A medial meniscus posterior root tear (MMPRT) with extrusion results in the loss in transmission of circumferential hoop stress, leading to significantly increased peak contact pressure at the tibiofemoral joint and to accelerated articular cartilage degeneration. For these reasons, the need to diagnose and treat MMPRTs early has been highlighted in recent years. With remarkable developments in imaging technology and in arthroscopy, MMPRTs are being diagnosed earlier and earlier. Recently, various repair techniques other than meniscectomy have evolved, aimed at restoring viability and the biomechanical properties of the torn meniscus. While much of the current studies on meniscal repair have demon- strated a high rate of healing and improvements in terms of subjective and functional parameters, there is no consensus concerning the optimal technique to manage MMPRTs. This article aims to present a review of the literature and sum- marize the clinically relevant anatomical, biomechanical, and functional roles of the medial meniscus, as well as the current trends regarding surgical techniques of MMPRTs. However, because the debate over surgical technique and the effectiveness of root repair for joint preservation remains controversial, further studies are still needed.
Keywords: Menisci, tibial; Posterior root tears; Meniscectomy; Meniscal repair
Current concepts in medial meniscus posterior root tears:
diagnosis, treatment, and outcomes
Dong-Hyun Lee, Young-Joo Shin, Eun-Kyoo Song, Jong-Keun Seon
Center for Joint Disease, Chonnam National University Hwasun Hospital, Hwasun, Korea
Copyright © 2017 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received November 26, 2016; Revised December 5, 2016; Accepted December 9, 2016
Correspondence to: Jong-Keun Seon, Center for Joint Disease, Chonnam National University Hwasun Hospital, 322 Seoyang-ro, Hwasun-eup, Hwasun 58128, Korea. Tel: +82-61-379-7678, Fax: +82-61-379-7681, E-mail: [email protected]
Arthroscopy and Orthopedic Sports Medicine
AOSM
INTRODUCTION
The medial meniscus, a crescent-shaped fibrous cartilage structure, is known to be essential for congruity of con- tact surfaces, stability, shock absorption, and propriocep- tion of the knee joint [1]. The medial meniscus comprises a cross-network of collagen fibers, proteoglycans, and glycoproteins and converts axial load into hoop stress during knee flexion and extension. A posterior root tear of the medial meniscus or medial meniscus posterior root tear (MMPRT) disrupts the biomechanics and the kine- matics of the knee joint, thereby accelerating its degen- eration. Biomechanical studies have reported that there are no significant differences in peak contact stresses between knees that underwent total meniscectomy and those that had a ruptured meniscal posterior root [2].
In 1991, Pagnani et al. [3] first described meniscal root tears as radial tears found within a 10-mm–proximity
of the posterior insertion of the meniscal root; research concerning these tears in the following 25 years has demonstrated the importance of meniscal root integrity.
Meniscal attachment, especially at the medial meniscus, is susceptible to injury and can cause meniscal extrusion, which leads to decreased surface area of contact and to a burdened cartilage [4]. The injury also leads to impaired loop stress and accelerates articular degeneration [5].
The posterior root of the meniscus, which has a thick lig- amentous attachment, is known to be vulnerable to dam- age. Such damage in elderly patients has been shown to be often induced by trauma or degenerative changes and to occur relatively commonly and repetitively. Although the clinical diagnosis of MMPRTs is known to be difficult, the sensitivity and specificity of the diagnosis are improv- ing with developments in magnetic resonance imaging (MRI) and arthroscopy. Lately, the efficacy of several techniques developed to repair MMPRTs have also been
proven [6,7]. The purpose of this review article is to report the current concepts of MMPRTs, from anatomy to treat- ment, focusing especially on controversial issues such as the question as to whether the main functions of the meniscus is restorable by repair and the gold standard of repair for meniscal injuries.
ANATOMY
The medial meniscus posterior root connects the pos- terior horn of the meniscus to bone so that the load transmitted from the femur to the tibia makes the cir- cumferential collagen fibers of the meniscus stretch, al- lowing impacts to be absorbed. The distribution of hoop stress by the circumferential fibers helps to transmit rela- tively axial loads across articular contact surface, which prevents the build-up of excessive pressure and destruc- tion of articular cartilage [8]. Unlike the medial meniscus anterior root which contains a simple flat insert inside the tibial plateau, the medial meniscus posterior root contains a relatively complex three-dimensional insert [9]. Hence, a clear understanding the medial meniscus posterior root anatomy is important for the diagnosis and treatment of MMPRTs [10]. The posterior root inserts just anteromedial to the posterior cruciate ligament (PCL) and at the posterior aspect of the medial tibial intercon- dylar eminence [11]. Johannsen et al. [9] quantitatively located the boundary of the medial meniscus posterior root as a region roughly 9.6-mm posterior and 0.7-mm exterior to the peak of medial tibial ridge; 3.5-mm exte- rior to the inflection point of the medial tibial plateau cartilage; and 8.2-mm anterior from the peak of the tibial attachment of the PCL. The mean total surface area of the posterior medial meniscus root greatly varies within the current literature, ranging from 47 to 80 mm2 [8]. This variability in measurement seems to be, as suggested by Ziegler et al. [12], because of ‘shiny white fibers’, which are found on the rear side and incompletely separated from the medial meniscus posterior root; it has been suggested that these white fibers maintain an appearance of conti- nuity with the bony attachment site of the posterior root, leading to the discrepancies in measurements. The pres- ence of such fibers have also been described as a possible cause of the posterior expansion of the medial meniscus posterior root, yet the clear function of this structure re- mains elusive [12].
