서론
무릎수술 후 일반적으로 대퇴근육의 약화, 통증 및 기능감 소가 나타나고, 수술로 인한 하지 근력의 불균형은 무릎관절 의 불안정성을 초래하며, 이에 따른 체중분포의 불균형은 보 행이나 앉았다 일어서기와 같은 일상활동 수행을 어렵게 하 는 원인이 된다[1]. 그러므로 대퇴부 근력의 안정화를 위한 재활치료는 무릎의 기능과 안정성 회복에 필수요소이다[2].전방십자인대재건술(anterior cruciate ligament
recon-struction, ACLR) 후 재활치료의 주된 목적은 염증 감소, 신 경근 근력 및 기능 회복, 관절 가동범위 회복과 환자의 일상 생활로의 복귀에 있으며, 대퇴부 근육과 넙다리뒤근육뿐 아 니라 고유감각의 운동패턴이 전방십자인대 수술 후 재활치료 에 중요한 역할을 한다[3]. ACLR 후 치료원칙은 수술 후 첫 날부터 적극적인 재활을 시행하는 것이다. 냉치료와 압박, 거 상의 조기 사용이 술 후 부종을 감소시키며, 술 후 수일 내에 완전 수동신전과 능동굴곡을 시행하는 것이 매우 중요하다. 재활의 빠른 진행은 수술과 관련된 관절경직, 근약화와 위축, 대퇴슬개 통증 등의 합병증을 감소시키며, 초기 재활에서 가 장 중요한 것은 재건된 인대에 부하를 주는 슬관절 신전 마지 막 30° 이내에서 열린 사슬의 저항 대퇴사두근 신전운동을 피 하는 것이다. 부력을 줄 수 있는 수중운동은 봉합사가 제거되 자마자 가능한 빨리 시행하여 점진적인 체중부하를 유도한다. 개인에 따라 정상적인 관절가동범위나 근력, 고유수용감각,
무릎수술 후 신경근전기자극치료: 체계적 문헌고찰
윤 진 희·조 선 영·김 석 현 | 한국보건의료연구원 신의료기술평가사업본부Neuromuscular electrical stimulation therapy
after knee surgery: a systematic review
Jin Hee Yoon, MS · Sunyoung Jo, MS · Seok-Hyun Kim, MD
Division for New Health Technology Assessment, National Evidence-based Healthcare Collaborating Agency, Seoul, Korea
Received: May 3, 2017 Accepted: May 19, 2017 Corresponding author: Seok-Hyun Kim
E-mail: [email protected] © Korean Medical Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons. org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
The recovery of quadriceps muscle strength and knee function after knee surgery is important. Recently, neuro-muscular electrical stimulation (NMES), which is a method in which an electrical current is applied to the surrounding targeted muscle, has been incorporated into muscle-strengthening programs. The objective of this review was to evaluate the safety and effectiveness of NMES in patients who have undergone knee surgery. A database search was performed in 8 Korean databases, Medline, Embase, and the Cochrane Library. Article selection and quality assessment were performed by 2 reviewers. Of the 580 articles selected, 14 papers (randomized controlled trials) were included in the final assessment. In the results of the meta-analysis, NMES combined with rehabilitation demonstrated a significant improvement in the enhancement of quadriceps muscle strength after anterior cruciate ligament reconstruction. On the basis of the currently available data, NMES with rehabilitation is associated with favorable outcomes, and should be considered a safe and effective procedure for enhancing quadriceps muscle strength.
운동 특이적 기술회복에 걸리는 속도는 다르며, 일반적으로 조기 재활프로그램을 통해 술 후 6개월 정도면 운동복귀가 가능해진다[4]. 슬관절 전치환술 후 재활은 수술 전에 무릎기 능을 평가하고 수술 후 재활치료 과정을 이해시키고 운동방 법들을 교육하는 것을 목적으로, 통증 정도, 관절 구축, 관절 가동범위, 내반슬, 무릎 주위 근력과 보행양항 승을 평가하여 수술 화 재활과정에 참고해야 한다. 재활치료 과정은 수술 후 초기 운동을 시작으로 지속적 수동운동, 기능 회복기 재활운 동, 슬관절 성형술 후 일상생활동작 훈련 및 스포츠활동의 순 서대로 진행된다[4].
신경근전기자극치료(neuromuscular electrical stimu-lation therapy, NMES)는 무릎 수술 후 전통적 치료에 더 해 추가 이득을 줄 수 있는 것으로 알려져 있다[3]. 슬관절 전 치환술을 받은 환자 중 NMES와 대퇴사두근의 강한 운동이 동반된 실험군이 대퇴사두근의 운동만 실시된 대조군과 비 교하여 근력과 운동 회복에 더 효과적이라는 연구가 보고된 바 있고[5], ACLR을 받은 환자를 대상으로 한 비교연구에서 는 대퇴사두근의 근력과 무릎기능 개선이 있었다고 보고되었 다[3]. 반면에, ACLR 후 운동치료 단독 및 NMES를 병용했 을 때 군간 유의한 차이가 없다는 연구결과도 보고되었다[6]. 본 연구에서는 무릎수술 후 대퇴부근육 강화 및 무릎기능 개선에 있어 NMES의 안전성 및 유효성을 체계적 문헌고찰 을 통해 검토한 후, 임상의와 환자들의 의사결정에 도움을 줄 수 있는 객관적 근거를 제공하고자 한다. 상세한 내용은 신의료기술평가본부 홈페이지(http://nhta.neca.re.kr)를 통해 확인이 가능하다.
