Case presentation
A 76-year-old man with a history of myocardial infarc- tion treated with transluminal coronary angioplasty, diabe- tes mellitus, atrial fibrillation, and heart failure on medica- tion was referred to our department for left sphenoid sinus lesion confirmed with brain magnetic resonance (MR) imaging, manifesting as dull-like headache and horizontal diplopia. The diplopia was worse with feeling of giddiness on looking straight ahead.
The abnormality on examination was limited to the left eye. Other neurological examination was normal. He complained about the progressive ptosis with swelling of the left upper eyelid. Visual acuity was 6/6 in both eyes.
There was no abnormality on colour vision test or Gold- man perimetry in either eye. The pupil size was isocoric and the left direct light reflex was sluggish but there was no relative pupillary defect. There was a pronounced limi- tation of medial gaze of left eyeball and his upper eyelid showed sluggish elevation or depression response to the physician’s order. It was concluded that left third nerve palsy were present. All movement of the right eye was normal.
On admission, brain MR imaging demonstrated low signal intensity in the left sphenoid sinus on axial T1 and T2-weighted settings. Axial post-contrast T1-weighted MR image at the level of the mid-orbit showed expan- sile tail-like shape lesion in the left sphenoid sinus which was connected to the superior orbit fissure and retrobulbar region (Fig. 1A). Paranasal sinus computed tomography (PNS-CT) showed left expansive sphenoid sinus filling with intermediate to high density materials without defi- nite bony erosion (Fig. 1B).
Actually, he had already been undergoing empirical an- tibiotics therapy for more than 3 days, though the symptom got aggravated that the patient could not elevate the left up- per eyelid even with effort. He complained the decreased vision of the left eye. Impaired ocular mobility, decreased J Rhinol 21(1), 2014
- 59 -
www.ksrhino.or.kr
A Case of Optic Neuropathy Secondary to Sphenoid Sinus Aspergillosis
Shin Chul Jung, MD, Hun Jae Oh, MD, Nam Yong Do, MD and Ji-Eun Lee, MD
Department of Otorhinolaryngology, Chosun University College of Medicine, Gwang-ju, Korea
aBstraCt
Orbital complication of an isolated sphenoid sinus lesion is rare. We recently experienced one case of optic neuropathy secondary to sphenoid sinus Aspergillosis. The patient presented with a headache and diplopia. Imag- ing and histology showed a sphenoid sinus lesion, andthe patientunderwent endoscopic sinus surgery. Because of the disease progression after the surgery,the patient was administered an anti-fungal agent underclinical suspicion ofan invasive fungal sinusitis infection before receiving histologic confirmation of tissue invasion by fungal hy- phae. The disease stabilized in three months by using approximately one month of anti-fungal agent. The type of treatment required for sphenoid sinus lesions depends on the extent of the disease upon initial examination as well ason the rapidity of diseaseprogression.
KeY WorDs : Sphenoid Sinus·Aspergillosis·Optic Neuropathy.
Address correspondence and reprint requests to Ji-Eun Lee, M.D, Department of Otorhinolaryngology, Chosun University College of Medicine, Chosun University Hospital, 365 Plimundaero, Dong-gu, Gwangju, 501-717, South Korea
Tel: +62-220-3206 · Fax: +62-225-2702 E-mail: [email protected]
Received for publication on October 17, 2013 Accepted for publicatoin on November 11, 2013
Fig. 1. (A)Preoperative magnetic resonance imaging shows ex- pansive lesion in left sphenoid sinus (T1, T2 and enhanced imag- es, from left). An iso- to hypointense signal density on T1-and T2 weighted images could be seen. Axial post-contrast T1-weight- ed MR image at the level of the mid-orbit showed expansile tail- like shape lesion in the left sphenoid sinus which was connected to the superior orbit fissure and retrobulbar region.
A
60 / J Rhinol 21(1), 2014
vision, ptosis, poor response to antibiotics, patient’s old age and several underlying medical conditions made urge physician to suspect strongly an invasive fungal sinusitis
infection. Thus, left side isolated sphenoidotomy was per- formed. Under general anesthesia, the natural ostium was opened via endoscopic transnasal approach while sparing the ethmoid cavity. Dissection proceeded medial to the middle turbinate, the ostium was widened medially and inferiorly with using the sphenoid punch forceps. In the sphenoethmoidal recess, yellowish, sticky and thick ma- terial drained through the small ostium (Figs. 2, 3). The natural ostium of sphenoid sinus was slightly expanded and the anterior wall of sphenoid sinus was supposed to be thin. Sphenoid sinus mucosa was edematous and hyper- emic without gross bony erosion (Fig. 4). The content and the mucosa of the sinus were taken for the biopsy.
Immediately after the operation, the headache relieved considerably, although ptosis and limitation of eye move- ment failed to show any improvement. On postoperative second day, severe headache reappeared after only a short remission. Poor response to antibiotic therapy and the pro- gression of the ocular complication shortly after the sphe- noidotomy operation made physician to strongly suspect the invasive fungal sinusitis. Thus, before the confirmation of presence of the fungal mucosa invasion by the biopsy, parenteral amphotericin B (maximum dose 50 mg daily) administration was started after consulting to the division of infectious disease 3 days after the operation.