EPIDEMIOLOGY
MMPRTs are relatively common lesions; it has been shown that between 10% and 21% of meniscal surgeries present with MMPRTs [13]. Because of more restricted mobility and significantly greater load, the posterior root of the medial meniscus is more prone to lesions than the posterior lateral root [14,15]. These tears are more com- mon in Eastern countries, such as Korea, where a floor- based lifestyle is habitual and traditional. The long-term repetitive hyper-flexion of the knee under weight-bearing required for such floor-based lifestyle is thought to be closely linked to the prevalence of MMPRTs. Chronic and repetitive hyper-flexion of the knee under weight-bearing in the older population, especially, may cause excessive pressure on the meniscus posterior root and its subse- quent impingement and degeneration [13]. Yet in another study, frequent performing of the Buddha position or kneeling could not be identified as major risk factors for MMPRTs. Previous studies that investigated risk factors of MMPRTs have stated that older age, a female gender, increased body mass index, and decreased sport activity are associated with a higher prevalence of MMPRTs [16].
The majority of patients with MMPRTs were found to not have undergone any major traumatic events [17];
however, in a different study it was shown that MMPRTs could result from acute traumatic events or multi-liga- mentous injuries, which are associated with trauma [18].
More frequently MMPRTs are chronic injuries associated with meniscal extrusion, with reduced shock absorp- tion, with joint degeneration, and ultimately with osteo- arthritis. MMPRTs increase peak contact pressure and cause similar biomechanical consequences as seen with total meniscectomy [2,19]. Furthermore, a higher risk of spontaneous osteonecrosis of the knee (SPONK) has been reported in association with MMPRTs more than it has been with simple radial tears of the meniscus [20].
SPONK has been shown to be associated with MMPRTs in 80% of cases and with medial meniscal tears in 67%
[21].
BIOMECHANICS
MMPRTs are essential for preserving hoop stress within the meniscus and preventing meniscal protrusion [17].
Allaire et al. [2] insisted that MMPRTs increase peak con- tact stress of the medial compartment by 25% relative to normal conditions. And Marzo and Gurske-DePerio [22]
reported similar results, showing that MMPRTs decreases the contact surface area by 20% and increases the peak contact stress by 32% across the medial compartment. In addition, MMPRTs have been shown to increase external rotation and lateral dislocation of the tibia, and these changes have been shown to cause varus deformity of the lower limbs [2].
DIAGNOSIS
Clinical examination
Clinical diagnosis of MMPRTs is generally known to be difficult. Patients generally complain of pain in the me- dial joint surface, swelling, and loss of knee flexion; and the McMurray test, which is typically positive for me- niscus injuries, may also be positive without evidence of mechanical locking [7]. Recently, Seil et al. [23] dem- onstrated a novel clinical test for medial meniscus root avulsions: during the varus stress test, which is one of the test components of the novel clinical test, the tester can palpate the medial meniscal extrusion with the knee in full extension. Of note, without the application of stress, the meniscus protrusion cannot be palpated.
A painful popping sensation, which often presents as a single event especially among Asians passed middle age, is known as a strong predictor of MMPRTs. Bae et al.
[24] reported that 83 of 86 patients (96.5%) with painful popping sensations were diagnosed as having an isolated MMPRT. And the presence of this clinical sign in MMPRT may also indicate that the patient’s articular cartilage is less degenerative status. When patients are first exposed to trivial injury, they may feel a popping sensation in the knee joint and then severe pain may develop later, which makes normal walking difficult. Although pain may re- solve and normal activity may resume, intermittent re- sidual pain and popping sounds can remain and signs of early degenerative diseases may be seen [24].
Radiographic imaging
For the diagnosis of MMPRTs, plain radiographic exami- nation of the knee under loading condition is recom- mended. Clinical symptoms such as early joint space narrowing, swift progression of arthritis, and varus de- formity of the knee are often caused by meniscal extru- sion [25]. Particularly, measuring the joint space via the Rosenberg view (45o flexion standing anteroposterior view) before and after the surgery is critical for diagnosis.
Standing lower extremity scanography is also recom-
mended [26]. Moon et al. [27] reported that 35.3% of knees with MMPRTs had a varus alignment of over 5o. And Hwang et al. [16] reported that varus alignment was one of the risk factors for MMPRTs and that the mean mechanical axis angle was 4.5o in patients with MMPRTs.
Magnetic resonance imaging
Because there lacks an effective physical examination to diagnose MMPRTs, MRI has been used to diagnose MMPRTs. However, it has been shown that among 67 di- agnoses of MMPRTs made by arthroscopy only 72.9% of them could be reaffirmed by preoperative MRI. Thus, ac- curately diagnosing MMPRTs through MRI may heavily depend on the quality of images and on how skilled the radiologist is [28].
Diagnostic accuracy of MRI for meniscal root avul- sions is not compromised by the presence of combined ACL tears [29]. However, the questions as to which MRI technique is most reliable and which image cut is most appropriate to detect meniscal root tears remain contro- versial. Recently, fat-suppressed volume isotropic turbo spin echo acquisition (FS 3D VISTA) with Reader Defined Axial reconstruction has been described as a powerful method to detect radial tears and MMPRTs [30]. Further, the presence of subchondral marrow edema, deep within the MMPRT, was described as a possible indicator of MMPRTs. It has been shown that the edema usually re- solves if they are associated with meniscal root tears [31].
Coronal plane imaging
In general, MMPRT lesions are most easily observed on consecutive coronal MRI images, which present the lesions as fibrous-cartilaginous bands attached to the medial tibia, such observations indicate a truncation of the posterior root. For their high specificity and sensi- tivity, T2-weighted images are generally viewed as the best forms of the MRI image [32]. Yet in cases where it is difficult to diagnose a tear, such as when the MMPRT is relatively small, a meniscal extrusion of the medial me- niscus is strongly suggestive of MMPRTs. The extrusion of the medial meniscus can be defined as the partial or complete dislocation of the cartilaginous plate in relation to the tibial plateau (Fig. 1). This is usually the result of a considerable disruption of the circumferential fibers of the meniscus and a loss in the ability to resist hoop strain.
