Annals of Surgical Treatment and Research 47
pISSN 2288-6575 • eISSN 2288-6796 http://dx.doi.org/10.4174/astr.2014.87.1.47 Annals of Surgical Treatment and Research
TECHNICAL ADVANCE
The paracholedochal vein: a feasible option as portal inflow in living donor liver transplantation
Joo Dong Kim, Dong Lak Choi, Young Seok Han
Division of Hepatobiliary Pancreas Surgery and Abdominal Organ Transplantation, Department of Surgery, Daegu Catholic University School of Medicine, Daegu, Korea
INTRODUCTION
Portal vein thrombosis (PVT) with cavernous transformation of the portal vein (CTPV) represents a surgically demanding challenge in living donor liver transplantation (LDLT) [1].
Although various surgical techniques and approaches to PVT has been introduced to overcome PVT, the absence of portal flow remains a surgically demanding challenge in the setting of LDLT because it has an obvious influence on surgical complexity, morbidity and mortality rates [1-3]. Furthermore, portal vein (PV) reconstruction is a very difficult procedure in LDLT with extensive PVT with CTPV in the setting of decreasing portal hypertension and providing adequate portal inflow [3,4]. Therefore, most transplant surgeons have hesitated to perform LDLT in cases with diffuse PVT and CTPV [4,5]. Herein, we present two successful adult LDLT using paracholedochal veins as portal inflow in cases with diffuse
PVT and CTPV.
SURGICAL TECHNIQUES
Case 1
A 63-year-old female patient with hepatitis B-related liver cirrhosis was transferred to Daegu Catholic University Medical Center because of refractory ascites and hepatic encephalopathy.
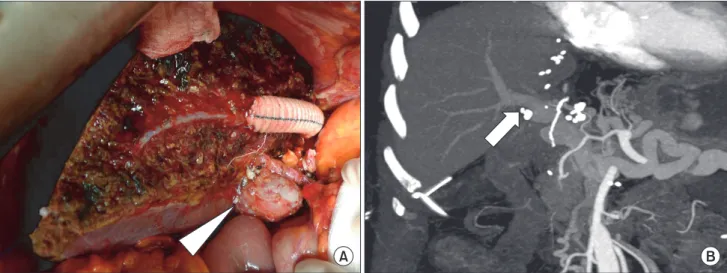
Preoperative Doppler ultrasonography and multidimensional computed tomography (MDCT) revealed the diffuse PVT that extended to the superior mesenteric vein (SMV) and splenic vein. In addition, marked dilated paracholedochal veins around the PV were being fed from the gastroepiploic veins and pan- crea ticoduodenal veins (Fig. 1A). Mesenteric venography demon- strated several findings, including complete invisibility of the main PV and SMV and large tortuous paracholedochal veins that extended to the proximal SMV (Fig. 1B). The donor was her
Received October 29, 2013, Revised December 26, 2013, Accepted January 14, 2014
Corresponding Author: Dong Lak Choi
Division of Hepatobiliary Pancreas Surgery and Abdominal Organ Transplantation, Department of Surgery, Daegu Catholic University Medical Center, Daegu Catholic University School of Medicine, 33 Duryugongwon-ro 17-gil, Nam-gu, Daegu 705-718, Korea Tel: +82-53-650-4063, Fax: +82-53-650-4950
E-mail: [email protected]
Copyright ⓒ 2014, the Korean Surgical Society
cc Annals of Surgical Treatment and Research is an Open Access Journal. All articles are distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Extensive thrombosis of the portal and splenomesenteric veins combined with cavernous transformation of the portal vein (CTPV) has been considered to be a contraindication for living donor liver transplantation (LDLT) due to technical difficulties and perioperative risks. In recent years, several surgical innovations including cavoportal hemitransposition, renoportal anastomosis, and portal arterialization have been introduced to overcome diffuse portal vein thrombosis (PVT) and CTPV, but their outcomes were unsatisfactory with significant morbidity and mortality. Herein, we report two successful cases of adult LDLT in diffuse PVT with CTPV managed using the paracholedochal vein as portal inflow to the graft.
[Ann Surg Treat Res 2014;87(1):47-50]
Key Words: Cavernous transformation of portal vein, Liver transplantation, Living donors
48
Annals of Surgical Treatment and Research 2014;87(1):47-50
59-year-old brother. The estimated graft volume of the donor’s right lobe as calculated by CT volumetry was 798 mL, 63.7%
of the whole liver and the estimated graft-to-recipient weight ratio (GRWR) was 1.42%. Therefore, LDLT using a modified right lobe graft from her younger brother was performed. After complete mobilization of the recipient’s liver, hepatic hilar dissection was attempted. However, dissection of the vascular pedicle at the hilum was too difficult due to severe fibrosis and a complex network of tortuous paracholedochal varices.
