Hilar Branching Anatomy of Living Adult Liver Donors:
Comparison of T2-MR Cholangiography and Contrast Enhanced T1-MR Cholangiography in Terms of Diagnostic Utility
1Joon Seok Lim, M.D.1, Myeong-Jin Kim, M.D.1,3, Kyung Sik Kim, M.D.2, Joo Hee Kim, M.D.1, Young Taik Oh, M.D.1, Jin Yong Kim, M.D.1, Hyung Sik Yoo, M.D.1,
Jong Tae Lee, M.D.1, Ki Whang Kim, M.D.1
1Department of Diagnostic Radiology, Yonsei University College of Medicine
2Department of Surgery, Yonsei University College of Medicine
3BK21 Project of Medical Science Yonsei University College of Medicine Received June 24, 2003 ; Accepted November 17, 2003
Address reprint requests to : Myeong-Jin Kim, M.D., Department of Diagnostic Radiology, Yonsei University Medical College, 134 Shinchon-dong, Seodaemoon-gu, Seoul 120-752, Republic of Korea.
Tel. 82-2-361-5843 Fax. 82-2-393-3035 E-mail: [email protected]
Purpose: To compare T2-weighted MR cholangiography (T2-MRC) and contrast-en- hanced T1-weighted MRC (enhanced T1-MRC) in the assessment of biliary anatomy in donor candidates for living related liver transplantation (LRLT).
Materials and Methods: Thirty-three potential donors underwent MR examination for preoperative evaluation. Using the single-shot half-Fourier RARE sequence, T2-weighted single-section and coronal images were obtained, and enhanced T1-MRC was performed, using 3D GRE sequences after the administration of mangafodifir trisodium. To assess the hilar ductal branching pattern and determine diagnostic confidence, two reviewers first evaluated the unpaired T2-MRC and enhanced T1-MRC images, and then paired T2-MRC and enhanced T1-MRC images together. In particular, in 12 cases in which direct cholan- giographys were performed, the feasibility of single duct-to-duct anastomosis was assessed using the unpaired and the paired sets sequentially.
Results: The reviewers’confidence tended to be higher for enhanced T1-MRC than T2- MRC, but the difference was not statistically significant. For both reviewers, confidence was significantly higher for the paired set than for T2- or enhanced T1-MRC alone (p <
.001). The types of biliary anatomy determined in the paired set matched the consensus reading in 33 (100%) and 30 cases(91%) assessed by reviewer 1 and 2, respectively. The separate interpretation of T2- and enhanced T1-MRC findings matched the consensus in- terpretation in 30 (91%) and 28 cases (85%), respectively, assessed by reviewer 1, and 26 (79%) and 28 cases (85%), respectively, assessed by reviewer 2. The possibility of single anastomosis was accurately predicted in 91.6% of cases in T2-MRC, and 100% at en- hanced T1-MRC and the combined set.
Conclusion: In the evaluation of the biliary anatomy of potential donors for LRLT, the combined use of T2-MRC and enhanced T1-MRC may improve diagnostic confidence and decrease the occurrence of a non diagnostic or equivocal interpretation at T2-MRC alone.
Index words :Bile duct radiography, technology Bile ducts MR
Bile ducts surgery Liver, transplantation
The evaluation of the biliary anatomy of donor candi- dates for adult-to-adult right lobe transplantation is es- sential. A candidate with biliary variants such as anom- alous drainage of the right posterior segmental duct (draining segments Ⅵ and Ⅶ) or trifurcation can pre- clude single duct-to-duct biliary anastomosis in the transplant recipient (1).
T2 weighted MR cholangiography (T2-MRC) is be- coming the modality of choice for the noninvasive eval- uation of biliary tract abnormalities, but its diagnostic limitations include poor visualization of the intrahepatic biliary tree compared with the extrahepatic (2), particu- larly in non-dilated systems such as that seen in healthy donor candidates. The recent development of liver-spe- cific contrast agents which excrete into the biliary tree, such as mangafodipir trisodium, has renewed interest in contrast-enhanced MR imaging of the biliary tree, a pro- cedure that may counter the limitations of heavily T2- weighted MR cholangiography. Lee et al. suggested that T1-weighted MR imaging, particularly when it involves high-resolution volumetric T1-weighted imaging of the liver, may facilitate the definition of intrahepatic bile duct anatomy in healthy liver transplant donor candi- dates and have a favorable impact on surgical results (3).
