Arthrosc Orthop Sports Med 2014;1(1):50-53
50
INTRODUCTION
Clinical studies on the outcomes of various surgical techniques to repair longitudinal tears of the menisco- capsular junction have been well published [1,2]. And much is known about typical radiological features that mark longitudinal tears on meniscocapsular junctions.
However, all of these studies have focused on injuries of the posterior horn of meniscus. To the best of our knowledge, literature on longitudinal tears combined with horizontal tears on the anterior horn of the medial meniscus (AHMM) is sparse [3]. The anterior horn of the meniscus has been known to be a difficult area to examine by magnetic resonance imaging (MRI) or arthroscopy [4]. In addition, Choi and Victoroff [5] found that physical findings for anterior horn tears are different to those of other meniscal tears. In this article, we present a case of a longitudinal tear combined with a horizontal tear on the AHMM.
CASE REPORT
A 24-year-old man university student majoring in Tae-
kwondo was referred to our clinic. He presented with pain in the extended knee and crepitation during walking in the medial compartment of the left knee joint. His symptoms mainly occurred when he kicked with a stretched force using the symptomatic knee or stood with axis-rotational force whilst kicking with the contralateral leg. The pain started around 6 months prior to the hospital visit, and has continuously increased since then.
Clinical examination of the affected knee showed slight effusion, tenderness over the anteromedial joint-line, and a positive McMurray test result. No signs of ligamentous instability were observed. Anteroposterior and lateral simple radiographs showed no degenerative changes at the medial compartment. MRI revealed a complex tear from the anterior horn to the mid-horn. Peripheral images indicated that the AHMM was displaced far anteriorly (Fig. 1). A suspected AHMM tear was concluded based on clinical and MRI findings, and surgery to reattach or dissect the AHMM was advised.
After general anesthesia, the patient was placed in a supine position and the affected knee was positioned at 90o of flexion. A leg holder was used to support the We present a case report of a symptomatic longitudinal tear combined with a horizontal tear on the anterior horn of the medial meniscus in a 24-year-old man Taekwondo athlete. At initial examination, the patient complained of pain in the affected knee that had begun around six months ago when the knee was fully extended. Radiological analysis of the knee identified an extensive tear from the mid-horn of the medial meniscus to the anterior horn root, thus, leading to the anterior displacement of the meniscus. We successfully performed meniscal repair of the lesion using five outside-in stitches.
Keywords: Menisci, tibial; Anterior horn; Tear; Repair
http://dx.doi.org/10.14517/aosm13008 pISSN 2289-005X·eISSN 2289-0068
Case Report
A longitudinal tear combined with a horizontal tear on the anterior horn of the medial meniscus
Sang Min Kim
1, Seung Hoon Kang
1, Jong Gwan Kim
1, Byung Woo Ahn
1, Gye Young Han
21Department of Orthopaedic Surgery, Changwon Samsung Hospital, Sungkyunkwan University School of Medicine, Changwon;
2Department of Orthopaedic Surgery, Kangwon National University School of Medicine, Chuncheon, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
AOSM
Received August 1, 2013; Revised September 26, 2013; Accepted October 10, 2013
Correspondence to: Sang Min Kim, Department of Orthopaedic Surgery, Samsung Changwon Hospital, 158 Paryong-ro, Masanhoewon-gu, Changwon 630-723, Korea. Tel: +82-55-290-6030, Fax: +82-55-290-6030, E-mail: [email protected]
Sang Min Kim, et al. A longitudinal tear combined with a horizontal tear on the AHMM
www.e-aosm.org 51
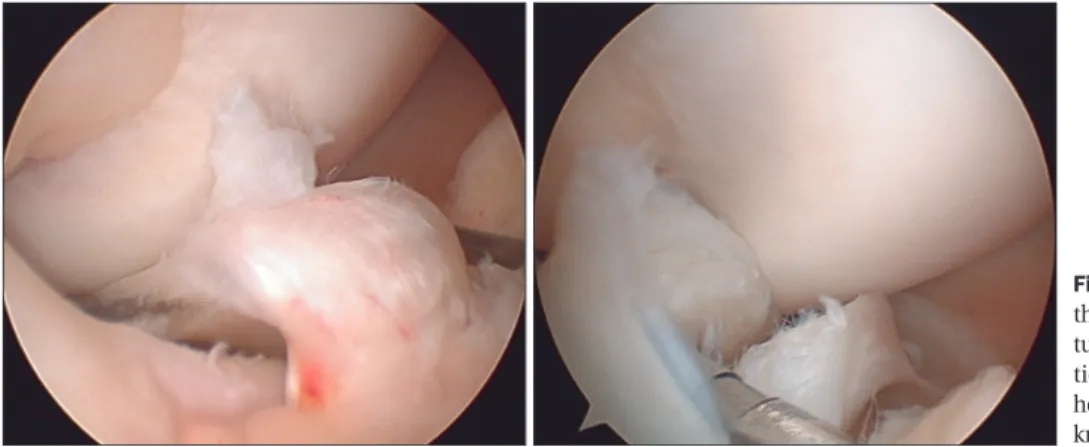
contralateral knee in abduction and flexion. Three standard portals (anterolateral, anteromedial, and supe- rolateral portals) were made. During diagnostic arthro- scopic examination, longitudinal meniscocapsular junctional tear on the medial meniscus, from the mid- horn to AHMM, was confirmed (Fig. 2). A horizontal tear was also observed from the mid-horn to AHMM (Fig. 3).The tear was located in zones B and C, according to Cooper et al. [6] (Fig. 4). The anterior horn root was intact.
