Vol. 21, No. 1, April, 2013
□ Case report □Interferon β-1b Treatment in a Korean Girl with Multiple Sclerosis
Hyo Jeong Kim, M.D., Heung Dong Kim, M.D., Ph.D.
Joon Soo Lee, M.D., Ph.D. and Hoon-Chul Kang, M.D., Ph.D.
*Division of Pediatric Neurology, Department of Pediatrics, Severance Children’s Hospital Yonsei University College of Medicine, Seoul, Korea
= Abstract =
Here we report a case of pediatric multiple sclerosis treated with interferon β-1b. Interferon beta is widely used in adult patients with multiple sclerosis (MS). However, its effects and safety in pediatric patients have not been well established. Although supporting data are limited, the use of disease modifying therapies (DMTs) such as interferon β-1b is recommended early in treatment of children with MS. Reports of interferon beta treatment in pediatric MS patients in Korea are rare. In this report, we describe a Korean girl who was effectively treated with interferon β-1b for three years. There were no relapses or serious side effects. Therefore, this report provides evidence supporting the use of interferon beta in pediatric MS patients in Korea and other Asian countries. We also reviewed current medical treatment of MS, including some DMTs and second-line treatment options such as natalizumab and cyclophosphamide, and several new oral agents such as fingolimod.
Key Words : Multiple sclerosis, Interferon β-1b, Disease modifying therapies
1)
Introduction
About 3-10% of all patients with multiple sclerosis (MS) experience disease onset before the age of 18 years
1). Most patients present with a relapsing-remitting pattern and have risk for developing physical and cognitive disabilities
1)
. Disease modifying therapies (DMTs) such as
This work was supported by National Research Foundation grant funded by the Korea government (No. 2010-0020353).
Received : 21 December 2012, Revised : 12 March 2013 Accepted : 28 March 2013
Corresponding : Hoon-Chul Kang, M.D.,Ph.D.
Division of Pediatric Neurology,Department of Pediatrics, Pediatric Epilepsy Clinics, Severance Children’s Hospital, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea.
Tel: 02)2228-2075, Fax: 02)393-9118 E-mail: hipo0207@yuhs.ac
interferon beta and glatiramer acetate are shown to have positive effects in reducing relapses in adult MS patients.
However, the efficacy of DMTs in children with MS still remains to be proven because cli- nical trials cannot be performed due to the small numbers of patients with this disease in addition to ethical problems. However, the current con- sensus is that all pediatric patients with MS should be considered for treatment with either beta-interferon or glatiramer acetate as first- line therapy as early as possible to prevent re- lapse and disability
2, 3).
There are few studies on the use of DMTs
in pediatric MS patients. There is a cohort study
of 43 pediatric MS patients treated with inter-
feron beta-1b
4). Asian countries have a lower
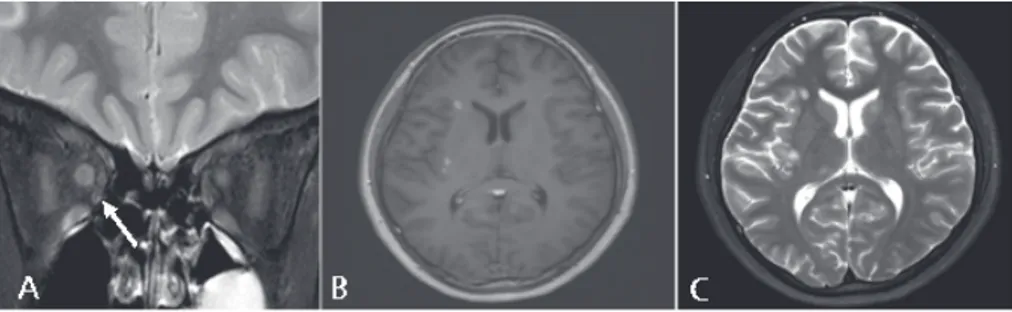
Fig. 1. The brain MRI shows slight enlargement and increased T2 signal in- tensity of the right optic nerve (A) while the gadolinium-enhanced T1 image (B) and T2 axial image (C) show multifocal plaques in the subcortex and deep white matter.
prevalence of MS than western countries, and reports about the use of DMTs in pediatric MS patients in Asia are rare. Here, we report a Korean patient with multiple sclerosis treated with interferon β-1b.
Case report
A 13-year-old girl presented with acute loss of visual acuity. The visual acuity in the right eye was 20/2000 and in the left eye it was 20/
60. Right optic disc swelling was also noted, and she was diagnosed with optic neuritis in the right eye. We performed brain magnetic resonance imaging (MRI), which showed slight enlargement and T2 signal hyperintensity of the right optic nerve (Fig 1A). Other brain lesions were not found. She was treated with high dose methyl prednisolone (1 g/day) intravenously for three days and was maintained on oral prednisolone thereafter (60 mg/day). Subsequently, her visual acuity completely recovered (20/60), and her condition improved with prednisolone tapered down to 10 mg/day.