In our study, contrast-enhanced T1-weighted MR cholangiography after mangafodipir trisodium adminis- tration was used as an alternative method for evaluation of the biliary anatomy in a donor candidate for LRLT.
The findings were compared with those of the widely used T2-MRC procedure in terms of their ability to diag- nose the hilar ductal branching anatomy and detect in- trahepatic biliary anomalies, which would preclude sin- gle anastomosis. The additional effect of contrast-en- hanced MR cholangiography (enhanced T1-MRC) was also investigated.
Materials and Methods
Donor candidates
The study involved of 33 consecutive candidates who underwent T2-MRC and enhanced T1-MRC between April 2001 and April 2002, and were referred for exami- nation as potential living adult-to-adult liver donors.
Nine candidates underwent laparotomy and operative cholangiography, and eight underwent uncomplicated hepatectomy (right hepatectomy n=7, left extended he- patectomy, n=1). For the ninth, the transplantation was aborted because intraoperative liver biopsy revealed un- favorable fatty change; however, operative cholangiog-
raphy was performed.
Three candidates underwent endoscopic retrograde cholangiography (ERCP), and a total of 12 including the nine who underwent operative cholangiography and the three in whom ERCP was performed) underwent direct cholangiography. The outcome of this, and the operative reports were reviewed by one investigator (J.S.L.) in terms of the biliary anatomy observed and the feasibility of single duct-to-duct anastomosis.
MRI technique
All donor candidates underwent both T2-MRC and enhanced T1-MRC using a 1.5-T MRI system (Horizon;
GE Medical Systems, Milwaukee, Wis., U.S.A.) and a phased-array multicoil. Breath-hold heavily T2-weight- ed single-shot fast spin-echo MR cholangiography (T2- MRC), was performed before the administration of mangafodipir trisodium. Initially, localizer images were obtained in the coronal and transverse planes using a spoiled gradient-recalled sequence with the following parameters: repetition time, msec/echo time, msec 130/1.7, a flip angle of 90°, a field of view of 36×24-36 cm, section thickness of 10 mm with no gap, a matrix size of 256×128, and one acquisition. Subsequently, thin-section T2-weighted images were obtained using a single-shot half-Fourier rapid-acquisition and relaxation sequence (single-shot fast spin-echo) with a 260-320 mm field of view. The imaging parameters were an ef- fective echo time of 66-100 msec, a field of view of 32
×24 cm, a section thickness of 5 mm with no gap, a re- ceiver bandwidth of 31.3 kHz, a matrix size of 256×
256, and half-Fourier acquisition. In order to maintain signals from the soft-tissue structure, fat suppression was not used for this sequence. In addition, by using a spatial fat saturation technique, multisection images with a long effective echo time of 645-869 msec were obtained. All other parameters were the same as for T2- weighted images. Single thick-section images were then obtained, using the following parameters: an echo time of 830-1,050 msec; a section thickness of 30 mm; and a field of view of 24×24 cm in the coronal, lateral, and left and right 15°, 30°, and 45°oblique planes. (Eight images were obtained.)
Mangafodipir trisodium (Teslascan; Nycomed, Princeton, N.J., U.S.A.) at a standard dose of 5 μmol/kg (0.1 mL/kg; maximum dose, 15 mL) was then adminis- tered intravenously via a slow injection lasting 1-2 min prior to a 10-mL saline flush. Between 10 and 15 min af- ter injection, axial and coronal volumetric 3D spoiled
gradient-echo images of the liver and biliary system (en- hanced T1-MRC) were obtained using the following pa- rameters: TR range/TE, 5-8/minimum; flip angle, 20°; matrix, 256×128; field of view, 32-24 cm (using a rec- tangular field of view); and 4 mm slice thickness with no intersection gap.
Qualitative image evaluation
T2-MRC images and enhanced T1-MRC images were separately analyzed by two radiologists (M.J.K and J.H.K). Images from the 33 unpaired examinations were arranged in random order, and the two observers re- viewed the images from 66 examinations. The 33 paired sets of T2-MRC and enhanced T1-MRC images were then arranged randomly, and four weeks later all mem- bers of the panel reviewed all the paired sets, complet- ing a standardized data sheet.