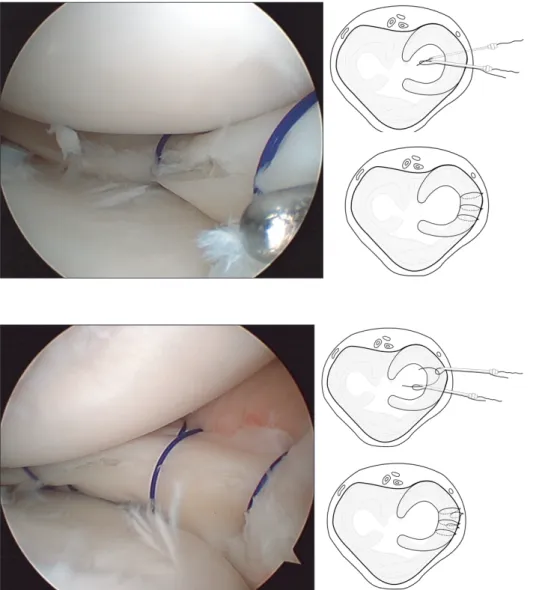
For arthroscopic meniscal repair, a spinal needle preloaded with No.0 PDS was penetrated into the space below the meniscus from the outside of the joint capsule. This suture material was pulled out through the anterolateral portal using a suture retriever and then, pulled above the meniscus to the outside of the joint capsule using a loop-formed spinal needle (Fig. 5).
Three stitches were made using this modified outside- in technique. Then, two-stitches were added using a
Fig. 2. Arthroscopic exploration through the anterolateral portal shows the longi- tu dinal tear at the meniscocapsular junc- tion from the mid-horn to the anterior horn of the medial meniscus on the right knee.
Fig. 1. Sagittal (left) and coronal (right) views of magnetic resonance imaging T2-weighted images of the right knee. An anterior horn of the medial meniscus with anterior displacement is shown having a complex tear.
Fig. 3. Arthroscopic view from anterolateral portal of the right knee shows the longitudinal tear of the medial meniscus that is combined with a horizontal tear.
Fig. 4. The tear is located across zones B and C according to the classification system established by Cooper et al. [6].
Sang Min Kim, et al. A longitudinal tear combined with a horizontal tear on the AHMM
www.e-aosm.org
52
modified suture technique for the vertical repair. The meniscus was pierced vertically using a suture hook and the No.0 PDS suture. After, both ends of the No.0 PDS suture on the femoral and tibial surfaces of the meniscus were pulled towards the outside of the joint capsule (Fig.
6). Finally, a skin incision was made adjacent to the suture materials and both ends were tied.
The preoperative symptoms were resolved and the Lysholm score increased from 40 to 85 points postsurgery.
The patient returned to his former activity 6 months postoperatively.
DISCUSSION
Meniscus tear is a common knee injury in young active individuals. According to a 10-year study on the epide- miology of sports injuries, Majewski et al. [7] reported
that meniscus injury is the second most prevalent injury involving around 24% of all internal knee injuries.
Most injuries are localized to the posterior horn of the meniscus, whereas an anterior horn tear, especially of the medial meniscus, is rare [8]. Terzidis et al. [9] reported that among 314 cases of athletic knee injuries, only 2.5% were located in the anterior horn.
The present report on a young Taekwondo player who exhibited a symptomatic knee in the extended position subsequently showed a longitudinal tear combined with a horizontal tear of the AHMM when examined arthroscopically. And given that tears in anterior horns are uncommon our case was even more unusual in that an isolated meniscal injury without a combined ligament rupture was seen.
