피
모양세포종양 증례를 내시경 소견에 초점을 두고 기존의 보고 들과 함께 고찰하고자 한다.
증 례
62세 여자환자가 내원 3주 전부터 발생한 배변 시 복통과 내원 10일 전부터 발생한 혈변을 주소로 외부병원에서 대장 내시경검사를 시행하였고, 구불결장에 종괴가 발견되어 정밀 검사를 위해 본원으로 전원되었다. 혈변의 양상은 변을 볼 때 마다 소량씩 선홍색의 피가 변에 섞여 나오는 양상이었다. 과 거력에서 B형간염 보균자였으며 당뇨병, 고혈압 등은 없었고 약물의 복용력은 없었다. 가족력에서 특이사항은 없었고 음주 및 흡연력은 없었다. 내원 시 활력 증후는 혈압 117/78
Fig. 1. Abdominopelvic CT finding. An about 5 cm sized enhancing fungating mass (white arrow) was seen on the sigmoid colon.
Pericolic infiltration was also seen.
Fig. 2. Colonoscopic finding. A purple colored polypoid mass with lobulating contour was seen on the sigmoid colon.
mmHg, 체온 36.8oC, 맥박수 77회/분, 호흡수 20회/분으로 정상이었다. 의식은 명료하였고, 급성 병색을 보였다. 결막은 창백하였고, 공막에 황달은 없었다. 흉부청진에서 특이소견은 보이지 않았고, 심음은 정상이었다. 복부타진에서 압통과 반 발통은 없었으며 촉지되는 종괴도 없었다. 직장수지검사에서 괄약근의 긴장도는 정상이었으며 촉지되는 종괴는 없었다.
내원 시 말초혈액검사에서 백혈구 5,100/mm3, 혈색소 8.5 g/dL, 혈소판 189,000/mm3이었고, 생화학검사에서 혈액요소 질소 12 mg/dL, 크레아티닌 0.6 mg/dL였으며 AST/ALT 29/18 IU/L, 총빌리루빈은 0.4 mg/dL였다. 면역혈청검사에 서 B형간염 표면항원은 양성이었고 B형간염 표면항체는 음성 이었으며 C형간염 항체는 음성이었다. 혈청 내 종양표지자는 CEA 0.89 ng/mL, CA 19-9 8.8 U/mL였다.
흉부 X선검사에서 특이소견은 없었으며, 복부 전산화단층 촬영에서 구불결장에 내강을 채우는 약 5 cm 크기의 비균질 한 조영증강(Hounsfiled unit=120)을 보이는 종괴가 관찰되 었고 장벽 주위로 경미하게 침윤소견을 보였다. 그 외 간내 종괴는 없었으며 복강 내에 림프절 종대나 복수는 없었다
(Fig. 1).
입원 2일째 시행한 구불결장내시경검사에서 항문연에서 26 cm 근위부 구불경장에 관강을 거의 막고 있는 종괴가 관 찰되었다. 종괴의 표면 색조는 대장암의 육안 소견과 달리 짙 은 검붉은 색을 띠고 있었으며 선구 형태의 구분이 어려웠다.
또한 주변 점막과 경계가 명확히 구분되었고 분엽화되어 있었 으며 점막의 취약성 및 궤양이 관찰되었다(Fig. 2). 내시경 시 행 시 종괴의 점막 취약성으로 삼출출혈이 있는 상태였고 색 조 및 점막의 취약성을 고려할 때 혈관종을 배제할 수 없어 출혈의 위험성 때문에 조직생검을 시행하지 않았다. 외부병원 에서 시행했던 조직검사 결과에도 괴사된 조직만이 관찰되었 다. 이 환자에서 내시경초음파검사는 항문 출혈의 증상과 빈 혈이 있고 악성종양과의 감별이 어려워 대장 절제를 고려하였 기 때문에 치료계획에 영향을 주지 않을 것으로 생각되어 시 행하지 않았다.
입원 3일째 시행한 양전자단층촬영에서 구불결장의 종괴 에 해당하는 부위에 국소적으로 흡수증가(max SUV=3.5)를 보였다. 항문출혈의 증상이 있고 악성종양과의 감별이 힘들어 조직생검을 시행하지 않았으나 복강경을 이용한 전방절제술 을 시행하였다.