연구방법
1. 연구설계 본 연구는 무릎수술을 받은 환자를 대상으로 NMES를 시 행하였을 때의 안전성과 유효성을 체계적 문헌고찰 및 메 타분석을 이용하여 확인하였다. PICO (patients-interven-tion-comparator-outcome)는 전문가 논의를 거쳐 다음과 같이 선정하였다. 대상환자는 무릎수술을 받은 환자로 중재 시술은 NMES, 비교시술은 재활치료·무치료·placebo-NMES를 포함하였고, 의료결과는 안전성으로 시술 관련 합 병증을 유효성으로는 대퇴부근육지수, 무릎기능지수, 보행 지수, 무릎통증지수를 평가하였다. 2. 문헌검색 문헌검색은 KoreaMed, 국립중앙도서관, 국회도서관, 국 가자료공동목록시스템, 학술연구정보서비스, 학술데이터베 이스검색, 과학기술학회마을, 한국의학논문데이터베이스의 8개 국내 데이터베이스와 Medline, Embase 및 Cochrane Library의 국외 데이터베이스를 이용하여 2015년 9월 14일 에 최종 검색을 완료하였다. 문헌검색 시 사용한 검색어는 국내데이터베이스의 경우 ‘neuromuscular electrical sti-mulation,’ ‘NMES,’ ‘신경근전기자극’의 검색어로 광범위하 게 검색한 후, 수작업으로 불필요한 문헌을 배제하였다. 국 외데이터베이스는 ‘anterior cruciate ligament,’ ‘posterior cruciate ligament,’ ‘total knee arthroplasty,’ ‘knee surgery’ 등 무릎수술 관련 적응증과 ‘electric stimulation,’ ‘NMES’ 등 중재시술을 포괄하는 검색어를 ‘AND’로 검색하였다. 3. 문헌선택 본 연구의 목적에 적합한 문헌을 선택하기 위하여 두 단계 의 과정을 수행하였다. 첫 번째 과정은 각 데이터베이스에서 검색된 문헌의 중복여부를 색인하였고, 다음으로 중복검색이 제거된 문헌을 대상으로 문헌선택 및 배제기준에 의거하여 2 명의 평가자가 각각 독립적으로 문헌의 선택과 배제를 수행하 였다. 평가자간 이견이 있을 경우 의견조정을 통해 선택여부 를 결정하였으며, 의견합치가 되지 않을 경우 전문가 회의를 통해 조정하였다. 문헌의 선택기준은 무릎수술 환자를 대상으 로 NMES를 수행한 연구와 적절한 의료결과가 하나 이상 보고 된 연구였다. 배제기준은 동물실험 및 전임상시험 연구, 원저 가 아닌 연구(non-systematic reviews, editorial, comment, opinion pieces, review, congress or conference material, guideline, note, news article, abstract, etc.), 비교시술이 없 는 연구(무치료, placebo 제외), 한국어 및 영어로 출판되지 않 은 연구, 무작위 임상시험이 수행되지 않은 연구였다.4. 문헌의 질 평가
선택된 문헌의 질 평가 도구는 영국 SIGN (Scottish Inter- collegiate Guidelines Network)의 방법론 점검표를 사용하
였다. 문헌의 질 평가는 2명의 평 가자가 독립적으로 수행하였고, 이 에 따른 판정결과에 대한 합의를 거쳐 조정하였다. 근거의 수준은 Table 1에 제시하였다. 5. 자료추출 자료추출은 평가에 필요한 모든 자료를 추출하기 위하여 기본 서식 을 작성하여 시범적으로 몇 개의 문 헌을 통해 서식이 적절한지 평가하 였으며, 유효성에서 1차 의료결과는 대퇴부 근육지수로, 그 외의 지표는 2차 의료결과로 구분하여 자료를 추출하였다. 문 헌마다 다르게 보고된 용어는 자료추출 과정에서 통일하였으 며, 자료추출에 대한 내용은 자문회의를 통해 확인하였다. 6. 메타분석 의료결과 중, 자문회의를 통하여 대퇴부 근육지수와 무릎 기 능지수에 대하여 메타분석(Comprehensive Meta Analysis; Biostat, Englewood, NJ, USA)을 시행하였다. 각 연구마다 중재결과를 다른 측정도구로 측정하여 단위가 동일하지 않기 때문에 표준평균편차(standardized mean difference, SMD) 값을 이용하였으며, 적응증 종류와 중재 시점으로 구분하여 분석을 실시하였다.