Meniscal extrusion has also been described in associa- tion with cartilage degeneration within the medial com- partment [33]; it has also been demonstrated that this
association is seen when the extrusion or displacement of the meniscus is greater than 3 mm [34]. Conversely, be- cause some authors argued that this 3-mm threshold had a high specificity (98%) but a low sensitivity (54%), they introduced the meniscal L/T (length/transverse) ratio as an adjunct index to diagnose MMPRTs [35].
Axial plane imaging
An important sign of MMPRTs is the radial linear defect of the posterior root of the cartilage plate, which can be found in axial plane imaging (Fig. 2). For some authors,
the axial image has been preferred over coronal and sagittal images when diagnosing MMPRTs because the perpendicular direction of the transverse ruptures with respect to the directional axis of the meniscus allows easier identification of the tear.
Sagittal plane imaging
The pathognomonic sign of an MMPRT is a ghost sign.
The ghost sign occurs when the posterior meniscus can- not be discerned at all in the sagittal plane and when the signal intensity of the meniscus, which is normally low, is converted to a high intensity signal. It also indicates a disconnected interval between the posterior root and the PCL (Fig. 3). In addition, in patients with MMPRTs, sagit- tal imaging at the medial side of the PCL shows that the tibial insert of the medial meniscus is attached to the an- terolateral midpoint of the posterior intercondylar fossa of the tibial plateau and that the PCL is attached to the posterolateral midpoint of the intercondylar fossa, 1- to 1.5-cm inferior to the joint line.
CHOICE OF TREATMENT
The current treatment options for MMPRTs can be di- vided into either conservative or surgical treatment;
the latter includes meniscectomy and meniscal repairs.
Important decision-making factors when choosing the mode of treatment for MMPRTs are (1) surgical candidacy of patients; (2) age; (3) type of injury (acute or chronic); (4) Fig. 1. The coronal T2-weighted image shows medial meniscal extru-
sion (arrow).
Fig. 2. The axial scan shows an area of high-signal intensity within the posterior horn, indicating a radial root tear (arrow).
Fig. 3. The sagittal magnetic resonance image shows a ghost sign at the medial meniscus posterior root tear, recognizable by loss in shape and signal intensity (arrow).
symptoms; and (5) the condition of the articular cartilage.
Although conservative treatment fails to prevent bio- mechanical and degenerative changes in patients with meniscal root tears, it may still be indicated for patients deemed as poor surgical candidates. However, surgi- cal treatment remains the best treatment option for MMPRTs especially in young patients, in patients with a healthy cartilage, and in those with acute injuries. Given that various factors influence the outcome of surgical treatment, a thorough evaluation of the indications that would recommend a patient for surgical treatment is re- quired to obtain satisfactory treatment outcomes.
Conservative treatment
The indications for conservative treatment of MMPRTs include a low demand lifestyle; an inoperable knee with severe medical problems, advanced arthritis (above an Outerbridge grade of 3 [19]); joint-space narrowing; varus malalignment (> 5o); and chronic, degenerative, and ir- reparable tears [27,36].
Typically, conservative treatment is used restrictively to treat MMPRTs if indications for surgical treatment are inadequate. Although conservative treatment may fail to restore the normal biomechanics of the knee and wors- ened degeneration of joints [37], it is still a useful initial mode of treatment in certain situations. For instance, conservative treatment can be attempted with satisfac- tory clinical outcomes in elderly patients, in candidates poorly suited for surgery, and in patients with preexisting arthritis. Conservative management may also be em- ployed to alleviate acute pain before surgical procedures.
Neogi et al. [38] evaluated 33 patients who underwent su- pervised exercise therapy for 12 weeks after being treated for MMPRTs and found that symptomatic and functional outcomes were improved at a mean follow-up of 35 months.
Modes of conservative treatments include non-steroi- dal anti-inflammatory drugs (NSAIDs), active muscle strengthening exercises around the knee joint, and life style modifications that promotes low demand activity.
The appropriate utilization of these approaches would provide not only acute symptomatic relief but also long- term favorable clinical results. For example, in patients with advanced arthritis, a multimodal approach such as a combination of oral medication (NSAIDs) and intra- articular injections to treatment may reduce the need for further surgical intervention.
Surgical treatment
Surgical options fall into 2 broad categories—menis- cectomy and meniscal repair—both of which can be performed arthroscopically as to avoid unnecessary dis- section of the posterior aspect of the knee. The general indications for surgical treatment has been high activ- ity, a healthy condition without pre-existing arthritic changes, a normal mechanical alignment, and mild to no joint-space narrowing. The list of indications for surgical treatment is constantly expanding, especially for surgical repairs. Meniscectomy is considered as the better option for chronic root tears since the meniscus is known to have a poor healing capacity and poor tissue quality. On the other hand, meniscal repair is the treatment of choice for acute traumatic root tears without pre-existing ar- thritis and for chronic symptomatic root tears in relative young patients who do not generally have osteoarthritis.
If patients indicated for surgical treatment present with excessive varus malalignment (> 5o), high tibial osteot- omy (isolated or concomitant repair) may be attempted for a better outcome. The main approaches for meniscal repair include the transtibial pullout repair and the suture anchor repair. The goals of an MMRPT repair surgery are to obtain relief of symptoms and to prevent the progres-
Table 1. Indications for Meniscal repairs in patients with MMPRTs
Consideration Details
Age < 65 yr
Time of injury Acutea)
Condition of joint Mild to no joint space narrowing
a. Outerbridge classification below grade 3 b. Kellgren-Lawrence grade I or II
Activity level Patients with relatively high-demand activity (laborers, sports activities [running, climbing, etc.]) Compliance Tolerance of partial weight bearing for at least 6 weeks
MMPRT, medial meniscus posterior root tear.
a)The definitions of “acute” and “chronic” for MMPRTs are yet to be determined.
sion of arthritis. The details of the common indications for meniscal repair is provided in Table 1 [6,7,25,27,39–42].