However, this medication finally led to nausea, dyspnea, pitting edema, liver dysfunction, and congestive heart fail- B
Fig. 1. (B) Preoperative computed tomographic image shows soft tissue lesion with calcification in left sphenoid sinus.
Fig. 2. Yellowish discharge from left sphenoid natural ostium could be seen.
Fig. 4. Hyperemic mucosa of sphenoid sinus wall after removal of all necrotic debris was observed.
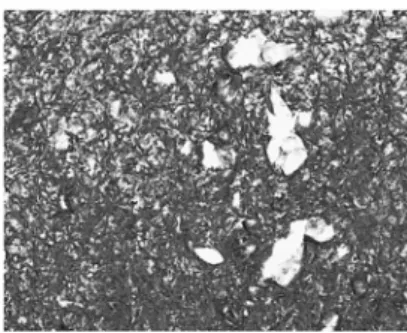
Fig. 5. Photomicrograph of sphenoid sinus specimen showed dichotomous, branching septate hypae (PAS; x400)
Fig. 6. Photomicrograph of sphenoid sinus specimen showed dichotomous, branching septate hypae (Silver stain; x400)
Fig. 3. Impacted necrotic fungal debris in the sphenoid sinus was removed during operation.
Jung et al : Sphenoid Fungal Sinusitis / 61
ure in a week. Meanwhile, histologic examination of the biopsy specimen showed chronic inflammatory changes consisted with numorous lymphocyte with dichotomous septate branching fungal hyphaes (Figs. 5, 6), compatible with Aspergillus without mucosa invasion.
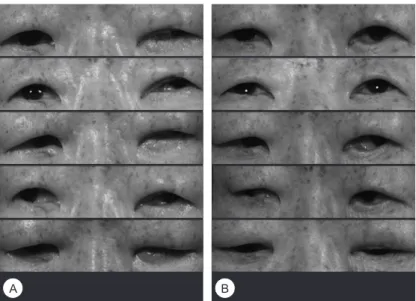
Oral voriconazole (400mg daily) was substituded for IV form 8 days after the previous treatment due to the side ef- fect mentioned above. A total of 28 days of voriconazole had administered, there has been a slow but consistent improvement in left eyeball movement (Fig. 7A). The pa- tient could open the upper eye lid much more comfortably at 2-month follow-up visit. Eventually, he could roll the eyeball almost full range of motion after 3 months post- operatively (Fig. 7B). The sphenoid sinus looked healthy and the large opening of it was maintained on endoscopic examination at last follow-up.
DisCussion
The fungal sinusitis is not a common disease, however, the prevalence has rising due to not only the increase of aging population, immunosuppressive patients and ad- ministration of systemic steroid but also the advanced diagnostic tool. Fungal sinusitis is subclassified into 4 dif- ferent types according to the time course or presence of invasion to the surrounding tissue; allergic, non-invasive, invasive or fulminant types, with non-invasive one being the most prevalent.
Isolated sinusitis in sphenoid lesion is rare and not usu- ally presented with symptoms related to sinuses involved such as nasal discharge, rhinorrhea, nasal stiffness and na- sal crusting, rather severe, persistent, and relentless head- ache and/or retrobulbar pain is more commonly accom- panied.1) Nowadays, there have been more reports with
fungal sinusitis having ocular complication such as diplo- pia, visual disturbance, ptosis, and/or ophthalmoplegia as the fist presenting symptoms.2) 3) Thus, it is important to suspect and diagnose the invasive type fungal sinusitis early, because once an orbital apex syndrome has devel- oped, it is ususally too late to save the patinet’s vision.
Orbital apex syndrome is composed of three elements: (i) visual loss due to optic neuropathy, (ii) opthalmoplegia due to third, fourth, and sixth cranial neuropathy; and (iii) ocular-orbital pain and/or anesthesia due to involvement of the opthalmic division of the fifth nerve.4) Orbital involve- ment worsens the prognosis because of ready availability of pathways for further intracranial spread. In patients with central nervous system involvement, the mortality is of 40% to 80%.5) 6)
The possible mechanism of ophthalmic complication by isolated sphenoid fungal sinusitis is supposed to be the di- rect effect of the acute inflammation of the sphenoid sinus mucosa going further into osteitis, which is more com- monly feasible when there is bony defect in the sinus wall.
In addition, compressive effect of the optic canal by the sphenoid mucocele or pyelocele and inflow of the inflam- matory byproducts after infection developed via veins or lymphatic ducts are known to be the possible offending causes. For the last reason, patients with eye or deep-lo- cated retrobulbar pain due to unsuspected invasive fungal sinusitis are occasionally treated with steroids for pre- sumed orbital inflammatory disease or giant cell arteritis, which contributes to the demise of the patients with fungal sinusitis, thus, earlier clinical suspicion is of importance.
