INTRODUCTION
Medial meniscus posterior root (MMPR) tears are fre- quently encountered in individuals more than 50 years of age with degenerative arthritis of the knee and have recently been receiving enormous attention in the clinical setting [1,2]. In the absence of accurate demographic data,
studies have reported MMPR tears are more prevalent in Asian countries with a culture of sitting on the floor and suggested obesity and old age are the major risk factors [3,4].
The tibial attachment site of the medial meniscus posterior horn is considered critical for maintaining normal meniscal function by distributing circumferential hoop tension and preventing meniscal extrusion [5]. The Background: The purpose of the present study was to investigate clinical and radiological outcomes of pullout suture repair of medial meniscus posterior root (MMPR) tear using a knotless anchor and a modified Mason-Allen stitch in terms of physical assessment, functional score and radiological Kellgren-Lawrence grade.
Methods: Eighteen consecutive patients were treated using an arthroscopic meniscal root repair technique. The average follow-up period was 15 ± 6.5 months (range, 13 to 32 months). There were 7 men and 11 women, and their mean age was 52.2 years (range, 43 to 60 years). Under the vision of the posterior trans-septal portal, the modified Mason-Allen stitch was applied to MMPR repair and the limbs of the two separate sutures were secured outside of the joint using knotless anchor. For postoperative clinical evaluation, joint line tenderness test, McMurray test, Lysholm knee scoring scale, Oxford knee score and visual analogue scale (VAS) were used. Radiological evaluation was performed using magnetic resonance imaging (MRI) and the Kellgren-Lawrence grading system.
Results: The tenderness over the medial joint line and positive McMurray test demonstrated in all patients preoperatively were observed in 9 patients (50%) and 5 patients (28%) postoperatively (P = 0.023, P < 0.001, respectively). The average postoperative Lysholm score, Oxford score, VAS score were significantly increased compared to the preoperative values (P
< 0.001). Postoperative Kellgren-Lawrence grades showed no significant difference from the preoperative values. Among eight patients in which postoperative MRI was performed, six patients exhibited complete healing and continuity at the previous tear site. Meanwhile, incomplete healing and some continuity within the posterior meniscal root lesion were found in two patients.
Conclusion: Our study demonstrated that pullout repair of MMPR tears using a knotless anchor and a modified Mason- Allen stitch provides a wide field of vision for optimal tibial tunneling without the risk of iatrogenic cartilage damage, facilitates firm and effective fixation, and produces satisfying clinical outcomes.
Keywords: Medial meniscus; Posterior root; Tear; Pullout suture repair; Mason-Allen stitch
One-year clinical outcomes of pullout suture repair of
medial meniscus posterior root tear using a knotless anchor and a modified Mason-Allen stitch
Young-Jin Seo
1, Yon-Sik Yoo
1, Si Young Song
1, In Sung Kim
1, Chan Hyeok Kim
1, Yoon Sang Kim
2, Seong-Wook Jang
21Department of Orthopaedic Surgery, Hallym University Dongtan Sacred Heart Hospital, Hwaseong; 2HiLab, Korea University of Technology and Education, Cheonan, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
AOSM
Received July 25, 2013; Revised August 20, 2013; Accepted September 7, 2013
Correspondence to: Yon-Sik Yoo, Department of Orthopaedic Surgery, Hallym University Dongtan Sacred Heart Hospital, 7 Keunjaebong-gil, Hwasung 445-907, Korea. Tel: +82-31-8086-2410, Fax: +82-31-8086-2429, E-mail: [email protected]
consequences of an MMPR tear could be as undesirable as total meniscectomy in terms of the loss of function of the circumferential fibers and weakening of the ability of the meniscus to withstand hoop stress in the medial compartment of the knee, which could lead to early onset of medial femorotibial arthritis [1,2,6].