Thus, after dissection and ligation of the hepatic arteries were performed, the PV and bile duct were clamped and transected en masse. Dissection of the native PV revealed that it had no obvious lumen and was replaced by a fibrotic, thrombosed cord. We identified two collateral veins with large orifices around the bile duct and transformed these large dilated
collaterals into a common orifice with a venoplasty at their confluence. Several small collaterals which were not suitable for portal inflow were ligated. After declamping of the hilum, we ensured that the blood flow was adequate for portal inflow by spurting through the common orifice. We carried out usual end-to-end anastomosis of the donor PV to the large common orifice formed by the confluence of the markedly dilated paracholedochal veins using a running suture of 6-0 prolene (Fig. 2A). The graft was reperfused after completion of the PV anastomosis followed by hepatic artery reconstruction using a microsurgical technique. Roux-en-Y hepaticojejunostomy was performed because of severe periductal fibrosis and a narrowed caliber that could not maintain bile flow for duct-to- duct anastomosis. Intraoperative Doppler assessment showed adequate portal blood flow to the graft, and the PV patency was
Fig. 1. (A) Preoperative CT showed diffuse portal vein thrombosis (arrow) extended to superior mesenteric vein (SMV) and marked dilated paracholedochal veins (arrowhead). (B) Schematic illustration of cavernous transformation of the portal vein found at CT and mesenteric venography showed large tortuous paracholedochal collaterals (arrows) and complete invisibility of main portal vein and proximal SMV due to thrombosis. PV, portal vein; SV, splenic vein; GEV, gastroepiploic vein.
Fig. 2. (A) End-to-end portal anastomosis was constructed between the graft and common cloaca formed by the confluence of paracholedochal veins (arrowhead). (B) Good portal vein patency to the graft (arrow) was demonstrated by dynamic computed tomography on the 14th postoperative day.
Annals of Surgical Treatment and Research 49 demonstrated by regular Doppler monitoring and MDCT (Fig.
2B).
The patient was discharged 3 weeks postoperatively without any complications and has been doing well for 22 months with normal graft function.
Case 2
A 51-year-old man was admitted with massive ascites and general weakness due to alcoholic liver cirrhosis. Preoperative Doppler ultrasonography and MDCT demonstrated several dilated paracholedochal veins along hilum and diffuse PVT extended to SMV like the first case. The donor was his 30-year- old son. The preoperative CT volumetry demonstrated the estimated right to left lobe volumes to be 966 mL and 500 mL (65.9% and 34.1% in volume ratio) and the estimated GRWR was 1.19%. Thus, we planned to perform LDLT using a modified right lobe graft from his son. During the operation, we found chronic organized PVT with dilated paracholedochal collaterals along porta hepatis. The transected PV showed no venous flow;
it contained chronic totally organized thrombi with fibrosis.
Even though we tried to eversion thrombectomy, it was failed to obtain sufficient portal inflow to the graft. Unfortunately, the caliber of these collaterals was smaller than that of case 1 and venous flow through common orifice with venoplasty from their confluence was not sufficient for portal inflow.
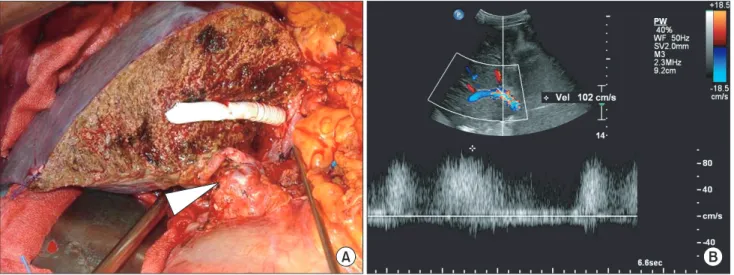
Because another approach to gain splanchnic inflow could not be available, we performed unification venoplasty with common colaca from paracholedochal veins and partially recanalized naitive PV to supplement unsatisfactory inflow through paracholedochal collaterals. This complex common orifice was anastomosed to the donor PV in end-to-end fashion as a single anastomosis (Fig. 3A). Hepatic artery and bile duct
reconstruction was performed by the same method as case 1.
Intraoperative Doppler ultrasonography showed satisfactory portal blood flow in the liver graft and the good PV patency was demonstrated by serial postoperative Doppler studies(Fig.
3B) and MDCT. He was discharged without any serious com- plication and has remained stable without ascites, variceal bleeding for 21 months after transplantation.
DISCUSSION
In the early period of liver transplantation, PVT was consi- dered to be a contraindication for the procedure because of the technical difficulties it entailed, especially the inability to gain an adequate portal supply [6]. However, several surgical techniques have been developed for deceased donor liver transplantation (DDLT), such as thrombectomy, interposition or a jump graft between the donor and recipient PV, cavoportal hemitransposition (CPHT), renoportal anastomosis (RPA), and PV arterializations [1,2]. With these surgical innovations, the results of DDLT for patients with PVT have been comparable to those of patients without PVT [1,6]. In spite of recent reports that described excellent outcomes in LDLT, several difficulties are associated with performance of these surgical innovations for pre-existing PVT in the setting of LDLT, such as the necessity of distal dissection of the vascular pedicle of the hilum, restricted availability of deceased donor vein grafts, and ethical concerns of the living donor [7]. Moreover, LDLT is still considered a surgically demanding challenge in the case of an extended PVT including the SMV with CTPV because this procedure is associated with perioperative morbidity and mortality as a result of rethrombosis and increased blood loss [8].