Standard treatment is the surgical debriment of the of- fending sinus with/without intravenous amphotericin B.
The anti-fungal agents are usually administered to the patients who are proved to be infected with fungus as in-
Fig. 7. (A) postoperative 1 month, (B) postoperative 3 months. The patients had medial gaze limitation of the left eye, which had improved at postopera- tive 3 months.
A B
62 / J Rhinol 21(1), 2014
vasive form by histopathologic findings. Thus, multiple biopsies need to be taken from various sinuses, as fungal invasion is patchy and the biopsy need to be repeated if the initial biopsy is negative. Conventional amphotericin B is the drug of choice, however, its use is limited by dose- related nephrotoxicity and infusion-related acute toxicity.
Voriconazole is a second generation triazole with a broad spectrum of antifungal activity against Candida, Asper- gillus, Cryptococcus, and other species.7) Voriconazole is introduced as a suitable alternative to ampohtericin B preparations for empirical antifungal therapy in patients with neutropenia and persistent fever.8)
In our case, authors strongly suspected this patient’s fungal sinusitis as invasive form before the histopatho- logic confirmation on the grounds of 1) poor response to antibiotic therapy; 2) combined optic neuropathy; 3) progression of the ocular complication shortly after the sphenoidotomy operation; 4) re-aggravation of headache after short time period of alleviation of symptom post- operatively; 5) several underlying conditions- diabetes, coronary vessel disease and hypertension; 6) patient’s old age. Theses conditions made urge physician to suspect strongly an invasive fungal sinusitis infection and decide to prescribe the parenteral amphotericin B.
In clinic, it sometimes could be questioned whether the discontinuation of anti-fungal agent should be considered after the biopsy being proved there was no mucosal inva- sion. Since, the biopsy was taken from a small legional area, it could not represent and give information about the whole sphenoid mucosa and thus it might be the limita- tion of the pathological diagnosis. Though pathological distinction between invasive and non-invasive forms of aspergillus is important, early clinical susipicion and em- pirical prescription are also critical in such a case.
The present case of chronic fungal sinusitis was suc- cessfully treated with surgery and voriconazole adminis- tration. Systemic amphotericin B for 1 week seemed to be insufficient to reach to the therapeutic effect, on the other hand, voriconazole for 4 weeks gradually improved head- ache and impaired eyeball movement. The optimal dura- tion of antifungal drug administration for chronic invasive fungal sinusitis is controversial, reports varying from 3 months to more than 15 months.9-11) Our case had expe-
rienced mild dyspnea, too, when administering voricon- azole, so we could not continue the therapy more longer.
저자역할(Author Contributions)
정신철, 오훈재, 도남용, 이지은은 본 연구에서 모든 자료에 접근할 수 있으며 자료의 안전성과 자료 분석의 정확성에 책임을 지고 있습니다.
연구 기획 : 정신철, 이지은. 자료 해석 및 분석 : 오훈재, 도남용. 논문 초안 : 정신철. 논문수정 : 이지은, 도남용. 연구 총괄 : 이지은.
Acknowledgement
This study was supported by research fund from Chosun University, 2013
referenCes
1) Sivak-Callcott JA, Livesley N, Nugent RA, et al. Localized inva- sive sino-orbital aspergillosis: characteristic features. Br J oph- thalmol 2004;88:681-7.
2) Schuster MG, Stern J. Zygomycosis orbital apex syndrome in association with a solitary lung carcinoma. J Med Vet Mycol 1995;33:73-5.
3) Simmons BP, Johnson G, Aber RC. Fungus ball of the sphenoidal sinus in an immunocompetent host. South Med J 1982;75:762-5.
4) Neuro-opthalmology of invasive fungal sinusitis: 14 consecutive patients and a review of the literature. Clinical and experimental opthalmology 2013;41:567-76.
5) Shamim MS, Siddiqui AA, Enam SA, et al. Craniocerebral asper- gillosis in immunocompetent hosts. Surgical perspective. Neurol India 2007;55:274-81.
6) Hedges RT, Leung LS. Parasellar and orbital apex syndrome caused by aspergillosis. Neurology 1976;26:117-20.
7) Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med 2002;347:408–15.
8) Walsh TJ, Pappas P, Winston DJ, Lazarus HM, Petersen F, Raf- falli J, et al. Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever. N Engl J Med 2002;346:225–34.
9) Chirch L, Roche P, Fuhrer J. Successful treatment of invasive Aspergillus sinusitis with caspofungin and voriconazole. Ear Nose Throat J 2008;87:30–3.
10) Baumann A, Zimmerli S, Hausler R, Caversaccio M. Invasive sphenoidal aspergillosis: successful treatment with sphenoido- tomy and voriconazole. ORL J Otorhinolaryngol Relat Spec 2007;69:121–6.
11) Notheis G, Tarani L, Costantino F, Jansson A, Rosenecker J, Frie- derici D, et al. Posaconazole for treatment of refractory invasive fungal disease. Mycoses 2006;49(Suppl 1):37–41.