The conventional meniscectomy for MMPR tears causes degeneration of the affected compartment and loss of hoop stress of the medial meniscus [4]. In contrast, a biomechanical study demonstrated that the peak contact pressure could be restored to normal after MMPR repair [7]. Thereafter, repair of MMPR tears has garnered growing interest and a variety of arthroscopic repair techniques have been proposed.
The currently available MMPR repair techniques include transosseous pull out suture techniques and suture anchor repair techniques [1,2,6,8-12]. Most of these techniques have been performed arthroscopically without the necessity of a posterior knee incision. However, such techniques are not conducive to visualization of the narrow posteromedial joint space, secure fixation of the torn meniscus, and correct tunnel positioning [1,2,6,8,10,12,13].
In addition, traditional arthroscopic techniques carry the risk of iatrogenic cartilage damage on the tibia and femur and meniscal injuries, and effective fixation in the final operational stage remains technically challenging.
Of the alternative techniques designed to overcome such limitations, we used a modified Mason-Allen stitch technique for the repair of MMPR tears through the trans- septal portal. The suture technique allows for firm traction of the posterior root, suture retrieval through the transtibial tunnel out of the anteromedial tibial cortex, and knotless anchor (Footprint PK, Smith & Nephew Endoscopy, Mansfield, MA, USA) fixation.
The purpose of the present study was to investigate clinical and radiological outcomes of pullout suture repair of MMPR tears using a modified Mason-Allen stitch and knotless anchor fixation with respect to the physical examination, knee function scores, and Kellgren-Lawrence
(K-L) grade. Our hypothesis was that there would be a significant improvement in the clinical outcome, whereas no notable difference would be observed in the K-L grade after surgery.
METHODS
Demographic data
Of the patients who underwent arthroscopic MMPR repair performed by the same surgeon between February 2007 and October 2010, 18 patients who were available for
≥ 1-year follow-up were enrolled in this study.
The inclusion criteria were as follows: (1) magnetic resonance imaging (MRI) evidence of an MMPR tear;
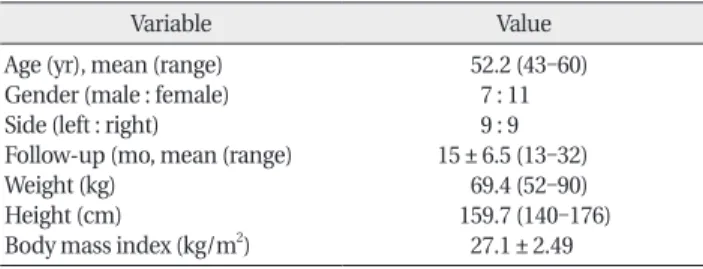
(2) the presence of persistent subjective pain along the medial joint line, catching, or giving-way symptoms in spite of ≥ 2 months of conservative treatment; and (3) K-L grade 1 or 2 degeneration. Patients were excluded if the age was ≥ 60 years, the contact surface between the posterior horn and the tibia accounted for more than half of the footprint diameter, the body mass index was >30, rheumatoid arthritis was present in the ipsilateral knee, there was an infection or a history of previous surgery. Of the 18 patients, 7 were male and 11 were female with a mean age at the time of surgery of 52.2 years (range, 43 to 60 years). The surgery was performed on the right side in 9 patients. The mean follow-up period was 15 ± 6.5 months (range, 13 to 32 months) (Table 1). The mean interval from symptom onset to surgery was 8.7 months. Thirteen patients had a history of minor trauma with symptoms, 16 patients felt acute pain when crouching, and 12 patients experienced popping when walking (Table 2).