결과
1. 연구에 선택된 문헌 문헌검색전략에 따라 검색된 문헌은 총 580편(국내 1편, 국외 579편)이었고, 중복검색을 제거한 449편(국내 1편, 국외 448편)에 대 하여 선택 및 배제기준을 적용하여 최종적으로 선택된 문헌 은 무작위 임상시험연구 총 14편(국내 1편, 국외 13편)이었 다(Figure 1). 근거의 수준은 모든 문헌에 ‘+’를 부여하였으Table 1. SIGN criteria for assignment of levels of evidence
Level Description
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias 1+ Well conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias 1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort studies High quality case control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is
causa
2+ Well conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causa
3 Non-analytic studies, e.g. case reports, case series 4 Expert opinion
SIGN, Scottish Intercollegiate Guideline Network; RCT, randomized controlled trial.
Table 2. SIGN criteria for assignment of grades of recommendation
Level Description
A At least one meta-analysis, systematic review, or randomized controlled trial rated as 1++, and directly applicable to the target population; or A body of evidence consisting principally of studies
rated as 1+, directly applicable to the target population, and demonstrating overall consistency of results
B A body of evidence including studies rated as 2++, directly applicable to the target population, and demonstrating overall consistency of results; or Extrapolated evidence from studies rated as 1++ or 1+ C A body of evidence including studies rated as 2+, directly applicable to the target population and
demonstrating overall consistency of results; Extrapolated evidence from studies rated as 2++ D Evidence level 3 or 4; or Extrapolated evidence from studies rated as 2+
SIGN, Scottish Intercollegiate Guideline Network. Selected studies
(n=14)
Exclusion • Duplicated studies (n=131) • Animal or pre-clinical studies
(n=6)
• Non-original articles (n=143) • Not published in Korean or
English (n=31) • Gray literatures (n=57) • Not performed appropriate
method (n=163) • No comparators (n=18) • Not reported outcomes of
interest (n=13) • Non-RCT (n=4) Identified studied through
electronic searches of databases (n=580)
Figure 1. Flow diagram of the study selection process. RCT, randomized
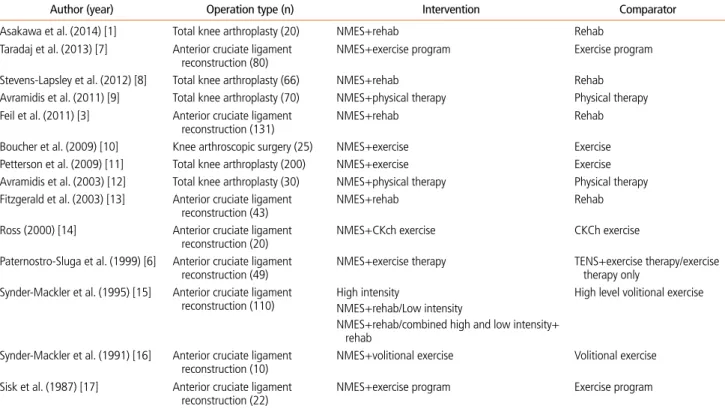
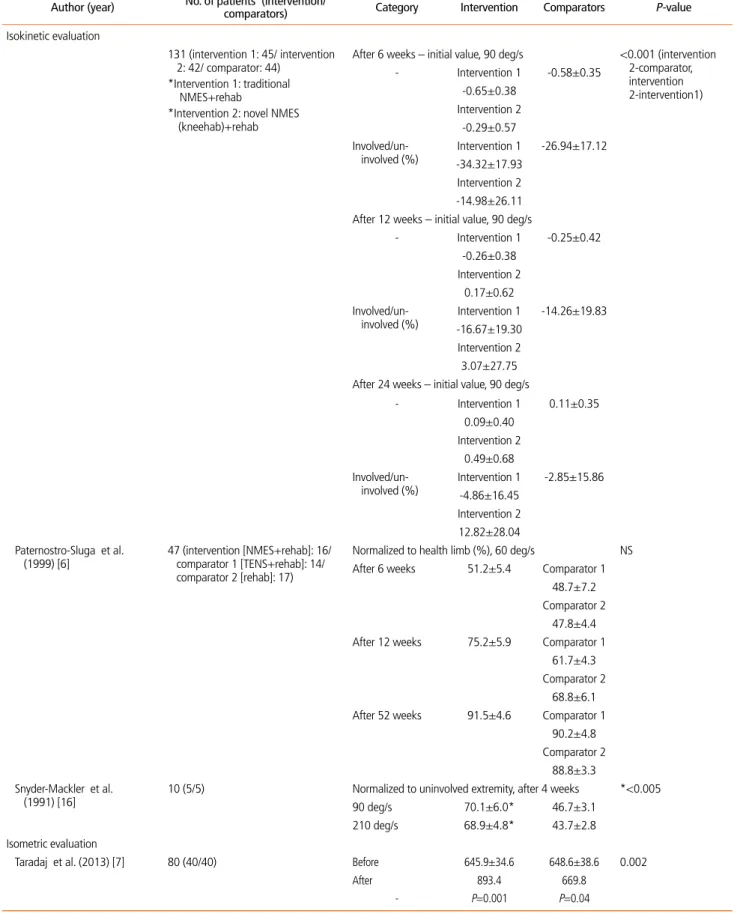
며, 근거 수준에 따른 권고등급은 Table 2와 같다. 선택된 문헌은 출판연도, 제1저자 성명을 알파벳순으로 정리하였다 (Table 3) [1,3,6-17]. 2. 안전성 및 유효성 평가 결과 NMES의 안전성은 시술 관련 합병증으로 평가하였다. 2편 의 문헌에서 중재시술 관련 부작용이나 합병증이 발생하 지 않았다고 언급하였고, 그중 1편의 문헌에서 첫 중재시술 시 1명의 환자가 약간의 어지러움을 느꼈다고 보고하였다. NMES의 유효성은 1차 의료결과로 대퇴부근육지수, 2차 의료결과로 무릎기능지수, 보행지수, 무릎통증지수를 연 구대상의 적응증별로 구분하여 평가하였다. 대퇴부근육 지수를 보고한 문헌은 11편으로, 등속성 평가결과로 대 퇴부근력을 보고한 문헌은 3편이었다(Table 4) [1,3,6-8,10,11,13,15-17]. Traditional NMES+재활프로그램 (중재군1, NMES 12주), new NMES+재활프로그램(중재 군2)과 재활프로그램 단독 시행(대조군) 후의 대퇴부근력 을 평가한 1편의 문헌에서는 90 deg/s에서 ‘6주 후-초기 값,’ ‘12주 후-초기값,’ ‘24주 후-초기값’을 각각 중재군1 –0.65±0.38, -0.26±0.38, 0.09±0.40 N·m/kg, 중재 군2 –0.29±0.57, 0.17±0.62, 0.49±0.68 N·m/kg, 대 조군 –0.58±0.35, -0.25±0.42, -2.85±15.86 N·m/kg 으로 보고하였으며, 중재군2는 중재군1, 대조군과 비교하 여 유의한 차이가 있었다(P<0.001). NMES+재활프로그 램(중재군, 6주 자극)과 경피적 전기신경자극+재활프로그 램(대조군1), 재활프로그램 단독 시행(대조군2) 후의 대퇴 부근력을 평가한 1편의 문헌에서는 60 deg/s에서 수술 받 지 않은 다리와의 표준화 결과 6주/12주/52주 시점에서 의 근육지수는 중재군 51.2±5.4/75.2±5.9/91.5±4.6%, 대조군1 48.7±7.2/61.7±4.3/90.2±4.8%, 대조군2 47.8±4.4/68.8±6.1/88.8±3.3%로 군간 유의한 차이는 없 었다. NMES+재활프로그램(4주 자극)과 재활프로그램 단 독 수행 후 수술 받지 않은 다리와의 표준화 결과 90 deg/ s에서 중재군 70.1±6.0%, 대조군 46.7±3.1%로 군간 유 의한 차이가 있었다(P<0.05). 등척성 평가결과를 보고한 7 편의 문헌 중 4편의 문헌에서 군간 유의한 차이가 있었고