Contraindications of a meniscal repair are excessive varus malalignment (> 5o) and cartilage degeneration on radiologic evaluation (Outerbridge classification 3 or 4;
Kellgren-Lawrence grade III or IV).
Meniscectomy
Meniscectomy, both partial and total meniscectomy, can be performed for posterior root tears. Treatment benefits are usually relief of acute pain and of mechanical symp- toms, such as locking of the knee during flexion, although the long-term benefits and outcomes of the intervention are yet to be studied. Compared to repairs, partial men- iscectomy has advantages of a relatively short operation time and a short hospitalization period, allowing patients to begin weight bearing early, perform a less restricted postoperative rehabilitation protocol, and return to daily activities faster [34]. When meniscectomy is carried out in case of partial root avulsion, only the free flap of the meniscal root should be removed and the remnant tis- sue on the tibial attachment site should be preserved.
However, partial meniscecotomy has not been shown to restore the native anatomy and the biomechanical prop- erties of the meniscus and is associated with increased pressure on the remnant meniscus and with exacerbated cartilage degeneration. Also, partial tears may progress to complete tears during debridement of the foot print, and it can lead to functional deficits of the knee joint.
Therefore, care should be taken to avoid such complica- tions when performing meniscectomies. The limitations
of meniscectomy has led to a shift in preference from menisecetomy to repairs over the recent years [2,9]. Nev- ertheless, partial meniscectomy can be a more effective treatment option than meniscal repair in certain situa- tions, such as in patients with chronic root tears and pre- existing arthritic chondral lesions.
Transtibial (transosseous) pullout repair
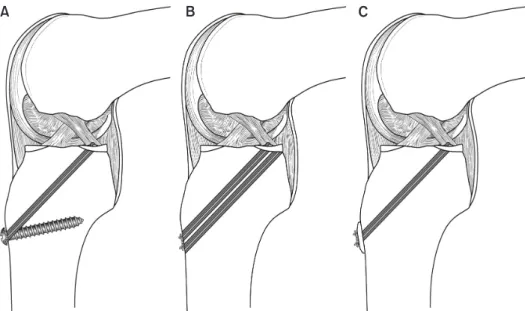
The transtibial pullout repair has been used for the fixa- tion of meniscal roots through the bone tunnel on the tibia. Indications for a transtibial pullout repair include a meniscal root tear that extends from the tibial insertion and no prior placement of a tibial bone tunnel through multiligamentous reconstruction. Arthroscopically, an ACL tibial drill guide is used to make 1 or 2 small bone tunnels at the anterior aspect of the proximal tibia. If visualization is inadequate under arthroscopy, an acces- sory posteromedial portal can be placed [43,44]. After confirming anatomical positioning, a suture passer is used to place No. 2 non-absorbable sutures through the substance of the avulsed meniscal root. The type of passer, curved or another such device, may be chosen at the discretion of the surgeon. Once passed, the sutures limbs are then shuttled through the tibial bone tunnel, tightened distally, and fixed using an appropriate fixa- tion device. Fixation devices typically used are screws [45], bone bridges [43,44], or pull-out buttons [46] (Fig. 4). For posterior horn medial meniscus root repairs, Kim et al.
[45] described an arthroscopic technique using a trans- tibial bone tunnel that is drilled using an ACL guide. They used 2 non absorbable sutures that were tensioned and
Fig. 4. Fixation technique for the trans- tibial pullout repair: Suture repair is tied over a screw (A), a button (B), and the bone bridge (C).
A B C
fixed over a screw and a washer on the anteromedial as- pect of the proximal tibia. Whereas, Ahn et al. [43] were the first to describe a double transosseous pullout suture repair using an accessory posterior transseptal portal to obtain secure fixation and a well-visualized root. This technique drills a tibial bone tunnel, using an ACL guide through the posteromedial portal, and ties two suture limbs sutures over a bony bridge that is found between the two tunnels on the anteromedial surface of the tibia.
In another example, Raustol et al. [44] passed the 2 eyelet pins through an accessory posteromedial portal placed at a steep angle. The 2 pins were used to create a mattress suture through the medial root and tied over the bone bridge at the anterolateral tibia. Lastly, Padalecki et al. [46]
reported a novel in situ pullout repair technique for ra- dial tears. The sutures were passed in an anteroposterior configuration and tied over a button at the anteromedial aspect of the proximal tibia.
Suture anchor repair
The transtibial pullout suture technique for root repair has its inherent disadvantages [1]: (1) the drilling of the bone tunnel interferes with concomitant ligament recon- struction; (2) the abrasion of the suture with the distal fixation may cause fixation loss; and (3) the surgery is challenging when concomitant corrective osteotomy is performed. While transosseous fixation is unsuitable under certain conditions, the suture anchor technique has theoretical advantages. Engelsohn et al. [47] first de- scribed an arthroscopic suture anchor technique using an accessory posteromedial portal, which is used to fa- cilitate anchor insertion and passage of sutures through
the avulsed root. Under arthroscopic visualization, a double-load suture anchor is inserted at the anatomical root attachment site and the sutures are passed through the accessory posteromedial portal, through which the sutures are tied using a knot pusher and knotted (dur- ing the tying and knotting the tension is placed directly on the meniscal root). Furthermore, the knots should be kept posteriorly because prominent suture knots may lead to complications such as anchor loosening and cartilage wear [34]. Often, the accessory portal is created more proximally to accomplish a more vertical inser- tion of the anchor and to avoid posterior convexity of the medial femoral condyle [26,48]. However, the optimal location and orientation of suture anchors are yet to be determined.