Operative technique
Surgery was performed in the supine position with the thigh fixed in a leg holder. If an MMPR tear was confirmed with diagnostic arthroscopy through anteromedial and anterolateral portals, a posteromedial portal and then a posterolateral portal were created (Fig. 1). An arthro- scope introduced through the anterolateral portal was
Table 1. Demographic data
Variable Value
Age (yr), mean (range) Gender (male : female) Side (left : right)
Follow-up (mo, mean (range) Weight (kg)
Height (cm)
Body mass index (kg/m2)
52.2 (43-60) 7 : 11 9 : 9 15 ± 6.5 (13-32)
69.4 (52-90) 159.7 (140-176)
27.1 ± 2.49
Table 2. Preoperative conditions
Variable No. (%)
Duration of symptoms before surgery (mo), mean (range)
Injury mode with trauma Preoperative pain when squatting Preoperative pain when running
8.72 (2-24) 13 (72) 16 (89) 12 (83)
advanced between the medial wall of the femoral inter- condylar notch and the posterior cruciate ligament to the posteromedial compartment. Subsequently, after visuali zation of the posteromedial compartment, a posteromedial portal was established at an appropriate location using a spinal needle. The septum was pierced with a switching stick that was inserted through the posteromedial portal. The switching stick was advanced further until its tip could be palpated through the skin around the posteolateral aspect of the knee. After making a stab incision in the skin over the prominent area, a sleeve was introduced along the switching stick that was removed prior to the insertion of an arthrscope through the sleeve. The posteromedial compartment was visualized via the arthroscope advanced through the posterolateral portal. If the posteromedial compartment was not approachable due to severe varus alignment, inercondylar notch narrowing, or adjacent tissue fibrosis, the arthroscope was inserted through the anteromedial portal and passed between the anterior cruciate ligament (ACL) and the lateral wall of the femoral intercondylar
notch and a posterolateral portal was established under direct visualization of the posterolateral compartment.
While inspecting the torn meniscal root and the insertion site with the arthroscope advanced from the posterolateral portal through the posterior septum, debri- dement of the torn end of the posterior horn of the medial meniscus was performed. Then, the bone bed around the insertion site was exposed using a high speed burr that was introduced through the posteromedial portal.
The Tightrope (Arthrex, Naples, FL, USA) guide set at 90o was inserted through the posteromedial portal and its tip was placed at the center of the tibial footprint of the medial meniscus posterior horn. A 3-cm longitudinal incision was made at the center between the tibial tuberosity and the posteromedial tibial cortex. After exposing the anteromedial tibial cortex, a 3.5-mm-diameter guide pin was drilled through the tunnel guide located anteromedial to the proximal tibia to the center of the footprint of the medial meniscus posterior horn. The Tighitrope system was removed and a bone tunnel of 4.5-mm-diameter was overdrilled using an Endobutton (Smith & Nephew Fig. 1. Posterior root tear of the medial meniscus in the left knee. (A) View from the anterolateral portal. (B) View from the posterior trans-septal portal via the posterolateral portal. A posterolateral capsular injury was identified.
Fig. 2. (A) Tightrope guide was inserted through the posteromedial portal. (B) A 3.5-mm-diameter guide pin was advanced into the center of the footprint of the medical meniscus posterior horn.
Endoscopy) drill for suture retrieval through the transtibial tunnel out of the anteromedial aspect of the proximal tibia (Fig. 2).
For the modified Mason-Allen stitch, a suture was passed from the posterior surface to the anterior surface of the torn end of the medial meniscus using a suture hook inserted through the postromedial portal (Fig. 3A, C).
During the procedure, the end of the suture hook was placed approximately 2-3 mm medial to the torn end of the meniscus and the hook was withdrawn when the suture was sufficiently advanced into the intramedullary cavity. Both ends of the No-1 polydiaxone monofilament
absorbable suture (PDS; Ethicon, Cornelia, GA, USA) were pulled through the bone tunnel out of the anteromedial portion of the tibia using a retriever. The second suture was advanced from 5 mm medial to the first stitch to penetrate the torn end of the meniscus and pulled through the transtibial tunnel out of the anteromedial portion of the proximal tibia in the same manner. Thus, the modified Mason-Allen suture wherein two stitches form a cross shape was completed (Fig. 3B, D). Each suture was replaced with Fiberwire sutures and both limbs were pulled through the bone tunnel toward the anteromedial tibia. While maintaining the suture tension,
Fig. 4. After repair of the meniscal root, secure fixation was obtained with ade- quate tension between the meniscal torn end and the bone bed. (A) View from the posterior septal portal. (B) View from the anterolateral portal.