Table 3. Study characteristics of included studies
Author (year) Operation type (n) Intervention Comparator
Asakawa et al. (2014) [1] Total knee arthroplasty (20) NMES+rehab Rehab
Taradaj et al. (2013) [7] Anterior cruciate ligament
reconstruction (80) NMES+exercise program Exercise program
Stevens-Lapsley et al. (2012) [8] Total knee arthroplasty (66) NMES+rehab Rehab
Avramidis et al. (2011) [9] Total knee arthroplasty (70) NMES+physical therapy Physical therapy Feil et al. (2011) [3] Anterior cruciate ligament
reconstruction (131) NMES+rehab Rehab
Boucher et al. (2009) [10] Knee arthroscopic surgery (25) NMES+exercise Exercise
Petterson et al. (2009) [11] Total knee arthroplasty (200) NMES+exercise Exercise
Avramidis et al. (2003) [12] Total knee arthroplasty (30) NMES+physical therapy Physical therapy Fitzgerald et al. (2003) [13] Anterior cruciate ligament
reconstruction (43) NMES+rehab Rehab
Ross (2000) [14] Anterior cruciate ligament
reconstruction (20) NMES+CKch exercise CKCh exercise
Paternostro-Sluga et al. (1999) [6] Anterior cruciate ligament
reconstruction (49) NMES+exercise therapy TENS+exercise therapy/exercise therapy only Synder-Mackler et al. (1995) [15] Anterior cruciate ligament
reconstruction (110) High intensity NMES+rehab/Low intensity
NMES+rehab/combined high and low intensity+ rehab
High level volitional exercise
Synder-Mackler et al. (1991) [16] Anterior cruciate ligament
reconstruction (10) NMES+volitional exercise Volitional exercise Sisk et al. (1987) [17] Anterior cruciate ligament
reconstruction (22) NMES+exercise program Exercise program
Table 4. Summary of results - quadriceps muscle strength
Author (year) No. of patients (intervention/comparators) Category Intervention Comparators P-value Isokinetic evaluation
131 (intervention 1: 45/ intervention 2: 42/ comparator: 44)
*Intervention 1: traditional NMES+rehab
*Intervention 2: novel NMES (kneehab)+rehab
After 6 weeks – initial value, 90 deg/s <0.001 (intervention 2-comparator, intervention 2-intervention1) - Intervention 1 -0.58±0.35 -0.65±0.38 Intervention 2 -0.29±0.57 Involved/un- involved (%) -34.32±17.93Intervention 1 -26.94±17.12 Intervention 2 -14.98±26.11 After 12 weeks – initial value, 90 deg/s
- Intervention 1 -0.25±0.42 -0.26±0.38 Intervention 2 0.17±0.62 Involved/un- involved (%) -16.67±19.30Intervention 1 -14.26±19.83 Intervention 2 3.07±27.75 After 24 weeks – initial value, 90 deg/s
- Intervention 1 0.11±0.35 0.09±0.40 Intervention 2 0.49±0.68 Involved/un- involved (%) Intervention 1-4.86±16.45 -2.85±15.86 Intervention 2 12.82±28.04 Paternostro-Sluga et al.