Stitch configuration for meniscal root repair
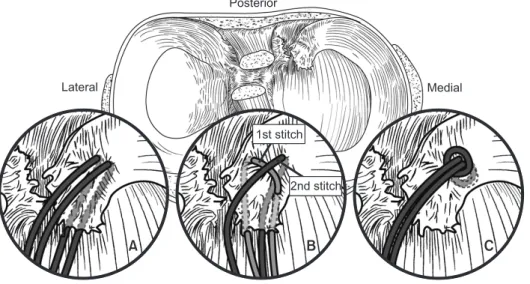
The biomechanical properties and the clinical results of various suture configurations have been reported for pull-out repair of MMPRTs. Various suture techniques ex- ist such as 2 simple sutures, horizontal mattress sutures, modified Mason-Allen sutures, and loop stitch (Fig. 5).
Feucht et al. [49] evaluated 4 different suture configura- tions (2 simple sutures, modified Mason-Allen sutures, horizontal mattress sutures, and 2 modified loop sutures) and found that the modified Mason-Allen suturing pro- vided the strongest tensile strength and holding power in cycling loading and in load-to-failure testing amongst the techniques tested. They also observed that horizontal mattress suturing and 2 modified loop suturing were as- sociated with a significantly higher displacement than the other two techniques. In a cadaveric study, Anz et al.
Fig. 5. Illustrations of the stitch configu- rations for the meniscal root repair; (A) 2 simple sutures, (B) modified Mason- Allen sutures consisting of a horizontal mattress suture (1st stitch) and a simple stitch (2nd stitch), and (C) a loop stitch.
Posterior
Lateral Medial
A B C
2nd stitch 1st stitch
[50] likewise compared the clinical outcomes of 4 differ- ent sutures used for meniscal root fixation (2 simple su- tures, an inverted mattress suture, 1 double-locking loop suture, and 2 double-locking loop sutures) and found that the failure loads of the 2 double-locking loop sutures were higher than those of the other suturing techniques.
Lee et al. [51] compared the clinical and radiographic re- sults of Mason-Allen sutures and those of simple sutures in 50 patients who underwent an arthroscopic meniscal repair. There were no significant differences between the techniques with respect to clinical outcomes, but the patients who received Mason-Allen suturing were associ- ated with less meniscal extrusion and less degeneration of the articular cartilage as seen through follow-up MRI than those who received simple sutures.
Clinical outcomes
The ideal treatment for meniscal root tears is yet to be determined. Several studies have investigated and evalu- ated the clinical outcomes after conservative treatment, meniscectomy, and meniscal repair of MMPRTs. The clinical results of these studies are summarized in Table 2 [6,7,13,18,28,48,52]. Historically, partial meniscectomy was the treatment of choice for radial tears involving the meniscus root. In a retrospective study by Ozkoc et al.
[28] that evaluated 67 patients who had received partial meniscectomy for MMPRTs, parameters of clinical out- comes (i.e., the Lysholm score in their study) was shown to be improved among patients but degeneration of the articular cartilage was shown to have worsened. They concluded that although partial meniscectomy provides moderate symptomatic relief in patients with MMPRTs, it cannot prevent articular degeneration, as determined radiographically. However, Bin et al. [13] reported that among 96 patients with MMPRTs who were treated with partial meniscectomy, most patients showed a significant improvement in terms of postoperative clinical out- comes. Thus, they concluded that partial meniscectomy can help patients with low morbidity.
The majority of the clinical studies available suggest that meniscal repairs should be considered as the first- line treatment for MMPRTs rather than partial meniscec- tomy because repairs allow meniscal continuity, integrity, and biomechanical properties to be restored, allowing the meniscus to withstand hoop stress, and symptoms to resolve. Chung et al. [52] reported that although 35%
of patients who received meniscectomy required revi- sion surgery using total knee arthroplasty, none who
received meniscal repair required it. Further, they found that meniscectomy was associated with a 5-year survival rate of only 75% among patients; whereas, meniscal re- pair was associated with a 100% 5-year survival rate. In their comparative study of meniscal surgical techniques, with a mean follow-up period of 48.5 months, Kim et al. [6] found that the clinical outcomes, postoperative Lysholm and IKDC subjective knee scores, significantly improved relative to the preoperative scores in both treat- ment groups (meniscectomy vs repair). But the repair group, who showed less postoperative meniscal extru- sion and a healed meniscus on MRI and on second-look arthroscopy, had better clinical and radiologic results than the meniscectomy group. The authors concluded that for the treatment of medial meniscus root tears the arthroscopic pullout repair provides better clinical and radiographic outcomes in the long-term than partial meniscectomy and has a higher potential to completely heal the meniscus, faciliating a restored ability of the me- niscus to convert axial load into hoop stress. When Lee et al. [7] retrospectively evaluated 20 consecutive patients who underwent arthroscopic pull-out suture repair for MMPRTs, they observed a significant improvement in HSS and Lysholm knee scores at a mean follow-up of 31.8 months after repair. Furthermore, they observed only a single case of exacerbated Kellgren-Lawrence radio- graphic arthritis. They concluded that the arthroscopic pull out repair for MMPRTs provides symptomatic relief and significant meniscal healing. In contrast, when Seo et al. [53] evaluated the structural integrity of the meniscus after arthroscopic repair in 11 knees with MMPRTs by second-look arthroscopy, although they found that the mean Lysholm score significantly increased (56.1–83.0) at a mean follow-up of 13.4 months, they did not ob- served complete healing in any of the knees (5 cases of loose healing; 4 cases of scar tissue healing; and 2 cases of failed healing were observed). They found that one tear had even progressed to a chondral lesion. They con- cluded that further studies are required to evaluate the correlation between clinical improvement and mensical healing, incomplete or failed.