수술로 절제된 종괴는 장관 내로 돌출하며 성장하는 모습 을 보였고, 크기는 5.5×4.2×2.5 cm였으며, 표면에는 분엽상 을 보이며 종괴 내부의 미만성 출혈로 인해 검붉은 색을 띠고 있었다. 주변조직과 비교적 경계가 명확하였으나 국소적으로 대장주위 연부조직으로 침윤이 관찰되었다. 종괴의 절단면은 고형성이었으며 광범위한 종괴내 출혈이 관찰되었다(Fig. 3).
현미경 검사에서 종양은 주로 점막층과 점막하층에 위치해 있었으며 일부에서 장막과 대장주위 연부조직으로의 침윤이 관찰되었다. 종양을 구성하고 있는 세포들은 다각형 모양의 혈관주위상피모양세포들로 가는 섬유혈관성 중격에 의해 폐포 모양으로 배열되어 있었다. 절제된 조직에 대해 면역조직화학 염색을 시행한 결과, human melanoma black-45 (HMB-45)
Fig. 3. Gross finding. (A) A 5.5 cm sized polypoid mass with lobulating contour was noted. (B) The cut surface showed diffuse hemorrhage.
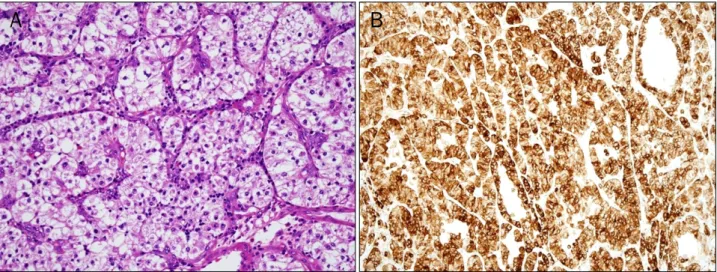
Fig. 4. Microscopic finding. (A) H&E stain (×400) showed the sheet-like growth of nests of epithelioid cells with an alveolar appearance. (B) The tumor cells were positive for human melanoma black-45 (×200).
에 강한 양성을 보였으며, vimentin에는 약양성을 보였고, cytokeratin, S-100 단백, smooth muscle actin, CD117, synaptophysin, chromogranin, cytokeratin 7, cytokeratin 20, CDX2, CD10, desmin, hepatocyte antigen에는 음성을 보여 혈관주위상피모양세포종양에 합당하였다(Fig. 4).
환자는 수술 후 7일째 합병증 없이 퇴원하여 외래 추적관 찰 중으로 수술 후 1년 4개월이 지난 현재까지 재발 없이 경 과 관찰 중이다.
고 찰
혈관주위상피모양세포종양은 1992년 처음 기술되었으며 평활근 및 멜라닌세포의 분화를 동시에 보이는 종양을 총칭하 는 용어이다.3 이 종양은 조직학적으로 혈관주위상피모양세포 가 공통적으로 존재하고 면역조직화학염색 시 HMB-45에 양 성 염색을 보이는 것이 특징이다.3 그러나 장관에서 발생한 혈관주위상피모양세포종양은 극히 드물어서 대장내시경 소견 에 대해서는 알려져 있는 바가 없다.
현재까지 국내 혹은 국외에서 보고된 장관에 발생한 혈관 주위상피모양세포종양은 총 20예이다.2-19 기존에 보고된 환 자들의 나이의 중앙값은 32세(6-63세)였고, 남성과 여성의 비 는 1:3으로 여성에 많았다. 이번 증례의 환자도 62세 여성으 로 기존의 보고들에 부합하였다.
이번 증례를 포함한 기존의 장관에서 발생했던 21예의 발 생부위는 직장이 5예로 가장 많았고, 다음으로는 맹장 4예, 구불결장 4예, 말단회장 2예 순이었으며 상행결장, 하행결장, 공장, 횡행결장이 각각 1예씩이었다. 이번 증례의 환자는 구 불결장에서 종양이 발생하였다. 종양의 크기의 중앙값은 3.7 cm (범위 1.2-13 cm)였으며 종양의 크기가 4 cm보다 작은 종양들은 점막층과 점막하층에 위치하였고 4 cm보다 큰 종양 들은 주로 장막층 근처에서 발생하여 장관 밖으로 자라는 경 우가 많았다(Table 1).
