Introduction
Anterior interosseous nerve (AIN) syndrome is cha
racterized by palsy of the flexor pollcis longus, the flexor digitorum profundus of the index and middle fingers, and the pronator quadratus muscle, and is also
referred to as KilohNevin syndrome.
1,2The incidence of AIN syndrome is low and accounts for less than 1% of all compression syndromes in the upper limb.
3The exact cause and pathophysiology remain unclear, but the suspected cause of spontaneous AIN palsy has been reported as neuralgic amyotrophy (NA), isolated neuritis, and entrapment neuropathy.
2,4,5Although a few cases of NA presenting as AIN palsy have been reported, predominant AIN paresis was very rare (9/246 cases, 3.6%).
6Recently, we encountered a patient diagnosed with isolated AIN palsy after videoassisted thoracoscopic surgery (VATS). Here we report a case and review the
비디오흉강경수술 후 전방골간신경증후군 형태로 나타난 신경통성근위축 - 증례 보고 -
김철기
1
, 구정회2
, 송선홍2
1대구 명성요양병원, 2울산대학교 의과대학 강릉아산병원 재활의학교실
Neuralgic Amyotrophy Presenting as Anterior Interosseous Nerve Syndrome After Video-Assisted Thoracoscopic Surgery - Case Report -
Cheol Ki Kim
1, Jung Hoi Koo
2, Sun Hong Song
21
Daegu Myungsung Medical Center, Daegu,
2Department of Rehabilitation Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea
Received February 7, 2017
Revised (1st) April 11, 2017, (2nd) May 11, 2017 Accepted May 12, 2017
Corresponding Author: Jung Hoi Koo
Department of Rehabilitation Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, 38 Bangdong-gil, Sacheon- myeon, Gangneung 25440, Korea
Tel: 82-33-610-4951, Fax: 82-33-610-4960, E-mail: [email protected]
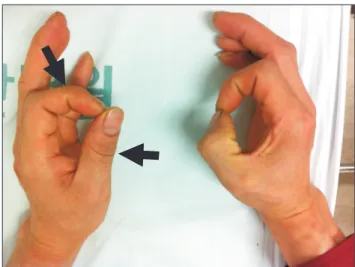
Anterior interosseous nerve (AIN) syndrome is a pure motor syndrome resulting in characteristic weakness of pinch between the thumb and index finger. Different etiologies such as spontaneous, traumatic, compression are suggested, but remain controversial. To our knowledge, a case of neuralgic amyotrophy (NA) presenting as predominant AIN palsy after video-assisted thoracoscopic surgery have not been reported yet. Hence, we report the case of a 34-year-old man who presented with thumb weakness and was diagnosed with AIN palsy due to NA.
Key Words: syndrome, neuralgic amyotrophy, palsy
Copyright © by Korean Association of EMG Electrodiagnostic Medicine
This is an Open Ac cess article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.