Each reviewer recorded the anatomic type of each hi- lar bile duct branching pattern (the orthogonal relation- ships between the right anterior and posterior segmental duct, and the left and common hepatic duct), grading di- agnostic confidence on a 5-point scale (1-5). The branching pattern and confidence grade for T2-MRC and enhanced T1-MRC image sets were reviewed for each modality separately, and in combination. The con- sensus subsequently reached was based on the findings for the combined set; the results were used as the gold standard in 21 cases in which direct cholangiography or surgery was not performed. The findings of ERCP (n=3) and surgery, including intraopertive cholangiography (n=9), were used as the gold standard for the remaining cases.
In donor candidates who underwent direct cholan- giography (n=12), each reviewer used the findings of T2 MRC, enhanced T1-MRC and the combined set to deter- mine the feasibility of single duct-to-duct anastomosis for right lobe donation, respectively. The results ob- tained by the two reviewers were compared using the k statistic, and interobserver agreement thus determined.
Discrepancies were resolved by consensus, and a single conclusion thus obtained. In all these 12 candidates, the results of MRC were compared with the confirmed re- sults of direct cholangiogrphy.
Statistical analysis
To determine the anatomic type of each hilar branch- ing pattern, the accuracy of T2-MRC, T1-MRC, and the combined set were determined according to the consen- sual findings of the two reviewers. Wilcoxon’s signed
rank test was used to assess differences in diagnostic confidence, and a P value less than 0.05 was considered statistically significant. In predicting the possibility of single anastomosis, the Kappa (κ) test was used to assess interobserver variability. Agreement was categorized as follows: κvalue of 0-0.2, poor; κof 0.2-0.4, fair; κof 0.4 -0.6, moderate; κof 0.6-0.8, good; and κof 0.8- 1.0, excellent. For each method, the sensitivity , speci- ficity and accuracy of the results were calculated.
Results
Biliary variants were identified in nine (27.3%) of 33 candidates. In four of these, the anterior segmental duct drained into the left hepatic duct, and in two, drainage of the posterior segmental duct was aberrant, involving the left duct (Fig. 1). In two candidates had the common hepatic duct trifurcated into two right branches and one left hepatic duct (trifurcation) (Fig. 2), and in one, the lat- eral segmental duct drained into the right duct (Fig. 3).
Diagnostic confidence and accuracy in determining the anatomic types of hilar branching pattern
For both reviewers, the mean diagnostic confidence level was higher for enhanced T1-MRC than for T2- MRC, through the difference was not statistically signifi- cant. For T2-MRC and enhanced T1-MRC in combina- tion, however, the mean confidence level was signifi- cantly higher than for either modality alone in both re- viewer 1 and 2 (p<0.001) (Table 1). The accuracy of T2- MRC, enhanced T1-MRC, and the combined set for de- termining the anatomic types of hilar branching pattern was calculated on the basis of consensual interpretation.
The separate interpretation of T2-MRC and enhanced T1-MRC matched the consensual findings in 30 (91%)
Table 1. Diagnostic Confidence of Hilar Biliary Branching Anatomy in T2-MRC, Enhanced T1-MRC and the Combined Set for Each Reviewer
Reader 1 Reader 2 Mean grade
T2-MRC 3.52 3.64
Enhanced T1-MRC 3.97 4
Combined set 4.76 4.52
Comparison of methods
T2-MRC vs Enhanced
T1-MRC p=0.1 p=0.056
T2-MRC vs Combined set p<0.001 p<0.001 Enhanced T1-MRC vs
Combined set p<0.001 p<0.001
and 28 cases (85%) (reviewer 1), 26 (79%) and 28 cases (85%) (reviewer 2). The types of biliary anatomy deter- mined from the combined set matched the consensual interpretation in 33 (100%) and 30 (91%) cases (reviewer 1 and 2, respectively).