이번 증례를 포함한 혈관주위상피모양세포종양 21예 중 대 장내시경은 13예에서만 시행되었는데 이를 분석하면 내강 내 로 돌출하는 폴립모양종괴로 관찰되는 경우가 12예, 외부압 박으로 관찰되는 경우가 1예였다.2-5,8,9,11,13-15,17,18 크기가 1.5
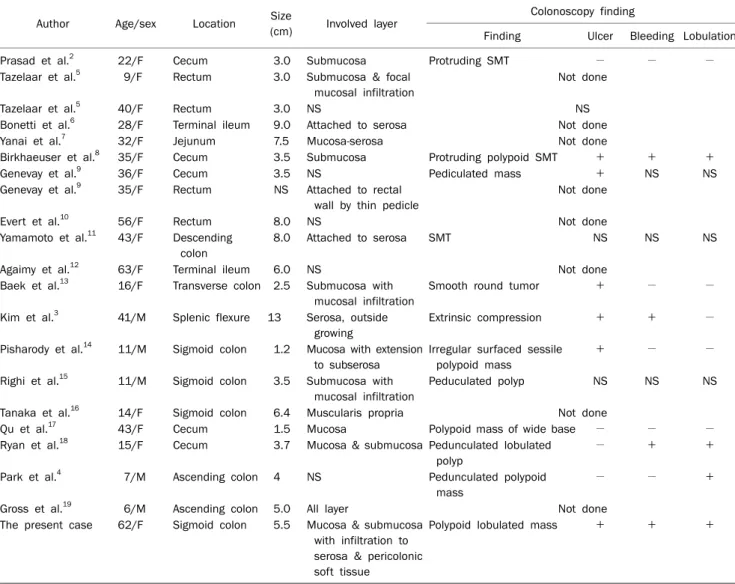
Table 1. Published Perivascular Epithelioid Cell Tumor Cases in Intestine
Author Age/sex Location Size
(cm) Involved layer Colonoscopy finding
Finding Ulcer Bleeding Lobulation
Prasad et al.2 22/F Cecum 3.0 Submucosa Protruding SMT − − −
Tazelaar et al.5 9/F Rectum 3.0 Submucosa & focal mucosal infiltration
Not done
Tazelaar et al.5 40/F Rectum 3.0 NS NS
Bonetti et al.6 28/F Terminal ileum 9.0 Attached to serosa Not done
Yanai et al.7 32/F Jejunum 7.5 Mucosa-serosa Not done
Birkhaeuser et al.8 35/F Cecum 3.5 Submucosa Protruding polypoid SMT + + +
Genevay et al.9 36/F Cecum 3.5 NS Pediculated mass + NS NS
Genevay et al.9 35/F Rectum NS Attached to rectal wall by thin pedicle
Not done
Evert et al.10 56/F Rectum 8.0 NS Not done
Yamamoto et al.11 43/F Descending colon
8.0 Attached to serosa SMT NS NS NS
Agaimy et al.12 63/F Terminal ileum 6.0 NS Not done
Baek et al.13 16/F Transverse colon 2.5 Submucosa with mucosal infiltration
Smooth round tumor + − −
Kim et al.3 41/M Splenic flexure 13 Serosa, outside growing
Extrinsic compression + + −
Pisharody et al.14 11/M Sigmoid colon 1.2 Mucosa with extension to subserosa
Irregular surfaced sessile polypoid mass
+ − −
Righi et al.15 11/M Sigmoid colon 3.5 Submucosa with mucosal infiltration
Peduculated polyp NS NS NS
Tanaka et al.16 14/F Sigmoid colon 6.4 Muscularis propria Not done
Qu et al.17 43/F Cecum 1.5 Mucosa Polypoid mass of wide base − − −
Ryan et al.18 15/F Cecum 3.7 Mucosa & submucosa Pedunculated lobulated polyp
− + +
Park et al.4 7/M Ascending colon 4 NS Pedunculated polypoid
mass
− − +
Gross et al.19 6/M Ascending colon 5.0 All layer Not done
The present case 62/F Sigmoid colon 5.5 Mucosa & submucosa with infiltration to serosa & pericolonic soft tissue
Polypoid lobulated mass + + +
M, male; F, female; NS, not specified; SMT, submucosal tumor.