In 1986, Hiatt et al. [9] reported the first successful DDLT
Fig. 3. (A) The complex common orifice formed by venoplasty from paracholedochal collaterals and native portal vein was anastomosed to the donor portal vein (arrowhead). (B) Serial postoperative Doppler studies demonstrated satisfactory portal vein flow to the graft.
Joo Dong Kim, et al: Portal revascularization using paracholedochal vein in living donor liver transplantation
50
Annals of Surgical Treatment and Research 2014;87(1):47-50
using a thin-walled bile duct varix as the inflow to the donor PV, and various alternatives were subsequently reported to overcome PVT with CTPV, such as CPHT, RPA, and portal arterializations [2,3]. In the present case, we planned to per- form PV reconstruction using large dilated paracholedochal veins because it was demonstrated that these collaterals could provide the adequate portal inflow to the graft in preoperative MDCT and mesenteric venography. This technique offers some advantages over other surgical options using systemic blood flow as portal inflow. The advantages include the followings:
(1) In PV reconstruction such as RPA, CPHT causes loss of hepatotrophic factors provided by PV inflow, which is believed to be essential for hepatic regeneration [2]. (2) In patients undergoing RPA and CPHT, persistent portal hypertension has been described with ascites, renal dysfunction, variceal bleeding, and hepatic encephalopathy [2,3]. (3) The long- term effects of PV inflow with systemic venous flow remain
unknown [2]. Finally, (4) less vascular dissection is required and the operating time is decreased to a jump graft from the SMV to PV of the graft [10]. However, this technique, as mentioned above, also has disadvantages; e.g., using collateral veins to reconstruct the portal flow may increase the incidence of vascular complications such as thrombosis [1,10].
CONCLUSION
The use of a recipient’s enlarged paracholedochal veins as a splanchnic venous supply into the graft can be a feasible option in cases with diffuse PVT and CTPV during LDLT.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Maluf D, Shim I, Posner M, Cotterell AH, Fisher RA. Salvage procedure for unex- pected portal vein thrombosis in living donor liver transplantation. Transplant Proc 2006;38:1422-4.
2. Rotellar F, Cienfuegos JA, Bueno A, Marti P, Valenti V, Zozaya G, et al. Por tal revascularization in the setting of caver- nous transformation through a para- choledocal vein: a case report. Trans plant Proc 2010;42:3079-80.
3. Paskonis M, Jurgaitis J, Mehrabi A, Kashfi A, Fonouni H, Strupas K, et al. Surgical strategies for liver transplantation in the case of portal vein thrombosis: current role of cavoportal hemitransposition and renoportal anastomosis. Clin Transplant 2006;20:551-62.
4. Zhang MM, Jin XQ, Yan LN, Kang Q, Guo
CB. Living-related liver transplantation for cavernous transformation of portal vein:
a clinical study of 3 cases. Zhonghua Gan Zang Bing Za Zhi 2008;16:270-3.
5. Zhang M, Guo C, Pu C, Ren Z, Li Y, Kang Q, et al. Adult to pediatric living donor liver trans plantation for portal cavernoma.
Hepa tol Res 2009;39:888-97.
6. Tao YF, Teng F, Wang ZX, Guo WY, Shi XM, Wang GH, et al. Liver transplant reci pients with portal vein thrombosis: a single center retrospective study. Hepato- biliary Pancreat Dis Int 2009;8:34-9.
7. Cho JY, Suh KS, Shin WY, Lee HW, Yi NJ, Lee KU. Thrombosis confined to the portal vein is not a contraindication for living donor liver transplantation. World J Surg 2008;32:1731-7.
8. Zhang LJ, Yang GF, Jiang B, Wen LQ, Shen W, Qi J. Cavernous transformation of portal vein: 16-slice CT portography and correlation with surgical procedure of orthotopic liver transplantation. Abdom Imaging 2008;33:529-35.
9. Hiatt JR, Quinones-Baldrich WJ, Ramming KP, Lois JF, Busuttil RW. Bile duct varices.
An alternative to portoportal anastomosis in liver transplantation. Transplantation 1986;42:85.
10. Wu TH, Chou HS, Pan KT, Lee CS, Wu TJ, Chu SY, et al. Application of cryo- preserved vein grafts as a conduit bet- ween the coronary vein and liver graft to reconstruct portal flow in adult living liver transplantation. Clin Transplant 2009;23:751-5.