A C
B
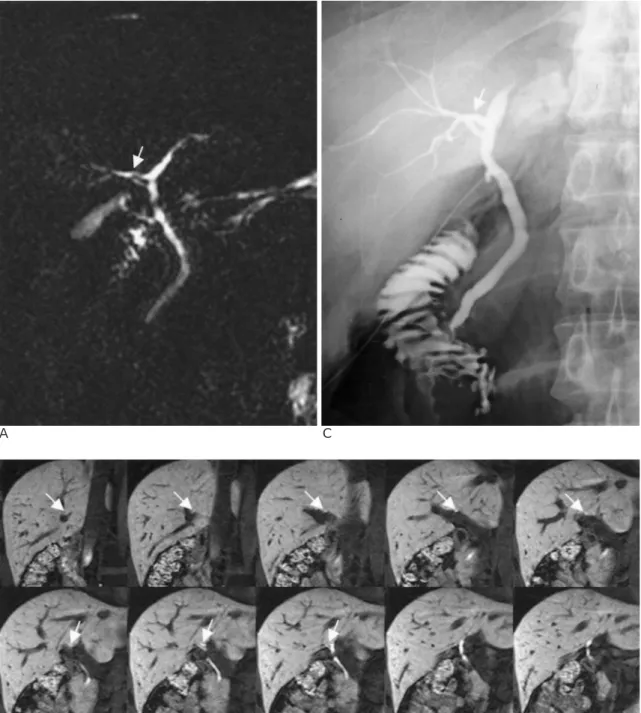
Fig. 1. Right posterior segmental duct to left hepatic duct pattern.
A. Heavily T2-weighted coronal single shot fast spin-echo thick-section MRC (∞/1004 [effective], 30-mm thickness) depicts a branch (white arrow) off left hepatic duct.
B. T1-weighted coronal enhanced T1-MRC shows right posterior segmental duct (white arrow) draining aberrantly into proximal left hepatic duct through serial image review from posterior to anterior. Diagnostic confidence of enhanced T1-MRC was higher than that of T2-MRC in both reviewers.
C. Intraoperative cholangiography confirmed this anomaly. The single anastomosis was identified to be impossible. Dual ductal anastomosis was performed in the associated recipient.
A B
C D
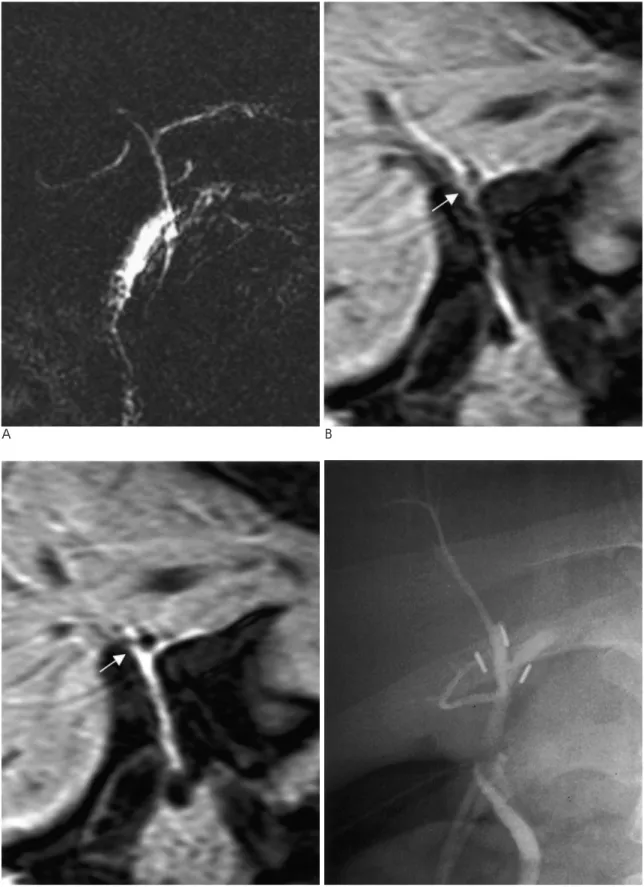
Fig. 2. Unfavorable trifurcation pattern that single anastomosis cannot be performed.
A. The junction of right posterior segmental duct and right hepatic duct cannot be accurately visualized on heavily T2-weighted single shot fast spin-echo MRC (∞/1,088 [effective], 30-mm thickness) T2-MRC was interpreted as normal biliary anatomy.
B, C. But enhanced T1-MRC depicts the unfavorable trifurcation pattern or very short right hepatic duct to disable a single duct to duct anastomosis in recipient (B is posterior to C).