cm보다 작았던 2예에서는 무경성 폴립으로 관찰되었고,14,19 2.5-5.5 cm 크기에서는 유경성 폴립으로 관찰되었다. 장막층 에서 기원한 13 cm 크기의 증례에서는 외부압박소견으로 관 찰되었다.3 그 외 소견으로 점막표면의 궤양이 관찰된 증례가 6예, 출혈이 관찰된 증례가 4예, 분엽상 모양이 관찰된 증례가 4예 있었다.
또, 대장내시경을 시행했던 13예 중 진단을 위한 조직생검 은 4예에서만 시행되었는데 그 중 1예(20%)에서 조직학적으 로 확진이 되었고,17 2예에서는 종양세포가 발견되었으나 확 진은 하지 못했으며,8,18 남은 1예에서는 비정형세포만 관찰되 어3 조직생검으로 확진되는 경우가 낮았다. 확진이 된 증례는 점막층에서 발생한 증례였고,17 종양세포가 발견은 되었으나 확진이 되지 못한 증례 중 하나는 점막하층에서 발생한 종양 이었는데 면역조직화학염색까지 시행하였으나 중간엽에서 발
생한 종양이라는 것만 확인되었고 확진이 되지 않아 수술로 종양 제거 후 확진되었다.8 다른 하나의 증례는 점막층과 점막 하층에서 발생한 종양이었는데 그 논문에 조직검사의 결과가 정확히 기술되어 있지 않고 악성종양을 시사한다고만 기록되 어 있어 왜 확진이 되지 않았는지는 판단하기 힘들었다.18 비 정형세포만 관찰되었던 증례는 종양이 장막층에서 발생하여 장벽 외측으로 자라는 종양으로 내시경으로는 외부압박으로 관찰되었기 때문에 확진이 되지 않았을 것으로 생각된다.3
이번 증례에서 구불결장내시경검사 시행 시 조직생검을 시 행하지 않았는데 이는 내시경 관찰 시 종괴의 점막 취약성으 로 삼출출혈이 있는 상태였고, 색조를 고려할 때 혈관종을 배 제할 수 없고, 생검 후 출혈의 위험성 때문에 조직생검을 시행 하지 않았다.
혈관주위상피모양세포종양은 드물게 발생하므로 표준치료
는 정립되어 있지 않으나 수술적 절제가 추천되고 있다.19 그 러나 Baek 등13은 점막층과 점막하층에 국한되어 있고 복부 전산화단층촬영에서 림프절 종대가 없는 2.5 cm 크기의 종양 을 내시경적 절제로 제거했다고 보고하였다. 이를 볼 때 종양 크기가 작고 점막하층 이내에 국한되어 있으며 주변으로의 침 윤이나 전이가 없다면 내시경적 절제를 시도해 볼 수도 있을 것으로 생각된다.
혈관주위상피모양세포종양은 드문 종양이므로 자연사나 예후에 대해서 알려져 있는 바가 거의 없으나 대부분 양성의 경과를 취한다고 알려져 있다.19 그러나 Folpe 등20은 악성경 과와 연관된 인자들로 5 cm 이상의 종양크기, 침윤성 성장, 핵 다형성 정도, 괴사, 높은 유사분열정도(고배율상 1/50 이 상) 등을 제안하였다.
결론으로, 장관에서 발생하는 혈관주위상피모양세포종양 은 매우 드물고, 내시경에서 종양이 존재하는 장벽내 위치와 크기에 따라 다양한 모습으로 나타날 수 있으며, 점막층을 침 범하지 않는 한 조직생검을 하더라도 확진되는 비율이 낮았 다. 그러나 관강 내 고형의 짙은 붉은 색 종양이 있을 때는 감별진단에 고려해야 하겠다.