(1999) [6] 47 (intervention [NMES+rehab]: 16/ comparator 1 [TENS+rehab]: 14/ comparator 2 [rehab]: 17)
Normalized to health limb (%), 60 deg/s NS After 6 weeks 51.2±5.4 Comparator 1
48.7±7.2 Comparator 2
47.8±4.4 After 12 weeks 75.2±5.9 Comparator 1
61.7±4.3 Comparator 2
68.8±6.1 After 52 weeks 91.5±4.6 Comparator 1
90.2±4.8 Comparator 2
88.8±3.3 Snyder-Mackler et al.
(1991) [16] 10 (5/5) Normalized to uninvolved extremity, after 4 weeks90 deg/s 70.1±6.0* 46.7±3.1 *<0.005
210 deg/s 68.9±4.8* 43.7±2.8
Isometric evaluation
Taradaj et al. (2013) [7] 80 (40/40) Before 645.9±34.6 648.6±38.6 0.002
After 893.4 669.8
- P=0.001 P=0.04
(P<0.05), 이 중 1편의 문헌에서는 저강도 NMES+재활프 로그램을 받은 군은 대조군과 유의한 차이가 없었다. 나머 지 3편의 문헌은 군간 유의한 차이가 없는 것으로 보고하였 다. 도수근력검사를 수행한 1편의 문헌에서는 군간 유의한 차이가 있었다(P<0.05). 메타분석결과 ACLR을 받은 환 자(6편)와 슬관절 전치환술을 받은 환자(2편) 모두 중재군 에서 대퇴부근육지수의 유의한 개선효과를 보였다(SMD, ACLR: 0.595 [0.148-1.042, 이질성: 70.5%]; 슬관절 전 치환술: 0.522 [0.046-0.999, 이질성: 10.5%]) (Figure 2) [1,3,6-8,13,16,17]. NMES 적용 후 3개월 이전 시점에 서의 메타분석 결과는 ACLR을 받은 환자(6편)와 슬관절 전치환술을 받은 환자(2편) 모두 중재군에서 대퇴부근육지 수 개선에 유의한 효과를 보였으며(SMD, ACLR: 0.652 [0.181-1.124, 이질성: 73.2%], 슬관절 전치환술: 0.528 [0.047-1.008, 이질성: 8.1%]), 3개월 이후 시점에서는 ACLR을 받은 환자(3편) 중, 중재군에서 대퇴부근육지수 개선에 유의한 효과를 보였고(SMD 0.430 [0.053-0.808, 이질성: 44.0%]), 슬관절 전치환술을 받은 환자에서는 유 의한 효과를 보이지 않았다(SMD 0.332 [-0.202–0.867, 이질성: 0%]). 무릎기능지수는 총 5편의 문헌에서 보고하였으며, 1편 의 문헌에서 6주차의 American Knee Society Score와,
Table 4. (Continued)
Author (year) No. of patients (intervention/comparators) Category Intervention Comparators P-value
Stevens-Lapsley et al. (2012) [8] 66 (35/31) Before 1.33±0.57 1.32±0.49 *<0.05
After 3.5 weeks* 0.93±0.41 0.66±0.24 After 6.5 weeks 1.20±0.47 1.04±0.35 After 13weeks 1.42±0.52 1.20±0.42 After 26 weeks 1.51±0.48 1.39±0.44
After weeks* 1.66±0.52 1.50±0.43
Boucher et al. (2009) [10] 25 (15/10) Involved 83.7±37.3 91.9±54.3 NS
Uninvolved 111.7±37.4 125.6±57.4 Peak torque index 73.5±18.3 71.2±26.9
Petterson et al. (2009) [11] 200 (100/100) 0 month 10.42 10.58 NS
3 month 19.05 17.35