Fig. 3. (A, B) View from the posterior trans-septal portal: the meniscal root and capsule were pierced by a suture hook that was introduced via the post- eromedial portal. (A) First horizontal suture (B) second vertical suture. (C, D) Pictures of the porcine tibia meniscus to demonstrate the modified Mason-Allen suture. (C) First horizontal suture and (D) second vertical suture. Arrows: direction of the suture passage.
the adequacy of the tension in the posterior horn was assessed using an arthroscopic probe (Fig. 4A, B).
The suture limbs were connected to a 5.5-mm knotless anchor (Footprint PK) and inserted 1 cm distal to the entry of the tibial bone tunnel with the knee in 90o flexion (Fig. 5). Postoperatively, a splint was applied with the leg in full extension. Weight-bearing during walking was not permitted for 4 weeks. Thereafter, range of motion (ROM) was gradually increased up to 90o with the knee protected in a hinged brace for 2 weeks. From the 6th postoperative week, partial weight-bearing was allowed as tolerated for 2 weeks. Full weight-bearing was initiated from the 8th postoperative week and ≥ 90o of ROM was initiated from the 3rd postoperative month [1].
Clinical and radiological evaluation
Clinical evaluation was performed using the joint line tenderness test, McMurray test, Lysholm knee score and Oxford knee score for subjective evaluation of the knee, and visual analogue scale (VAS) for measuring pain level preoperatively and at the last follow-up.
For radiological evaluation, standing anteroposterior
radiographs taken with the knee in 45o flexion and MRI scans were obtained preoperatively and at the last follow-up. Joint degeneration of the affected knee was assessed using the K-L grading system [14]. Healing of the MMPR tear was assessed by comparing MRI scans obtained preoperatively and at a mean of 13.2 months postoperatively. Complete healing was defined as the absence of high signal intensity in the posterior horn of the meniscus on postoperative MRI and appearance of the normal meniscal configuration in the coronal and axial planes [1] A meniscus was considered partially healed if the postoperative MRI shows diffuse areas of high signal intensity. The MRI scans were reviewed by a musculoskeletal radiologist who was unaware of the patients’ clinical information.
Statistical analysis
Statistical analyses were performed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). The preoperative and postoperative clinical data were compared using a paired t-test with a significance level set at P < 0.05.
Fig. 5. (A) Fiberwire suture limbs were connected to a Knotless anchor (Footprint PK). (B-D) Pictures of the porcine tibia to demonstrate the knotless anchor fixation: the knotless anchor was inserted at 1 cm inferior to the tibial tunnel and (B) and adequate tension could be obtained during insertion of the knotless anchor (C and D).
RESULTS
Clinical results
Tenderness over the medial joint line that had been present in all knees preoperatively was noted in 9 patients (50%) postoperatively, and McMurray’s test was positive in 5 patients (28%) postoperatively, indicating statistically significant improvement (P = 0.023 and P < 0.001, res- pectively). The Lysholm score and Oxford score were in- creased remarkably to 78.6 and 34.9, respectively (P < 0.001 for both). A statistically significant improvement was observed in the VAS score (P < 0.001). These results are described in Table 3.
Radiological results
There was no notable change in the K-L grade between the preoperative (grade 1 in 11 knees and grade 2 in 7 knees) and postoperative (grade 1 in 8 knees and grade 2 in 10 knees) assessments, suggesting no significant progression of joint degeneration (Table 3). MRI was performed at the last follow-up on 8 knees, 6 of which exhibited continuity at the previous tear site without the presence of diffuse areas or high signal intensity and normal meniscal configuration in the axial and coronal planes. In the remaining 2 knees, partial high signal intensity was seen in spite of the presence of continuity, albeit incomplete.