REFERENCES
1. Folpe AL, Kwiatkowski DJ. Perivascular epithelioid cell neo- plasms: pathology and pathogenesis. Hum Pathol 2010;41:1- 15.
2. Prasad ML, Keating JP, Teoh HH, et al. Pleomorphic angiomyoli- poma of digestive tract: a heretofore unrecognized entity. Int J Surg Pathol 2000;8:67-72.
3. Kim KH, Jang BI, Kim TN, et al. A case of perivascular epithelioid cell tumor (PEComa) arising in the colon. Korean J Intern Med 2007;72:540-545.
4. Park SJ, Han DK, Baek HJ, et al. Perivascular epithelioid cell tu- mor (PEComa) of the ascending colon: the implication of IFN-α 2b treatment. Korean J Pediatr 2010;53:975-978.
5. Tazelaar HD, Batts KP, Srigley JR. Primary extrapulmonary sugar tumor (PEST): a report of four cases. Mod Pathol 2001;14:
615-622.
6. Bonetti F, Martignoni G, Colato C, et al. Abdominopelvic sarcoma of perivascular epithelioid cells. Report of four cases in young women, one with tuberous sclerosis. Mod Pathol 2001;14:563- 568.
7. Yanai H, Matsuura H, Sonobe H, Shiozaki S, Kawabata K.
Perivascular epithelioid cell tumor of the jejunum. Pathol Res Pract 2003;199:47-50.
8. Birkhaeuser F, Ackermann C, Flueckiger T, et al. First description of a PEComa (perivascular epithelioid cell tumor) of the colon:
report of a case and review of the literature. Dis Colon Rectum 2004;47:1734-1737.
9. Genevay M, Mc Kee T, Zimmer G, Cathomas G, Guillou L.
Digestive PEComas: a solution when the diagnosis fails to "fit".
Ann Diagn Pathol 2004;8:367-372.
10. Evert M, Wardelmann E, Nestler G, Schulz HU, Roessner A, Röcken C. Abdominopelvic perivascular epithelioid cell sarcoma (malignant PEComa) mimicking gastrointestinal stromal tumour of the rectum. Histopathology 2005;46:115-117.
11. Yamamoto H, Oda Y, Yao T, et al. Malignant perivascular epithe- lioid cell tumor of the colon: report of a case with molecular analysis. Pathol Int 2006;56:46-50.
12. Agaimy A, Wünsch PH. Perivascular epithelioid cell sarcoma (malignant PEComa) of the ileum. Pathol Res Pract 2006;202:
37-41.
13. Baek JH, Chung MG, Jung DH, Oh JH. Perivascular epithelioid cell tumor (PEComa) in the transverse colon of an adolescent: a case report. Tumori 2007;93:106-108.
14. Pisharody U, Craver RD, Brown RF, Gardner R, Schmidt-Sommer- feld E. Metastatic perivascular epithelioid cell tumor of the colon in a child. J Pediatr Gastroenterol Nutr 2008;46:598-601.
15. Righi A, Dimosthenous K, Rosai J. PEComa: another member of the MiT tumor family? Int J Surg Pathol 2008;16:16-20.
16. Tanaka M, Kato K, Gomi K, et al. Perivascular epithelioid cell tumor with SFPQ/PSF-TFE3 gene fusion in a patient with advanced neuroblastoma. Am J Surg Pathol 2009;33:1416- 1420.
17. Qu GM, Hu JC, Cai L, Lang ZQ. Perivascular epithelioid cell tumor of the cecum: a case report and review of literatures. Chin Med J (Engl) 2009;122:1713-1715.
18. Ryan P, Nguyen VH, Gholoum S, et al. Polypoid PEComa in the rectum of a 15-year-old girl: case report and review of PEComa in the gastrointestinal tract. Am J Surg Pathol 2009;33:475- 482.
19. Gross E, Vernea F, Weintraub M, Koplewitz BZ. Perivascular epithelioid cell tumor of the ascending colon mesentery in a child: case report and review of the literature. J Pediatr Surg 2010;45:830-833.
20. Folpe AL, Mentzel T, Lehr HA, Fisher C, Balzer BL, Weiss SW.
Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol 2005;29:1558-1575.