12 month 22.64 20.60
0-3 month (%) 83 64
3-12 month (%) 19 19
0-12 month (%) 117 95
Fitzgerald et al. (2003) [13] 43 (21/22) After 12 weeks 75.9±16.8* 67.0±19.9 *<0.05
After 16 weeks 83.1±15.6* 75.0±17.8 Snyder-Mackler et al. (1995)
[15] 110 (Intervention 1: High intensity NMES+rehab 31/ Intervention 2: Low intensity NMES+rehab 25/ Intervention 3: High and Low intensity NMES + rehab 20/ Comparator: rehab 34)
After 6 weeks Intervention 1 Comparator
-70 57
Intervention 2 51 Intervention 3
70
Sisk et al. (1987) [17] 22 (11/11) After 7 weeks 0.73±0.41 NS
After 8 weeks 0.90±0.44 After 9 weeks 1.11±0.63 Manual muscle testing
Asakawa et al.(2014) [1] 20 (10/10) Before 87.93±8.62 91.9±11.41 <0.05
After 114.1±19.71 96.49±17.44
- P=0.001 P=0.420
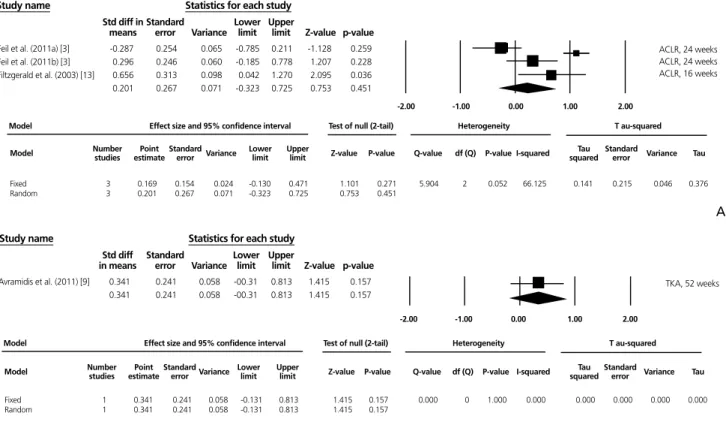
6주/12주차의 The Oxford Knee Score가 중재군에서 유 의한 무릎기능지수의 개선이 있었고, 1편의 문헌에서 10 주차의 Activities of Daily Living Scale이 중재군에서 유 의한 개선이 있었다. 나머지 3편의 문헌에서는 Lysholm Score, Lower Extremity Functional Scale, Hospital for Special Surgery Knee Score에서 군간 유의한 차이가 없 었다. 전체 환자에서 메타분석 결과 NMES 후 12주 시점의 무릎기능지수는 군간 유의한 차이가 없었으며, 적응증별로 분석한 결과, ACLR을 받은 환자에서는 유의한 차이가 없 었고, 슬관절 전치환술을 받은 환자에서는 중재군에서 무 릎기능지수의 유의한 개선효과가 있었다. 12주 이후 시점 에서는 전체 환자, ACLR을 받은 환자, 슬관절 전치환술을 받은 환자 모두에서 군간 유의한 차이가 없었다(Figure 3) [3,9,13]. 모든 보행지수는 6편의 문헌에서 보고하였으며, 1편의 문 헌에서 Timed Up & Go Test, Stair-Climbing Test, Six-Minute Walk test에서 군간 유의한 차이가 없었고, 나머지
5편의 문헌에서는 Timed Up & Go Test, Stair-Climbing Test, Six-Minute Walk test, Walking Speed Score, Walking Distance, Lateral Step-Up Test, Stance Time of Involved Limb, Cadence, Walking Velocity에서 군간 유의한 차이가 있는 것으로 보고하였다. 무릎통증지수는 총 5편의 문헌을 근거로 평가하였으며, 중재 후 군간 유의한 차 이가 있다고 보고한 문헌은 없었다.
결론
NMES는 십자인대 및 무릎인공관절 수술 전후 대퇴부근 육 강화 및 무릎 안정성 개선을 위해 의료용 전극을 대퇴부 에 부착하여 전기자극을 가하는 시술로, 본 연구는 동 시술 이 안전하고 유효한 시술인지 여부를 파악하기 위하여 수 행되었다. NMES의 안전성 및 유효성 검토결과, 동 시술의 부작용이나 합병증을 보고한 문헌이 없으므로 안전성에는Figure 2. Results of meta-analysis for quadriceps indices. (A) Anterior cruciate ligament reconstruction (ACLR) and (B) Total knee arthroplasty (TKA).