However, two months after the first attack of visual loss in the right eye, she had a second attack of optic neuritis in both eyes. At that point, she had a loss of visual acuity in addition
to weaknesses of the left hand and both lower extremities. Her brain MRI showed increased signal in the both optic nerves and multifocal plaques in the subcortex and deep white matter (Fig 1B, C). Her spine MRI showed no abnor- malities.
She was diagnosed with multiple sclerosis based on the two clinical attacks and the pre- sence of multiple brain MRI lesions compatible with MS according to the 2010 revision to the McDonald criteria. The oligoclonal band profile was negative in the cerebrospinal fluid (CSF) and her IgG index was not checked. She was treated with steroid pulse (methyl prednisone 1 g/day) intravenously for three days followed by oral prednisolone (60 mg/day), tapered down slowly over the next six months. While on oral prednisone, she was also treated with interferon β-1b (Betaferon
Ⓡ) subcutaneously every other day. Her decreased visual acuity and weakness fully resolved, and she has been doing well for three years without any relapse. She sometimes complains of flu-like symptoms, which are well controlled with acetaminophen.
Discussion
According to a recent nationwide survey, the
prevalence of MS in Korea is 3.5-3.6 per 100,000
5), lower than the prevalence in western countries. The age specific prevalence is 0.53 from 5 to 9 years, 1.25 from 10 to 14 years and 2.14 from 15 to 19 years
5). The number of pe- diatric patients with multiple sclerosis in Korea is small, and reports of interferon beta treatment are limited. In one report, among ten patients treated with interferon β-1b, seven patients had no relapse, and three patients showed a reduc- tion in relapse rate with no severe adverse ef- fects
6). Those findings suggest interferon β-1b is an effective and safe treatment in Korean pediatric MS patients, similar to the results of a multicenter multinational review of interferon β-1b treatment in 43 children with MS
4).
Second-line treatment options for adults with active progressing relapsing-remitting MS that is unresponsive to interferon or glatiramer acetate are natalizumab, mitoxantrone and cyclophos- phamide. Among them, natalizumab treatment was demonstrated to be effective and well tole- rated in a cohort study of 17 pediatric MS pati- ents
7). Cyclophosphamide was also used in a group of 17 pediatric MS patients and was ef- fective, but showed some severe side effects such as bladder cancer, sterility, amenorrhea and osteoporosis
8). Further studies are required to assess the utility of these drugs as a second- line treatment option for pediatric patients with severe MS.
Several new oral treatments have shown be- nefit and have generated considerable interest because of the convenient mode of administration.
Five new oral drugs- fingolimod, cladribine, te- riflunomide, laquinimod, and dimethyl fumarate -have shown positive effects in phase III trials
9). Fingolimod, an immune modulator of sphingosine- 1-phosphate (S1P) receptors, was approved as
a first-line treatment for adult relapsing-remit- ting MS by the US Food and Drug Administration (FDA) in 2010. Safety and efficacy data for new oral treatments in adult MS patients will guide considerations for use in pediatric MS patients.
Accurate diagnosis is required in using inter- feron β-1b for treating MS. Neuromyelitis optica (NMO), an autoimmune inflammatory disorder characterized by optic neuritis and transverse myelitis, has clinical manifestations similar to MS. Because interferon β treatment is not ef- fective and even exacerbates the symptoms of NMO
10), careful assessment of clinical manife- stations, MRI features, and the presence of NMO IgG is required for accurate diagnosis. This pa- tient had recurrent optic neuritis, but the pos- sibility of NMO was ruled out because of the normal spinal MRI findings. The diagnosis of MS can be confirmed by clinical evidence alone according to the 2010 McDonald criteria. Our patient had two apparent attacks with objective clinical evidence in the optic nerve and brain cortex.
Optic neuritis in children is much less frequent
than in adults. In a study of childhood optic ne-
uritis
11), 13% of patients with isolated optic neu-
ritis had progressed to multiple sclerosis after
ten years of follow-up, while 19%, 22%, and
26% had progressed to MS after 20, 30 and 40
years, respectively. The presence of brain le-
sions on MRI except optic nerve as the initial
presentation of optic neuritis is known to be the
most important risk factor for MS
12). In addition,
the presence of unilateral
13)or bilateral sequential
or recurrent optic neuritis also increases the
risk of developing MS
11). Though our case had
no abnormal lesions on baseline brain MRI, optic
neuritis occurred unilaterally at first and recurred
bilaterally, which could be suggestive of an in-
creased risk of developing MS. Thus, pediatric patients with optic neuritis having such risk factors should be observed carefully.