DISCUSSION
The distinctive features of the surgical technique for the repair of MMPR tears in this study include the use of the
posterior trans-septal portal instead of the conventional anteromedial and anterolateral portals for enhanced visualization of the MMPR, a modified Mason-Allen suture for more durable suture, and a knotless anchor (Footprint PK) for fixation of the sutures advanced to the anteromedial aspect of the tibia.
In the past, partial meniscectomy was considered to provide clinical improvement in knees with MMPR.
However, the risk of the procedure for early onset arthritis [2,3,7,15-18] has been suggested by a multitude of studies focusing on the importance of the maintenance of hoop stress. Thus, the significance of MMPR repair is twofold: prevention of early arthritis and restoration of the biomechanics of the knee joint [6-8,19-21].
The conventional arthroscopic MMPR repair techniques using an anterolateral portal do not allow for adequate visualization of the posterior compartment through the notch between the femur and the tibia in knees with intercondylar notch narrowing, tibial spine enlargement, adjacent soft tissue degeneration [6]. Moreover, separate lesions between the posterior root and the adjacent posterior joint capsule are difficult to inspect through an anterolateral portal and an incomplete suture repair could result in an interruption of blood flow from the posterior joint capsule [18]. Although anterior approaches with use of a medial collateral ligament release were introduced by some authors [18,22], the potential risk of the release of the intact ligament has not yet been determined. In order to overcome these limitations, we used a posterior trans-septal portal in this study suggested by Ahn and Ha [23]. This portal provides arthroscopic visualization of the structures in the posterior compartment of the knee, such as the areas adjacent to the posterior horn, meniscal roots, posterior septum, and posterior joint capsule, without the risk of damage to the neurovascular structures. In our study, the posterior trans-septal portal established through the posterolateral portal allowed complete visualization of the posteromedial compartment, and the posteromedial portal was used as a working portal without the risk of cartilage damage and medial collateral ligament injuries [24-27].
The fundamental principles of MMPR repair are similar to those of rotator cuff repair in terms of fixating the torn end of the meniscus to a bone bed, and a number of MMPR repair techniques based on simple stitching have been proposed [27]. However, simple stitching carries the risk of a retear or suture failure caused by weak tensile force. In contrast, the biomechanical and clinical Table 3. Clinical outcomes
Variable Preoperative Postoperative P-value McMurray test
Joint line tenderness Visual analogue scale Lysholm score Oxford knee score Kellgren-Lawrence grade 1
2 3 4
Healing status of MRI Complete Incomplete Retear
18 18 7.6 ± 1.3 67.3 ± 10.6 19.2 ± 7.2
11 7 0 0 - - -
5 9 2.9 ± 1.8 78.6 ± 7.2 34.9 ± 5.9
8 10
0 0 6 2 0
<0.001 0.023
<0.001
<0.001
<0.001 -
-
MRI, magnetic resonance imaging.
superi ority of the Mason-Allen technique has been well recognized: crossing of a vertical suture and a horizontal suture provides greater ultimate strength and stiffness than do other repair techniques [24-28].
Gerber et al. [24] proposed a modified Mason-Allen technique for rotator cuff repair and Scheibel and Habermeyer [28] suggested that a modified Mason-Allen technique would result in greater contact pressure on the bone bed in rotator cuff repair using a suture anchor. In a study by Lee et al. [27], the Mason-Allen stitch was applied to MMPR repair where the limbs of the two separate sutures passed through the torn end of the meniscus were knotted outside of the joint and a horizontal loop was made using the shuttle relay method. Then, a vertical loop was created to complete the cruciate-shaped stitch.