D. Intraoperative cholangiography confirmed this biliary anomaly. Extended left hepatectomy was performed in this donor.
A B
C D
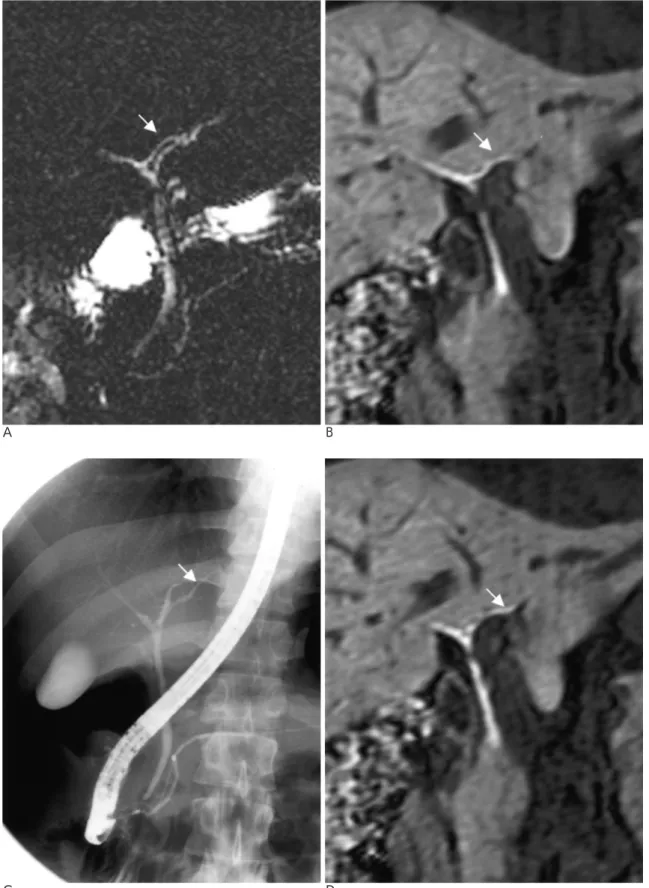
Fig. 3. Left lateral segmental duct to right hepatic duct pattern.
A. Heavily T2-weighted single shot fast spin-echo MRC (∞/995 [effective], 30-mm thickness) depicts a branch (white arrow) off right hepatic duct.
B, C. T1-weighted coronal enhanced T1-MRC shows the left lateral segmental duct (white arrow) to right hepatic duct pattern (B is posterior to C).
D. This left lateral segmental duct (white arrow) to right hepatic duct pattern well visualized on intraoperative cholangiography
Assessement of the possibility of single duct to duct anastomosis
In four of twelve cases in which direct cholangiogra- phy was performed, biliary anomalies were visualized (one case each of anterior duct to left duct, posterior duct to left duct, unfavorable trifurcation, and lateral duct to right duct). Singe duct-to-duct anastomosis for right lobe donation was found to be impossible in all four cases. In three recipients who received donations from three of four candidates with biliary anomalies, double anastomosis was performed in two cases, and left lobe transplantion in the other. Liver donation did not proceed in the candidate with lateral duct to right duct anomaly.
Overall interobserver agreement in determining the possibility of single anastomosis showed good or excel- lent agreement (κ=1.0 for T2-MRC, κ=0.657 for en- hanced T1-MRC, and κ=0.824 for the combined set).
Table 2 shows the sensitivity, specificity and accuracy of the findings, with each imaging technique assessed for possible single duct-to-duct anastomosis for right lobe donation.T2-MRC showed 100% sensitivity, 80%
specificity, and 91.6% accuracy, with no false negative cases, one false positive and seven true positives.
Enhanced T1-MRC and the combined set showed 100%
sensitivity and 100% specificity and 100% accuracy.
Discussion
Most current MRC techniques are based on variants of heavily T2-weighted fat-suppressed rapid acquisition using relaxation enhancement (RARE) pulse sequences.
The spatial resolution of current MRC techniques is, however, limited owing to the use of thick sections and blurring from the use of multiecho techniques with long echo trains. Because of relatively low spatial resolution, the depiction of intrahepatic biliary anatomy is often in- adequate in individuals without a dilated biliary system, and for this reason, a new approach to MR cholangiog- raphy which permits its accurate delineation is clearly
needed. Several studies have suggested that a new ap- proach should rely on contrast agents that are excreted into the bile ducts for delineation of intrahepatic biliary anatomy using 3D T1-weighted imaging (3, 4), and in this regard, the spatial resolution of MRC can be poten- tially improved by using rapid 3D T1-weighted gradient- echo techniques with contiguous or overlapping thin sections in which bile has been enhanced by the admin- istration of a suitable biliary contrast medium such as mangafodipir trisodium. In particular, in the preopera- tive assessment of living liver donor candidates, en- hanced T1-MRC can play an important role in the accu- rate depiction of hilar branching bile duct anatomy.
