■
Yong-Woo Lee, PT, MS; Se-Jong Choi, PT, MS; Chang-Ho Song, PT, PhD
■
전체 글
■
■
수치

관련 문서
The purpose of this study is to come up with a method to evaluate Virtual Reality Art. To suggest the method, Noël Carroll's category-relative evaluation
Based on the above results, the 12-week complex type correction program had a positive effect on the shoulder angle, trunk rotation angle, and body shape
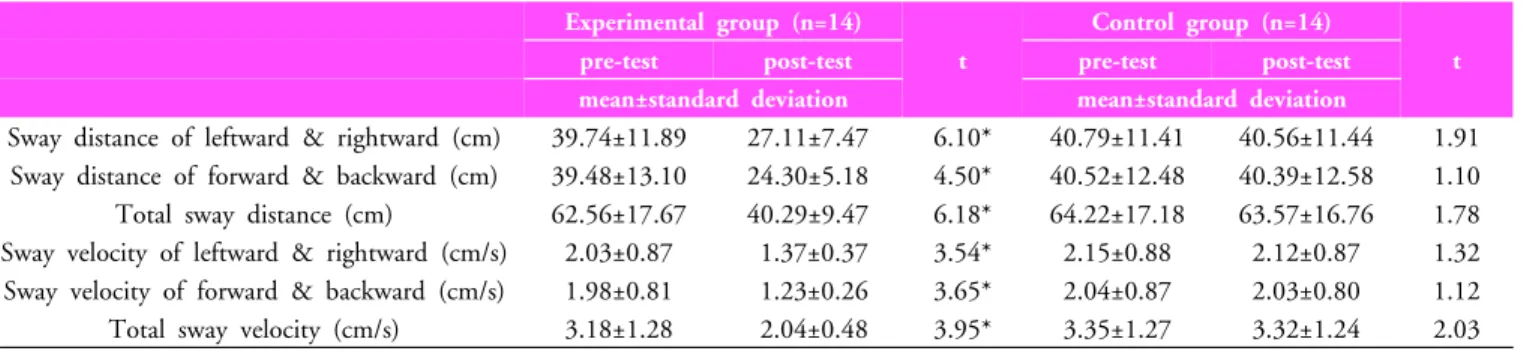
The purpose of this study was to investigate how the Da Vinci body board exercise program affects the body balance and physical stress of women with body imbalance.. For
The purpose and necessity of this study was to investigate the effect of the 8-week GX complex exercise program on the stress index, blood lipid and APG
Third, for the change in balance ability according to core training and plyometric training, the core group showed a significant difference in travel area
The purpose of this study was to investigate the change of body composition and physical fitness after 12 weeks of practice with middle-aged women centered
Second, with regards to the human resource development measures to improve the qu ality of life of the lower-income classes, general agreement was reached on the need
The effect of the stress management program on the stress coping and perceived stress of the patients with finger replantation. Unpublished master's