In our study, a suture was advanced forward from behind the torn meniscal end to form a horizontal loop and a vertical loop was created medial to the horizontal loop to finish the cruciate-shaped stitch using a couple of simple sutures as in the Mason-Allen technique. We believe this modified Mason-Allen technique is time efficient and relatively easy to perform, and thus highly reproducible.
Various techniques for fixation of the torn end of the meniscus to a bone bed and their benefits and drawbacks are well documented in the literature [1,2,6,8-12].
An arthroscopic suture anchor fixation suggested by Engelsohn et al. [29] is advantageous in that the procedure can be performed without a tibial tunnel [1,2,6,9,20];
however, it requires considerable skill for suture anchor positioning and fixation, and an improper positioning would lead to a non-anatomical repair or fixation failure [4].
Still, pullout repair techniques have been preferred by many authors and satisfying clinical outcomes have been reported [1,4,5,7,12,18,30]. In particular, transosseous pullout repair techniques have been demonstrated in various studies [4,5,8,13,18,19,30-32]. In a study by Kim et al. [19], a suture was pulled out through a 5-mm- diameter tunnel using a wire loop. Ahn et al. [8] created a tibial tunnel using a 2.9-mm cannulated drill bit to allow for the use of a 4.0-mm cannulated screw and used a wire loop for suture pullout. In another study, Ahn et al. [13] introduced a double transosseous pullout suture technique that requires two tibial tunnels made with an ACL tibial guide pin. Marzo and Kumar [31] used a suture grasper for suture pullout through a 7-mm-diameter tibial tunnel. A tibial tunnel of small diameter is beneficial for reducing iatrogenic injuries and increasing the contact area between the meniscus and the tibia. Unfortunately,
it takes tremendous skill to pull out a suture through a narrow tunnel or necessitates extended surgical time or additional surgical equipment. In this study, the tibial tunnel was created using a 4.5-mm-diameter Endobutton drill and a suture retriever was used to withdraw the suture through the tunnel with ease and safety.
In our study, the clinical results of pullout repair were comparable to those of other series [1,4,5,7,12,18,30]. Joint line tenderness and the number of positive McMurray test decreased significantly after surgery. Furthermore, notable improvement was observed in the postoperative VAS score, Lysholm score, and Oxford knee score. On the radiological evaluation, there was no significant pre- and postoperative change in the K-L grade, and complete healing was observed in 75% of the patients with follow- up MRI.
In a 2-year follow-up study, Lee et al. [5] noted significant improvement in the Lysholm score and complete healing without cartilage damage at second-look arthroscopy.
Kim et al. [1] reported functional improvement in terms of the Lysholm score and presence of MRI evidence of complete healing in 50% of the cases at 2 years after surgery. In a study by Kim et al. [18], there were significant increases in the postoperative Lysholm score and International Knee Documentation Committee (IKDC) score, evidence of healing was observed in 68% of the 47% of the total patients who were available for a second- look arthroscopy, and complete healing, partial healing, and repeat tears were observed with MRI in 56.7%, 36.7%, and 6.7%, respectively, at the last follow-up. Moon et al.
[7] observed notable improvement in the postoperative VAS score and Lysholm score and excellent healing in 90.3% of the patients on postoperative MRI scans. On the other hand, Seo et al. [11] reported that complete healing was not achieved in any of the cases after pullout repair at second-look arthroscopy; however, they could not determine a relationship between complete healing and clinical improvement.
Suture fixation in the anteromedial tibia can be per- formed with various methods using a sliding knot, a screw, a washer, tying over a bone bridge, a button, or an EndoButton [4,5,8,13,18,19,30-32]. In the present study, we used a knotless anchor that is commonly used in rotator cuff repair in an attempt to achieve maximum early strength during insertion. Maintenance of meniscal tension is vital for a successful MMPR repair because a loose suture results in the inability of the meniscus to withstand hoop stress. The knotless anchor was useful
for obtaining easy and effective fixation as opposed to the other methods that exhibit the risk of decreasing tension and strength during knotting of sutures. An additional benefit of the knotless anchor fixation is that implant- related irritation can be avoided due to the insertion into the tibial cortex. The drawback is that abrasion or rupture of the suture may result from the contact with the sharp nail thread and the bone.