At initial consultation, the patient complained of pain at the anteromedial aspect of the knee joint during knee Fig. 5. A spinal needle preloaded with PDS No.0 was penetrated into the space beneath the meniscus from the outside of the joint capsule. This suture material was pulled out through the anterolateral portal using a suture retriever and then, pulled above the meniscus to the outside of the joint capsule using a loop-formed spinal needle.
Fig. 6. For the vertical repair, the meniscus was pierced vertically using a suture hook and a No.0 PDS suture. Both ends of the No.0 PDS on the femoral and tibial surfaces of the meniscus were pulled to the outside of the joint capsule.
Sang Min Kim, et al. A longitudinal tear combined with a horizontal tear on the AHMM
www.e-aosm.org 53
extension. A characteristic symptom of an anterior horn tear is pain during knee extension, especially experienced during motions such as ball kicking, and pain during weight-bearing extension. Eren [10] investigated joint- line tenderness by physical examination as an indicator for meniscal tear and found that its reliability as a diagnostic indicator is useful (96%), sensitive (89%), and specific (97%). On the other hand, the merit of MRI is still controversial in terms of diagnosing an anterior horn tear. Shankman et al. [4] emphasized potential pitfalls of MRI when diagnosing tears in the anterior horn of the meniscus, reporting a 74% false-positive rate.
Ahn et al. [11] introduced a vertical repair technique to stabilize a torn anterior horn. Vertical repairs can hold more circumferential collagenous fibers of the meniscus and has more strength than the horizontal repair [1].
However, there may be a risk of meniscal injury when piercing the meniscus due to the increased mobility of the torn meniscus in the vertical suture technique. Therefore,
using the modified outside-in technique without piercing the meniscus may be useful in some cases. In this present case, the modified outside-in technique was considered to be the more reasonable choice of technique as both longitudinal and horizontal tears required minimal handling of the meniscus.
In conclusion, meniscal injury can occur in the anterior horn of medial meniscus with a longitudinal tear combined with a horizontal tear. A preoperative diagnosis of the anterior horn tear was possible based on MRI findings together with physical findings. The modified outside-in technique was the choice of treatment to repair the torn meniscus.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Ahn JH, Bae TS, Kang KS, Kang SY, Lee SH. Longitudinal tear of the medial meniscus posterior horn in the anterior cruciate ligament-deficient knee significantly influences anterior stability.
Am J Sports Med 2011;39:2187-93.
2. Ahn JH, Kim SH, Yoo JC, Wang JH. All-inside suture technique using two posteromedial portals in a medial meniscus posterior horn tear. Arthroscopy 2004;20:101-8.
3. Feucht MJ, Minzlaff P, Saier T, Lenich A, Imhoff AB, Hinterwimmer S. Avulsion of the anterior medial meniscus root: case report and surgical technique. Knee Surg Sports Traumatol Arthrosc 2013 Mar 1 [Epub]. http://dx.doi.org/10.1007/s00167-013-2462-7.
4. Shankman S, Beltran J, Melamed E, Rosenberg ZS. Anterior horn of the lateral meniscus: another potential pitfall in MR imaging of the knee. Radiology 1997;204:181-4.
5. Choi NH, Victoroff BN. Anterior horn tears of the lateral meniscus in soccer players. Arthroscopy 2006;22:484-8.
6. Cooper DE, Arnoczky SP, Warren RF. Arthroscopic meniscal repair. Clin Sports Med 1990;9:589-607.
7. Majewski M, Susanne H, Klaus S. Epidemiology of athletic knee injuries: A 10-year study. Knee 2006;13:184-8.
8. Shepard MF, Hunter DM, Davies MR, Shapiro MS, Seeger LL. The clinical significance of anterior horn meniscal tears diagnosed on magnetic resonance images. Am J Sports Med 2002;30:189- 92.
9. Terzidis IP, Christodoulou A, Ploumis A, Givissis P, Natsis K, Koimtzis M. Meniscal tear characteristics in young athletes with a stable knee: arthroscopic evaluation. Am J Sports Med 2006;
34:1170-5.
10. Eren OT. The accuracy of joint line tenderness by physical examination in the diagnosis of meniscal tears. Arthroscopy 2003;19:850-4.
11. Ahn JH, Wang JH, Yoo JC, Kim SK, Park JH, Park JW. The modified outside-in suture: vertical repair of the anterior horn of the meniscus after decompression of a large meniscal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:1288-91.