Early treatment of pediatric MS is important to prevent physical disabilities and cognitive im- pairment. Pediatric patients with MS experience more frequent relapses than adults, and they acquire irreversible physical disabilities about ten years earlier than patients with adult onset disease
14). While physical disability is usually quantified using the Expanded Disability Status Scale (EDSS), cognitive impairment is often overlooked although it is notably more severe in patients with younger age of onset
15). Serial assessment of cognitive function is recommended to minimize the damage. Above all, DMTs such as interferon β-1b are expected to reduce re- lapse rate and have a positive effect in slowing disease progression in pediatric MS patients.
국 문 요 약
다발성 경화증 환아에서 Interferon β-1b의 효과적인 치료 증례
연세대학교 의과대학 소아과학교실
김효정ㆍ김흥동ㆍ이준수ㆍ강훈철
인터페론 베타는 성인 다발성 경화증 환자에서 질 병의 경과를 호전시키고 재발을 방지하는 효과가 있 어서 널리 사용되고 있다. 소아에서는 안정성 및 효 과가 잘 정립되어 있지는 않으나 최근 연구결과들에 따르면 소아의 다발성 경화증에서도 Interferon β- 1b와 같은 disease modifying therapies (DMTs) 를 초기에 사용하도록 권고하고 있다. 저자들은 다발 성 경화증으로 진단된 13세 여자 환자에서 3년간 In- terferon β-1b를 사용하여 부작용과 재발 없이 효 과적으로 치료 하였기에 이를 보고하는 바이다.
References
1) Banwell B, Ghezzi A, Bar-Or A, Mikaeloff Y, Tardieu M. Multiple sclerosis in children: clinical diagnosis, therapeutic strategies future directions.
Lancet Neurol 2007;6:887-902.
2) Chitnis T, Tenembaum S, Banwell B, Krupp L, Pohl D, Rostasy K, et al. Consensus statement:
evaluation of new and existing therapeutics for pediatric multiple sclerosis.Mult Scler 2012;18:
116-27.
3) Ghezzi A, Banwell B, Boyko A, Amato MP, Anlar B, Blink¬enberg M, et al. The management of multiple sclerosis in children: a European view.
Mult Scler 2010;16:1258-67.
4) Banwell B, RederAT, Krupp L, Tenembaum S, Eraksoy M, Alexey B, et al. Safety and tolera- bility of interferon beta-1b in pediatric multiple sclerosis. Neurology 2006;66:472-6.
5) Kim NH, Kim HJ, Cheong HK, Kim BJ, Lee KH, Kim EH, et al. Prevalence of multiple sclerosis in Korea. Neurology 2010;75:1432-8.
6) Lim BC, Hwang H, Kim KJ, Hwang YS, Cheon JE, Kim IO, et al. Relapsing demyelinating CNS disease in a Korean pediatric population: Multiple sclerosis versus neuromyelitis optica. Mult Scler 2011;17:67-73.
7) Ghezzi A, Pozzilli C, Brescia-Morra V, Bortolon F, Carpra R, Grimaldi L, et al. Safety and effec- tiveness of natalizumab in pediatric multiple sclerosis: results of 17 patients. MultScler 2009;
15(Suppl2):774.
8) Makhani N, Gorman MP, Branson HM, Stazzone L, Banwell B, Chitnis T. Cyclophosphamide the- rapy in pediatric multiple sclerosis. Neurology 2009;72:2076-82.
9) JoepKillestein, Richard A Rudick, Chris H Polman.
Oral treatment for multiple sclerosis. Lancet Neurol 2011;10:1026-34.
10) Kim SH, Kim W, Li XF, Jung IJ, Kim HJ. Does interferon beta treatment exacerbate neuromy- elitis optica spectrum disorder? Mult Scler 2012;
10:1480-3.
11) Lucchinetti CF, Kiers L, O’Duffy A, Gomez MR, Cross S, Leavitt JA, et al. Risk factors for de- veloping multiple sclerosis after childhood optic neuritis. Neurology 1997;49:1413-8.
12) Bonhomme GR, Waldman AT, Balcer LJ, Daniels AB, Tennekoon GI, Forman S, et al. Pediatric optic neuritis: brain MRI abnormalities and risk of multiple sclerosis. Neurology 2009;72:881-5.
13) Morales DS, Siatkowski RM, Howard CW, Wart- man R. Optic neuritis in children. J Pediatr Op- thalmol Strabismus 2000;37:254-9.
14) Renoux C, Vukusic S, Mikaeloff Y, Edan G, Clanet M, Dubois B, et al. Natural history of multiple sclerosis with childhood onset. New Engl J Med 2007;356:2603-13.
15) Amato MP, Goretti B, Ghezzi A, Lori S, Zipoli V, Portaccio E, et al. Cognitive and psychosocial features of childhood and juvenile MS. Neurology 2008;70:1891-7.