The limitations of the study include the relatively small study population and short follow-up period. In addition, the radiological evaluation of meniscus healing was restricted by the limited availability of patients for follow- up MRI. Furthermore, in the absence of biomechanical criteria, it was difficult to evaluate the superiority of the
fixation using a knotless anchor and a modified Mason- Allen suture technique over other fixation methods, which we believe should be addressed in further research.
Our study demonstrated that pullout repair of MMPR tears using a knotless anchor and a modified Mason- Allen stitch provides excellent visualization for safe tibial tunneling without the risk of iatrogenic cartilage damage, facilitates firm and effective fixation, and produces satisfying clinical outcomes.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Kim JH, Chung JH, Lee DH, Lee YS, Kim JR, Ryu KJ. Arthroscopic suture anchor repair versus pullout suture repair in posterior root tear of the medial meniscus: a prospective comparison study.
Arthroscopy 2011;27:1644-53.
2. Jung YH, Choi NH, Oh JS, Victoroff BN. All-inside repair for a root tear of the medial meniscus using a suture anchor. Am J Sports Med 2012;40:1406-11.
3. Ozkoc G, Circi E, Gonc U, Irgit K, Pourbagher A, Tandogan RN.
Radial tears in the root of the posterior horn of the medial meni- scus. Knee Surg Sports Traumatol Arthrosc 2008;16:849-54.
4. Jones C, Reddy S, Ma CB. Repair of the posterior root of the medial meniscus. Knee 2010;17:77-80.
5. Lee JH, Lim YJ, Kim KB, Kim KH, Song JH. Arthroscopic pullout suture repair of posterior root tear of the medial meniscus:
radiographic and clinical results with a 2-year follow-up. Arthro- scopy 2009;25:951-8.
6. Kim JH, Shin DE, Dan JM, Nam KS, Ahn TK, Lee DH. Arthroscopic suture anchor repair of posterior root attachment injury in medial meniscus: technical note. Arch Orthop Trauma Surg 2009;
129:1085-8.
7. Moon HK, Koh YG, Kim YC, Park YS, Jo SB, Kwon SK. Prognostic factors of arthroscopic pull-out repair for a posterior root tear of the medial meniscus. Am J Sports Med 2012;40:1138-43.
8. Ahn JH, Wang JH, Yoo JC, Noh HK, Park JH. A pull out suture for transection of the posterior horn of the medial meniscus: using a posterior trans-septal portal. Knee Surg Sports Traumatol Arthrosc 2007;15:1510-3.
9. Koenig JH, Ranawat AS, Umans HR, Difelice GS. Meniscal root tears: diagnosis and treatment. Arthroscopy 2009;25:1025-32.
10. Nicholas SJ, Golant A, Schachter AK, Lee SJ. A new surgical technique for arthroscopic repair of the meniscus root tear. Knee Surg Sports Traumatol Arthrosc 2009;17:1433-6.
11. Seo HS, Lee SC, Jung KA. Second-look arthroscopic findings after repairs of posterior root tears of the medial meniscus. Am J Sports Med 2011;39:99-107.
12. Cho JH. Modified pull-out suture in posterior root tear of the medial meniscus: using a posteromedial portal. Knee Surg Relat Res 2012;24:124-7.
13. Ahn JH, Wang JH, Lim HC, et al. Double transosseous pull out suture technique for transection of posterior horn of medial meniscus. Arch Orthop Trauma Surg 2009;129:387-92.