A
Study name
Feil et al. (2011a) [3] -0.025 0.241 0.058 -0.497 0.447 -0.103 0.918 Feil et al. (2011b) [3] 0.795 0.247 0.061 0.312 1.279 3.225 0.001 Fitzgerald et al. (2003) [13] 0.482 0.309 0.096 -0.124 1.089 1.558 0.119 Paternostro-sluga et al. (1999) [6] 0.693 0.359 0.129 -0.010 1.359 1.931 0.053 Sisk et al. (1987) [17] 0.084 0.427 0.182 -0.753 0.920 0.196 0.845 Snyder-Macket et al. (1991) [16] 4.900 1.265 1.601 2.420 7.380 3.873 0.000 Taradaj et al. (2013) [7] 0.715 0.231 0.053 0.263 1.167 3.100 0.002 0.595 0.228 0.052 0.148 1.042 2.609 0.009
Model Number Point Standard Variance Lower Upper Z-value P-value studies estimate error limit limit Q-value df (Q) P-value I-squared Tau Standard squared error Variance Tau Model Effect size and 95% confidence interval Test of null (2-tail) Heterogeneity T au-squared
Fixed 7 0.521 0.114 0.013 0.298 0.745 4.568 0.000 20.353 6 0.002 70.520 0.231 0.204 0.042 0.480 Random 7 0.595 0.228 0.052 0.148 1.042 2.609 0.009
Statistics for each study Std diff in
means Standarderror Variance Lowerlimit Upperlimit Z-value p-value
ACLR, 55 and Under ACLR, 55 and Under ACLR, 55 and Under ACLR, 55 and Under ACLR, 55 and Under ACLR, 55 and Under ACLR, 55 and Under
8.00 4.00 0.00 -4.00 -8.00 B Study name Asakawa et al. (2014) [1] 0.946 0.472 0.222 0.022 1.871 2.007 0.045 Stevens-Lapsley et al. (2012) [8] 0.383 0.249 0.062 -0.105 0.871 1.538 0.124 0.522 0.243 0.059 0.046 0.999 2.147 0.032
Statistics for each study Std diff in
means Standarderror Variance Lowerlimit Upperlimit Z-value p-value
TKA, 60 and Under TKA, over 60
Model Number studies estimate Point Standard Variance Lower Upper error limit limit Z-value P-value Q-value df (Q) P-value I-squared squared Tau Standard error Variance Tau Model Effect size and 95% confidence interval Test of null (2-tail) Heterogeneity T au-squared
Fixed 2 0.505 0.220 0.048 0.074 0.937 2.297 0.022 1.117 1 0.291 10.428 0.017 0.225 0.050 0.129 Random 2 0.522 0.243 0.059 0.046 0.999 2.147 0.032 8.00 4.00 0.00 -4.00 -8.00
문제가 없는 것으로 판단된다. 또한, 메타분석 결과 ACLR 을 받은 환자에서 재활치료 시 NMES를 적용하였을 때 중 재군에서 대퇴부근육지수가 유의한 개선을 보였으므로 동 시술은 ACLR을 받은 환자의 대퇴부근력 강화에 있어 안전 성 및 유효성이 있는 것으로 평가하였다(권고등급 B). 다 만, 슬관절 전치환술을 받은 환자의 경우 NMES를 적용하 였을 경우 3개월 이전 시점에서는 중재군에 효과가 있는 것 으로 나타났으나, 선택문헌 및 전문가 자문 의견에 따라 군 간 유의한 차이가 없다는 대규모 연구가 메타분석에 포함 되지 않아 중재시술의 효과를 단정하기 어려운 것으로 평 가하였다.
Acknowledgement
This study was supported by research funds of the Ministry of Health and Welfare.
찾아보기말: 신경근전기자극치료; 전방십자인대재건술; 대퇴사두근력
ORCID
Jin Hee Yoon, http://orcid.org/0000-0003-0544-8878 Sunyoung Jo, http://orcid.org/0000-0002-7394-1050 Seok-Hyun Kim, http://orcid.org/0000-0003-1714-9824
REFERENCES
1. Asakawa Y, Jung JH, Koh SE. Neuromuscular electrical stimu-lation improves strength, pain and weight distribution on patients with knee instability post surgery. Phys Ther Rehabil Sci 2014;3:112-118.
2. Frost H, Lamb SE, Robertson S. A randomized controlled trial of exercise to improve mobility and function after elective knee arthroplasty: feasibility, results and methodological diffi-culties. Clin Rehabil 2002;16:200-209.
3. Feil S, Newell J, Minogue C, Paessler HH. The effectiveness of supplementing a standard rehabilitation program with super-imposed neuromuscular electrical stimulation after anterior cruciate ligament reconstruction: a prospective, randomized, single-blind study. Am J Sports Med 2011;39:1238-1247.
Figure 3. Results of meta-analysis for knee function indices. (A) Anterior cruciate ligament reconstruction (ACLR) and (B) Total knee arthroplasty (TKA).