Arthroscopic repair of MMPRTs is currently considered as the treatment of choice [15,53]. However, there is an unanswered question as to which surgical technique—
the transtibial pullout suture technique versus the suture anchor technique—is better [11]. The transtibial pullout suture technique for root repair has inherent disad- vantages. In response, the suture anchor technique has
Table 2. Summary for clinical outcomesa StudyYearLevel of evidenceStudy designNo. of patientsFollow-up duration OutcomesConclusion Ozkoc et al. [28]2008IVPartial meniscectomy6756.7 mo (range, 8–123 mo)The mean Lysholm score improved from 53 to 67. The average KL grade increased significantly; grade 2 (pre- operative; range, 0–3) to grade 3 (postoperative; range, 2–4)
Partial meniscectomy for MMPRTs provides symptomatic relief but does not prevent progression of radiographic osteoarthritis. Bin et al. [13]2004IVPartial meniscectomy9628.3 mo (range, 12–52 mo)The average Lysholm score increased from 68 to 83.4Partial meniscectomy helps to improve subjective symptoms in elderly patients with degenerated articular cartilage. Chung et al. [52]2015IIIPartial meniscectomy (group M) vs Pullout suture repair (group R)
57 (20 vs 37)More than 5 yrThe mean Lysholm score and IKDC score; both groups showed a significant improvement, but a better result was found for group R compared to group M. The 5-year survival rates; 75% in groups M and 100% in group R (P < 0.001).
Arthroscopic repair was more effective than partial meniscectomy in terms of the clini- cal and radiologic outcomes and survival for at least the 5-year follow-up. Although both groups failed to prevent progression of arthritic change, repair delayed the progression of arthritic change more than partial meniscectomy. Kim et al. [6]2011IIIPartial meniscectomy vs Pullout suture repair58 (28 vs 30)48.5 moA significant improvement (P < 0.05) in Lysholm and IKDC scores was found in both groups. Comparison of the Lysholm and IKDC scores, joint space narrow- ing, and progression of KL between the repair and the partial meniscectomy groups showed that the former had better results. Also, the success rate of healing was higher in the repair group (93.3%).
Arthroscopic pullout repairs of MMPRTs gave significantly better clinical and radio- logic results than partial meniscectomy, and meniscal healing with restoration of hoop tension was observed on MRI and second-look arthroscopy. Lee et al. [7]2009IVPullout suture repair2031.8 mo (range, 24–48 mo)The KL grade increased in only 1 knee. Meniscal healing was observed in all repaired menisci without additional chondral lesions on second-look arthroscopy. The HSS and Lysholm knee scores improved postoperatively.
Arthroscopic pullout suture repair is an ef- fective treatment for posterior root tears of the medial meniscus with degenerated articular cartilage of less than grade III. All cases had no definitive degenerative arthritic changes at the limited short-term follow-up. Jung et al. [48]2012IVSuture anchor repair1330.8 mo (range, 24–40 mo)No patients had joint line tenderness or effusion, or were positive for the McMurray test, postoperatively. A significant improvement in Tegner activity level and in Lysholm score was found. The mean medial meniscal extrusion was 3.9 mm preoperatively and 3.5 mm post- operatively (P > 0.05).
This study demonstrates a symptomatic improvement after meniscal root repair, using suture anchors. However, follow-up MRI scans does not show complete heal- ing of all repair attempts. Kim et al. [18]2011IIIPullout suture repair vs Suture anchor repair45 (22 vs 23)25.9 mo (range, 24–27)Significant improvement in function and meniscal extrusion were found in both groups (P < 0.05) but no significant differences in KL grade or gap distance on MRI were found in both groups (P > 0.05). Complete structural healing was observed in 11 cases in the pull- out suture group and in 12 cases in the suture anchor group (P > 0.05).
This study demonstrates significant func- tional improvement in both the suture anchor repair and pullout suture repair groups. Reduction of meniscal extrusion seems to be appropriate to preserve the protective role of the meniscus against car- tilage degeneration after an MMPRT repair. KL, Kellgren-Lawrence radiographic grade; MMPRT, medial meniscal posterior root tear; IKDC, International Knee Documentation Committee subjective score; MRI, magnetic resonance imaging; HSS, Hospital for Special Surgery score.
evolved to compensate for the disadvantages associated with the pullout technique. Because arthroscopic knot using suture anchor technique is placed directly on the meniscus using a knot pusher, the suture anchor tech- nique can help to achieve theoretically a more precise tensioning during repair. Jung et al. [48] reviewed that 13 patients with MMPRT underwent all-inside repair with suture anchors. A significant improvement in the both the Tegner activity level and the Lysholm score were seen.
But one patient who had loosening of the suture anchor underwent arthroscopic anchor removal 8 months post- operatively. When the outcomes of 22 MMPRT repairs using arthroscopic suture anchors were compared to those of 23 repairs using pullout sutures, Kim et al. [18]
found that the postoperative functional scores were sig- nificantly improved from their respective preoperative scores, but the Kellgren-Lawrence grade did not improve after treatment in both groups. While clinical and radio- logic outcomes did not statistically differ between the groups, a higher rate of meniscal healing was observed in the suture anchor group than the pullout suture group.
Failed repairs, retears, and cartilage degeneration are amongst the most prevalent complications after menis- cal repair, although their exact prevalence remains to be studied. Careful attention should be paid to avoid other complications such as neurovascular injuries associated with guide-pin insertion, iatrogenic injury to cruciate ligaments, and postoperative complications, such as in-
fections, arthrofibrosis, and deep venous thrombosis [40].
CONCLUSION
Given the growing understanding of the importance of meniscal root attachments and of their functional signifi- cance, the increasing accuracy in the identification and treatment of root tears is not surprising. Better results are being demonstrated for meniscal repairs, indepen- dently of the technique used, than for meniscectomy, providing that a strict patient selection is performed.
Although much of the current studies demonstrate clini- cal and biomechanical efficacy of MMPRT repairs, the optimal treatment method for meniscal tears is still to be established. And this controversy is largely because there remains an unresolved issue of inconsistency and applicability of findings due to the diversity in contexts in which the studies were carried out in the existing lit- erature and because the majority of the current studies present level III or IV evidence. Therefore, high quality, randomized-controlled trials are required to robustly de- termine the biomechanical consequences of root repairs and the most optimal repair technique for MMPRTs.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Koenig JH, Ranawat AS, Umans HR, Difelice GS. Meniscal root tears: diagnosis and treatment. Arthroscopy 2009;25:1025-32.
2. Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechani- cal consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. J Bone Joint Surg Am 2008;90:1922-31.
3. Pagnani MJ, Cooper DE, Warren RF. Extrusion of the medial me- niscus. Arthroscopy 1991;7:297-300.
4. Lerer DB, Umans HR, Hu MX, Jones MH. The role of meniscal root pathology and radial meniscal tear in medial meniscal extru- sion. Skeletal Radiol 2004;33:569-74.
5. Hein CN, Deperio JG, Ehrensberger MT, Marzo JM. Effects of medial meniscal posterior horn avulsion and repair on meniscal displacement. Knee 2011;18:189-92.
6. Kim SB, Ha JK, Lee SW, et al. Medial meniscus root tear refix- ation: comparison of clinical, radiologic, and arthroscopic find- ings with medial meniscectomy. Arthroscopy 2011;27:346-54.
7. Lee JH, Lim YJ, Kim KB, Kim KH, Song JH. Arthroscopic pullout suture repair of posterior root tear of the medial meniscus: radio-
graphic and clinical results with a 2-year follow-up. Arthroscopy 2009;25:951-8.
8. Johnson DL, Swenson TM, Livesay GA, Aizawa H, Fu FH, Harner CD. Insertion-site anatomy of the human menisci: gross, ar- throscopic, and topographical anatomy as a basis for meniscal transplantation. Arthroscopy 1995;11:386-94.
9. Johannsen AM, Civitarese DM, Padalecki JR, Goldsmith MT, Wijdicks CA, LaPrade RF. Qualitative and quantitative anatomic analysis of the posterior root attachments of the medial and lat- eral menisci. Am J Sports Med 2012;40:2342-7.
10. Śmigielski R, Becker R, Zdanowicz U, Ciszek B. Medial meniscus anatomy-from basic science to treatment. Knee Surg Sports Traumatol Arthrosc 2015;23:8-14.
11. Nicholas SJ, Golant A, Schachter AK, Lee SJ. A new surgical technique for arthroscopic repair of the meniscus root tear. Knee Surg Sports Traumatol Arthrosc 2009;17:1433-6.
12. Ziegler CG, Pietrini SD, Westerhaus BD, et al. Arthroscopically pertinent landmarks for tunnel positioning in single-bundle and double-bundle anterior cruciate ligament reconstructions. Am J
Sports Med 2011;39:743-52.
13. Bin SI, Kim JM, Shin SJ. Radial tears of the posterior horn of the medial meniscus. Arthroscopy 2004;20:373-8.
14. Vedi V, Williams A, Tennant SJ, Spouse E, Hunt DM, Gedroyc WM.
Meniscal movement. An in-vivo study using dynamic MRI. J Bone Joint Surg Br 1999;81:37-41.
15. Papalia R, Vasta S, Franceschi F, D’Adamio S, Maffulli N, Denaro V. Meniscal root tears: from basic science to ultimate surgery. Br Med Bull 2013;106:91-115.
16. Hwang BY, Kim SJ, Lee SW, et al. Risk factors for medial menis- cus posterior root tear. Am J Sports Med 2012;40:1606-10.
17. Mariani PP, Iannella G, Cerullo G, Giacobbe M. Avulsion of both posterior meniscal roots associated with acute rupture of the anterior cruciate ligament. J Orthop Traumatol 2015;16:259-62.
18. Kim JH, Chung JH, Lee DH, Lee YS, Kim JR, Ryu KJ. Arthroscopic suture anchor repair versus pullout suture repair in posterior root tear of the medial meniscus: a prospective comparison study.
Arthroscopy 2011;27:1644-53.
19. Guermazi A, Hayashi D, Jarraya M, et al. Medial posterior menis- cal root tears are associated with development or worsening of medial tibiofemoral cartilage damage: the multicenter osteoar- thritis study. Radiology 2013;268:814-21.
20. Sung JH, Ha JK, Lee DW, Seo WY, Kim JG. Meniscal extrusion and spontaneous osteonecrosis with root tear of medial menis- cus: comparison with horizontal tear. Arthroscopy 2013;29:726- 32.
21. Robertson DD, Armfield DR, Towers JD, Irrgang JJ, Maloney WJ, Harner CD. Meniscal root injury and spontaneous osteonecrosis of the knee: an observation. J Bone Joint Surg Br 2009;91:190-5.
22. Marzo JM, Gurske-DePerio J. Effects of medial meniscus poste- rior horn avulsion and repair on tibiofemoral contact area and peak contact pressure with clinical implications. Am J Sports Med 2009;37:124-9.
23. Seil R, Dück K, Pape D. A clinical sign to detect root avulsions of the posterior horn of the medial meniscus. Knee Surg Sports Traumatol Arthrosc 2011;19:2072-5.
24. Bae JH, Paik NH, Park GW, et al. Predictive value of painful pop- ping for a posterior root tear of the medial meniscus in middle- aged to older Asian patients. Arthroscopy 2013;29:545-9.
25. Kim YM, Joo YB, Cha SM, Hwang JM. Role of the mechanical axis of lower limb and body weight in the horizontal tear and root ligament tear of the posterior horn of the medial meniscus. Int Orthop 2012;36:1849-55.
26. Shelbourne KD, Dickens JF. Digital radiographic evaluation of medial joint space narrowing after partial meniscectomy of buck- et-handle medial meniscus tears in anterior cruciate ligament- intact knees. Am J Sports Med 2006;34:1648-55.
27. Moon HK, Koh YG, Kim YC, Park YS, Jo SB, Kwon SK. Prognostic factors of arthroscopic pull-out repair for a posterior root tear of the medial meniscus. Am J Sports Med 2012;40:1138-43.