14. Kellgren JH, Lawrence JS. Radiological assessment of osteo- arthrosis. Ann Rheum Dis 1957;16:494-502.
15. Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus: similar to total meniscectomy. J Bone Joint Surg Am 2008;90:1922-31.
16. Seo JH, Li G, Shetty GM, et al. Effect of repair of radial tears at the root of the posterior horn of the medial meniscus with the pullout suture technique: a biomechanical study using porcine knees. Arthroscopy 2009;25:1281-7.
17. Han SB, Shetty GM, Lee DH, et al. Unfavorable results of partial meniscectomy for complete posterior medial meniscus root tear with early osteoarthritis: a 5- to 8-year follow-up study.
Arthroscopy 2010;26:1326-32.
18. Kim SB, Ha JK, Lee SW, et al. Medial meniscus root tear refixation: comparison of clinical, radiologic, and arthroscopic findings with medial meniscectomy. Arthroscopy 2011;27:346- 54.
19. Kim YM, Rhee KJ, Lee JK, Hwang DS, Yang JY, Kim SJ. Arthro- scopic pullout repair of a complete radial tear of the tibial attach- ment site of the medial meniscus posterior horn. Arthroscopy 2006;22:795.e1-4.
20. Choi NH, Son KM, Victoroff BN. Arthroscopic all-inside repair for a tear of posterior root of the medial meniscus: a technical note.
Knee Surg Sports Traumatol Arthrosc 2008;16:891-3.
21. Park YS, Moon HK, Koh YG, et al. Arthroscopic pullout repair of posterior root tear of the medial meniscus: the anterior approach using medial collateral ligament pie-crusting release. Knee Surg Sports Traumatol Arthrosc 2011;19:1334-6.
REFERENCES
22. Kim YJ, Kim JG, Chang SH, Shim JC, Kim SB, Lee MY. Posterior root tear of the medial meniscus in multiple knee ligament injuries. Knee 2010;17:324-8.
23. Ahn JH, Ha CW. Posterior trans-septal portal for arthroscopic surgery of the knee joint. Arthroscopy 2000;16:774-9.
24. Gerber C, Schneeberger AG, Beck M, Schlegel U. Mechanical strength of repairs of the rotator cuff. J Bone Joint Surg Br 1994;
76:371-80.
25. Ma CB, MacGillivray JD, Clabeaux J, Lee S, Otis JC. Biomechanical evaluation of arthroscopic rotator cuff stitches. J Bone Joint Surg Am 2004;86:1211-6.
26. Castagna A, Conti M, Markopoulos N, et al. Arthroscopic repair of rotator cuff tear with a modified Mason-Allen stitch: mid-term clinical and ultrasound outcomes. Knee Surg Sports Traumatol Arthrosc 2008;16:497-503.
27. Lee DW, Jang SH, Ha JK, Kim JG, Ahn JH. Meniscus root refixation technique using a modified Mason-Allen stitch. Knee Surg Sports
Traumatol Arthrosc 2013;21:654-7.
28. Scheibel MT, Habermeyer P. A modified Mason-Allen technique for rotator cuff repair using suture anchors. Arthroscopy 2003;
19:330-3.
29. Engelsohn E, Umans H, Difelice GS. Marginal fractures of the medial tibial plateau: possible association with medial meniscal root tear. Skeletal Radiol 2007;36:73-6.
30. Griffith CJ, LaPrade RF, Fritts HM, Morgan PM. Posterior root avulsion fracture of the medial meniscus in an adolescent female patient with surgical reattachment. Am J Sports Med 2008;36:789-92.
31. Marzo JM, Kumar BA. Primary repair of medial meniscal avulsions: 2 case studies. Am J Sports Med 2007;35:1380-3.
32. Harner CD, Mauro CS, Lesniak BP, Romanowski JR. Bio- mechanical consequences of a tear of the posterior root of the medial meniscus: surgical technique. J Bone Joint Surg Am 2009;91 Suppl 2:257-70.