A
Study name
Feil et al. (2011a) [3] -0.287 0.254 0.065 -0.785 0.211 -1.128 0.259 Feil et al. (2011b) [3] 0.296 0.246 0.060 -0.185 0.778 1.207 0.228 Filtzgerald et al. (2003) [13] 0.656 0.313 0.098 0.042 1.270 2.095 0.036 0.201 0.267 0.071 -0.323 0.725 0.753 0.451
Statistics for each study Std diff in
means Standarderror Variance Lowerlimit Upperlimit Z-value p-value
ACLR, 24 weeks ACLR, 24 weeks ACLR, 16 weeks
Model Effect size and 95% confidence interval Test of null (2-tail) Heterogeneity T au-squared
Fixed 3 0.169 0.154 0.024 -0.130 0.471 1.101 0.271 5.904 2 0.052 66.125 0.141 0.215 0.046 0.376 Random 3 0.201 0.267 0.071 -0.323 0.725 0.753 0.451 2.00 1.00 0.00 -1.00 -2.00
Model Number studies estimate Point Standard Variance Lower Upper Z-value P-value error limit limit squared Q-value df (Q) P-value I-squared Tau Standard error Variance Tau
B
Model Effect size and 95% confidence interval Test of null (2-tail) Heterogeneity T au-squared
Fixed 1 0.341 0.241 0.058 -0.131 0.813 1.415 0.157 0.000 0 1.000 0.000 0.000 0.000 0.000 0.000 Random 1 0.341 0.241 0.058 -0.131 0.813 1.415 0.157
Model Number Point Standard studies estimate error Variance Lower Upper limit limit Z-value P-value Q-value df (Q) P-value I-squared squared Tau Standard error Variance Tau
Study name
Avramidis et al. (2011) [9] 0.341 0.241 0.058 -00.31 0.813 1.415 0.157 0.341 0.241 0.058 -00.31 0.813 1.415 0.157
Statistics for each study Std diff
in means Standarderror VarianceLowerlimit Upperlimit Z-value p-value
2.00 1.00 0.00 -1.00 -2.00 TKA, 52 weeks
4. Han TR, Bang MS, Jeong SG. Rehabilitation medicine. 5th ed. Seoul: Koonja Publishing; 2008.
5. Stevens JE, Mizner RL, Snyder-Mackler L. Neuromuscular electrical stimulation for quadriceps muscle strengthening after bilateral total knee arthroplasty: a case series. J Orthop Sports Phys Ther 2004;34:21-29.
6. Paternostro-Sluga T, Fialka C, Alacamliogliu Y, Saradeth T, Fialka-Moser V. Neuromuscular electrical stimulation after anterior cruciate ligament surgery. Clin Orthop Relat Res 1999;(368):166-175.
7. Taradaj J, Halski T, Kucharzewski M, Walewicz K, Smykla A, Ozon M, Slupska L, Dymarek R, Ptaszkowski K, Rajfur J, Pasternok M. The effect of neuromuscular electrical sti-mulation on quadriceps strength and knee function in pro- fessional soccer players: return to sport after ACL reconstruc-tion. Biomed Res Int 2013;2013:802534.
8. Stevens-Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther 2012;92:210-226. 9. Avramidis K, Karachalios T, Popotonasios K, Sacorafas D,
Papathanasiades AA, Malizos KN. Does electric stimulation of the vastus medialis muscle influence rehabilitation after total knee replacement? Orthopedics 2011;34:175.
10. Boucher T, Wang S, Trudelle-Jackson E, Olson S. Effectiveness of surface electromyographic biofeedback-triggered neuro-muscular electrical stimulation on knee rehabilitation. N Am J Sports Phys Ther 2009;4:100-109.
11. Petterson SC, Mizner RL, Stevens JE, Raisis L, Bodenstab A, Newcomb W, Snyder-Mackler L. Improved function from progressive strengthening interventions after total knee arthroplasty: a randomized clinical trial with an imbedded prospective cohort. Arthritis Rheum 2009;61:174-183. 12. Avramidis K, Strike PW, Taylor PN, Swain ID. Effectiveness
of electric stimulation of the vastus medialis muscle in the rehabilitation of patients after total knee arthroplasty. Arch Phys Med Rehabil 2003;84:1850-1853.
13. Fitzgerald GK, Piva SR, Irrgang JJ. A modified neuromuscular
electrical stimulation protocol for quadriceps strength train-ing followtrain-ing anterior cruciate ligament reconstruction. J Ort-hop Sports Phys Ther 2003;33:492-501.
14. Ross M. The effect of neuromuscular electrical stimulation during closed kinetic chain exercise on lower extremity per-formance following anterior cruciate ligament reconstruction. Res Sports Med 2000;9:239-251.
15. Snyder-Mackler L, Delitto A, Bailey SL, Stralka SW. Strength of the quadriceps femoris muscle and functional recovery after reconstruction of the anterior cruciate ligament: a pro-spective, randomized clinical trial of electrical stimulation. J Bone Joint Surg Am 1995;77:1166-1173.
16. Snyder-Mackler L, Ladin Z, Schepsis AA, Young JC. Electrical stimulation of the thigh muscles after reconstruction of the anterior cruciate ligament: effects of electrically elicited contraction of the quadriceps femoris and hamstring muscles on gait and on strength of the thigh muscles. J Bone Joint Surg Am 1991;73:1025-1036.
17. Sisk TD, Stralka SW, Deering MB, Griffin JW. Effect of elec-trical stimulation on quadriceps strength after reconstructive surgery of the anterior cruciate ligament. Am J Sports Med 1987;15:215-220.
Peer Reviewers’ Commentary
본 논문은 무릎수술 후 대퇴사두근 위축을 예방하기 위한 신경근 전기자극치료의 효과 및 안전성을 검증하기 위해 체계적으로 기 술한 종설 논문이다. 문헌검색에 대한 체계적인 방법에 대해 잘 기술되었고, 결론에 도출할 때까지 과정도 잘 정리되었다. 차후 노인환자의 슬관절 전치환술에 대한 효과의 검증을 위한 추가적 인 후속연구가 나오기를 기대한다. [정리: 편집위원회]