28. Ozkoc G, Circi E, Gonc U, Irgit K, Pourbagher A, Tandogan RN.
Radial tears in the root of the posterior horn of the medial menis- cus. Knee Surg Sports Traumatol Arthrosc 2008;16:849-54.
29. De Smet AA, Blankenbaker DG, Kijowski R, Graf BK, Shinki K.
MR diagnosis of posterior root tears of the lateral meniscus us- ing arthroscopy as the reference standard. AJR Am J Roentgenol
2009;192:480-6.
30. Lim D, Lee YH, Kim S, Song HT, Suh JS. Fat-suppressed volume isotropic turbo spin echo acquisition (VISTA) MR imaging in evalu- ating radial and root tears of the meniscus: focusing on reader- defined axial reconstruction. Eur J Radiol 2013;82:2296-302.
31. Umans H, Morrison W, DiFelice GS, Vaidya N, Winalski CS. Poste- rior horn medial meniscal root tear: the prequel. Skeletal Radiol 2014;43:775-80.
32. Lee SY, Jee WH, Kim JM. Radial tear of the medial meniscal root:
reliability and accuracy of MRI for diagnosis. AJR Am J Roent- genol 2008;191:81-5.
33. Choi CJ, Choi YJ, Lee JJ, Choi CH. Magnetic resonance imaging evidence of meniscal extrusion in medial meniscus posterior root tear. Arthroscopy 2010;26:1602-6.
34. Bhatia S, LaPrade CM, Ellman MB, LaPrade RF. Meniscal root tears: significance, diagnosis, and treatment. Am J Sports Med 2014;42:3016-30.
35. Park HJ, Kim SS, Lee SY, et al. Medial meniscal root tears and meniscal extrusion transverse length ratios on MRI. Br J Radiol 2012;85:e1032-7.
36. Ahn JH, Jeong HJ, Lee YS, et al. Comparison between conserva- tive treatment and arthroscopic pull-out repair of the medial meniscus root tear and analysis of prognostic factors for the determination of repair indication. Arch Orthop Trauma Surg 2015;135:1265-76.
37. Shelbourne KD, Roberson TA, Gray T. Long-term evaluation of posterior lateral meniscus root tears left in situ at the time of anterior cruciate ligament reconstruction. Am J Sports Med 2011;39:1439-43.
38. Neogi DS, Kumar A, Rijal L, Yadav CS, Jaiman A, Nag HL. Role of nonoperative treatment in managing degenerative tears of the medial meniscus posterior root. J Orthop Traumatol 2013;14:193-9.
39. Harner CD, Mauro CS, Lesniak BP, Romanowski JR. Biomechani- cal consequences of a tear of the posterior root of the medial meniscus. Surgical technique. J Bone Joint Surg Am 2009;91 Suppl 2:257-70.
40. Vyas D, Harner CD. Meniscus root repair. Sports Med Arthrosc 2012;20:86-94.
41. Kim YM, Joo YB. Pullout failure strength of the posterior horn of the medial meniscus with root ligament tear. Knee Surg Sports Traumatol Arthrosc 2013;21:1546-52.
42. Lee DW, Ha JK, Kim JG. Medial meniscus posterior root tear: a comprehensive review. Knee Surg Relat Res 2014;26:125-34.
43. Ahn JH, Wang JH, Yoo JC, Noh HK, Park JH. A pull out suture for transection of the posterior horn of the medial meniscus: using a posterior trans-septal portal. Knee Surg Sports Traumatol Ar- throsc 2007;15:1510-3.
44. Raustol OA, Poelstra KA, Chhabra A, Diduch DR. The meniscal ossicle revisited: etiology and an arthroscopic technique for treat- ment. Arthroscopy 2006;22:687.e1-3.
45. Kim YM, Rhee KJ, Lee JK, Hwang DS, Yang JY, Kim SJ. Ar- throscopic pullout repair of a complete radial tear of the tibial attachment site of the medial meniscus posterior horn. Arthros- copy 2006;22:795.e1-4.
46. Padalecki JR, Jansson KS, Smith SD, et al. Biomechanical con-
sequences of a complete radial tear adjacent to the medial meniscus posterior root attachment site: in situ pull-out repair restores derangement of joint mechanics. Am J Sports Med 2014;42:699-707.
47. Engelsohn E, Umans H, Difelice GS. Marginal fractures of the medial tibial plateau: possible association with medial meniscal root tear. Skeletal Radiol 2007;36:73-6.
48. Jung YH, Choi NH, Oh JS, Victoroff BN. All-inside repair for a root tear of the medial meniscus using a suture anchor. Am J Sports Med 2012;40:1406-11.
49. Feucht MJ, Minzlaff P, Saier T, Lenich A, Imhoff AB, Hinterwim- mer S. Avulsion of the anterior medial meniscus root: case report and surgical technique. Knee Surg Sports Traumatol Arthrosc 2015;23:146-51.
50. Anz AW, Branch EA, Saliman JD. Biomechanical comparison
of arthroscopic repair constructs for meniscal root tears. Am J Sports Med 2014;42:2699-706.
51. Lee DW, Kim MK, Jang HS, Ha JK, Kim JG. Clinical and radiologic evaluation of arthroscopic medial meniscus root tear refixation:
comparison of the modified Mason-Allen stitch and simple stitch- es. Arthroscopy 2014;30:1439-46.
52. Chung KS, Ha JK, Yeom CH, et al. Comparison of clinical and ra- diologic results between partial meniscectomy and refixation of medial meniscus posterior root tears: a minimum 5-year follow- up. Arthroscopy 2015;31:1941-50.
53. Seo JH, Li G, Shetty GM, et al. Effect of repair of radial tears at the root of the posterior horn of the medial meniscus with the pullout suture technique: a biomechanical study using porcine knees. Arthroscopy 2009;25:1281-7.