Carlos et al. (5) reported that combining T2-MRC and enhanced T1-MRC (using gadolinium-ethoxybenzyl-di- ethylenetriamine penta-acetic acid as an intrabiliary contrast agent) significantly improved biliary visualiza- tion compared with each test alone. The improvement was small, however, and the perceived added value of an intrabiliary contrast agent was modest. Their study, though, assessed the utility of the agent only in terms of ductal depiction; we tried to evaluate the added effect in terms of the confidence with which the hilar branching ductal anatomy was diagnosed during the preoperative assessment of donor candidates. Our degree of confi- dence was not significantly different between T2-MRC and enhanced T1-MRC. For reviewer 1, accuracy tend- ed to be lower for enhanced T1-MRC (91% in T2-MRC and 85% in enhanced T1-MRC) than T2-MRC, though for both reviewers, diagnostic confidence for the com- bined set was significantly higher than for T2-MRC or enhanced T1-MRC alone. With regard to accuracy, for both reviewers 1 and 2 this was also higher for the com- bined set than for T2-MRC or enhanced T1-MRC alone.
These findings suggest that the combination of images obtained at standard T2-MRC and enhanced T1-MRC improved both diagnostic confidence and accuracy in determining the anatomic type of a hilar branching pat- tern.
In donor candidates, the preoperative assessment of Table 2. Assessment of Possibility for Single Duct to Duct Anastomosis
Examination TP* TN* FP* FN* Sensitivity Specificity Accuracy
T2-MRC 7 4 1 0 100 80 91.6
T1-MRC 7 5 0 0 100 100 100
Combined set 7 5 0 0 100 100 100
* Data are numbers of patients, out of a total of 12, with false negative (FN), false positive (FP), true negative (TN), and true positive (TP) of determination on performance possibility of single anastomosis.
Sensitivity, specificity and accuracy values are cited as percentages.
hilar branching patterns is essential. Ductal anomalies such as aberrant drainage of the right posterior segmen- tal duct into the left hepatic duct or at the level of the bi- furcation (trifurcation) preclude performance of single duct-to-duct biliary anastomosis and require additional biliary anastomoses that may incur an increased risk of biliary complication (6, 7). In order to determine whether single anastomosis was possible, we therefore determined the sensitivity and specificity of each imag- ing method (T2-MRC, enhanced T1-MRC and the com- bined set), finding that the sensitivity, specificity, and accuracy of enhanced T1-MRC and the combined set were excellent. In the case of T2-MRC, the trifurcation pattern was not identified in one candidate, and single anastomosis was thus at first considered possible. On the basis of the findings of enhanced T1-MRC and the combined set, however, the reviewers considered that single anastomosis might be impossible. Intraoperative cholangiography demonstrated insufficient right hepatic duct length for single biliary anastomosis without jeop- ardizing the donor’s biliary system (Fig. 2).
Our study suffered several limitations. First, with re- gard to diagnostic confidence analysis, we found that as with many small studies examining technological ad- vances, the expected bias was toward the new tech- nique (in this case, enhanced T1-MRC). Despite this, the diagnostic confidence rate was not significantly different between T2-MRC and enhanced T1-MRC. Only the combined set showed significantly higher diagnostic confidence than either of the two modalities alone.
Second, in evaluating the possibility of single anastomo- sis, we selected from among the 33 candidates the twelve who underwent direct cholangiography. This was not perfored in those in whom on T2-MRC or en- hanced T1-MRC depicted a definitely unfavorable bil- iary anomaly, a fact which indicated selection vias.
Thirld, the combined set was in a few cases helpful in
hilar branching pattern typing and determining the fea- sibility of single anastomosis. Because of the small sam- ple size, statistical analysis was, however, limited. In the future, further data collection from a larger number of subjects may help determine whether findings for the combined set are likely to have a favorable impact on surgical results. However, we believe our study is the first to focus on the clinical application of enhanced T1- MRC to a situation in which donor candidates for living related liver transplantation are assessed.
In conclusion, enhanced T1-MRC has the potential to enhance the reliability of the preoperative evaluation of hilar biliary anatomy in donor candidates or to lessen the occurrence of a non-diagnostic or equivocal interpre- tation at T2-MRC alone.
References
1. Morgan GR, Lee V, Krinsky G, et al. Duct to duct biliary anasto- mosis with t-tube drainage in adult right lobe living donor liver transplantation without bile leaks. (abstr) Hepatology 2000;32:
214A
2. Hintze RE, Adler A, Veltzke W, et al. Clinical significance of mag- netic resonance cholangiopancreatography (MRCP) compared to endoscopic retrograde cholangiopancreatography (ERCP).
Endoscopy 1997;29:182-187
3. Lee VS, Rofsky NM, Morgan GR, et al. Volumetric mangafodipir trisodium-enhanced cholangiography to define intrahepatic biliary anatomy. AJR Am J Roentgenol 2001;176:906-908
4. Mitchell DG, Alam F. Mangafodipir trisodium: effects on T2- and T1-weighted MR cholangiography. J Magn Reson Imaging 1999;9:
366-368
5. Carlos RC, Hussain HK, Song JH, Francis IR. Gadolinium- Ethoxybenzyl-Diethylenetriamine Pentaacetic Acid as an intrabil- iary contrast agent: preliminary assessment. AJR Am J Roentgenol 2002;179:87-92
6. Marcos A, Fisher RA, Ham JM, et al. Selection and outcome of liv- ing donors for adult to adult right lobe transplantation.
Transplantation 2000;69:2410-2415
7. Marcos A, Ham JM, Fisher RA, Olzinski AT, Posner MP. Single- center analysis of the first 40 adult-to-adult living donor liver trans- plants using the right lobe. Liver Transpl 2000;6:296-301
대한방사선의학회지 2004;50:185-193
생체 부분 간이식 공여자의 술전 담문계 해부학적 변이에 관한 T2강조 및 조영증강 T1강조 담도조영술간의 진단적 유용성 비교
11연세대학교 의과대학 진단방사선과학교실
2연세대학교 의과대학 외과학교실
3연세대학교 의과대학 BK21 의학
임준석1・김명진1,3・김경식2・김주희1・오영택1・김진용1・유형식1・이종태1・김기황1
목적: 생체 부분 간이식 공여자의 담문계 해부학적 변이 진단에 관한 T2 강조 자기공명담관조영술(T2-MRC)과 조영 증강 T1강조 조영술(CE-MRC)의 유용성을 비교 분석하였다.
대상과 방법: 33명의 간이식 공여 후보자를 대상으로 하였으며, T2-MRC는 단발포급속스핀에코 방법을 이용하여 획 득되었으며, 5 mm두께의 관상면 영상과, 총담관을 중심으로 여러 각도의 단일 절편영상을 얻었다. CE-MRC는 mangafodifir trifodium을 주사후, 삼차원 GRE sequence를 사용하여, 축상면과 관상면 영상을 얻었다. 두 명의 방사선 과 의사가, T2-MRC와 CE-MRC를 각각 분리하여 본 경우와 모두 본 경우를 구분하여, 담문계 해부학적 변이와 진단 신뢰도를 기록하였으며, consensus reading을 기준으로 각 방법의 해부학적 변이 진단의 정확도를 비교하였다. 특히 직접 담관 조영술을 시행한 12예에서는 단일 담관계 문합의 수행가능성 여부를 판단하였으며, 이를 직접 담관 조영술 의 결과와 비교하였다.
결과과: 담문계 해부학적 변이 진단에 있어 두 평가자의 진단 신뢰도는 T2-MRC보다 CE-MRC에서 높은 양상을 보였으 나, 통계학적 차이는 없었다. T2와 T1강조 MRC를 모두 본 경우에는 두 평가자 모두 각각의 영상을 따로 본 경우 보다, 통계학적으로 더 높은 진단 신뢰도를 보였다(p<0.001). 두 영상을 같이 본 경우 두 평가자는 consensus reading과 각 각 33(100%), 30(91%) 예에서 일치된 결과를 보였으며, T2-MRC와 CE-MRC를 따로 본 경우 두 평가자에서 T2- MRC: 30(91%), CE-MRC: 28(85%) 그리고 T2-MRC: 26(79%), CE-MRC: 28(85%)의 일치된 결과를 보였다.
직접 담관 조영술을 시행한 12예에서의 단일 담관 문합술의 수행가능성 예측 정확도는 T2-MRC: 91.6% CE-MRC:
100% 그리고 paired set: 100% 였다.
결론: 생체 부분 간이식 공여자의 술전 담관계 해부학적 변이 진단에 T2-MRC와 T1-MRC를 모두 시행함으로써 진단 신뢰도와 정확도를 향상시킬 수 있다.