J Korean Soc Transplant
2008;22:138-141 □
증 례
□138
책임저자:김상일, 서울시 서초구 반포동 505 강남성모병원 내과, 137-701 Tel: 02-590-2710, Fax: 02-599-3589 E-mail: drksi@catholic.ac.kr
Cryptosporidiosis in a Small Bowel Transplant Recipient
Departments of
1Internal Medicine,
2Surgery,
3Laboratory Medicine,
4Parasitology, Kangnam St. Mary’s Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea
Youn Jeong Kim, M.D.
1, Sang Il Kim, M.D.
1, Yang Ree Kim, M.D.
1, Ik-Jun Choi, M.D.
1, Myung Duk Lee, M.D.
2, Yeon Joon Park, M.D.
3, Ho Woo Nam, M.D.
4and Moon Won Kang, M.D.
1소장이식 후 발생한 장 크립토스포리디움증 1예
가톨릭대학교 의과대학 1내과학교실, 2외과학교실, 3진
단검사의학과, 4기생충학교실
김윤정
1ㆍ김상일
1ㆍ김양리
1ㆍ최익준
1ㆍ이명덕
2ㆍ박 연준
3ㆍ남호우
4ㆍ강문원
1소장 이식 후 환자에서 설사는 비교적 흔하게 나타날 수 있는 중요한 증상으로, 감염성 원인과 비감염성 원인으로 나눌 수 있다. 감염성 원인으로는 거대 세포 바이러스나 Epstein-Barr virus, 아데노 바이러스, Clostridium difficile, Entamoeba histolytica, Giardia lamblia, Cryptosporidium이 있으며 비감염성 원인으로는 cyclosporine, tacrolimus과 같 은 면역억제제의 사용이나 이식거부반응이 있을 수 있다.
이 중 Cryptosporidium은 소화기, 담도, 호흡기계 상피세포 를 감염시키는 원충으로 정상환자에서는 경한 질환을 일 으켜 특별한 치료 없이 회복될 수 있으나, 사람면역결핍바 이러스 감염 환자나 장기 이식 환자와 같이 면역저하 환 자에서는 치명적일 수 있다. 저자는 설사를 주소로 내원한 소장이식 환자에서 반복적인 분변검사를 통해 cryptospori- diosis를 진단하였고 paromomycin으로 효과적으로 치료하 였기에 문헌 고찰과 함께 보고하는 바이다. 장기 이식 후 발생한 설사 환자에서 그 원인을 밝히는 것은 쉽지 않으 므로 신선한 검체를 이용한 반복적인 검사가 반드시 필요 하며, 흔하지는 않으나 Cryptosporidium이 이식 환자 설사 의 원인일 수 있으므로 분변의 항산성 검사를 고려해야 할 것이다. (대한이식학회지 2008;22:138-141)
중심 단어: 소장이식, 크립토스포리디움, 설사
INTRODUCTION
Cryptosporidum is a common intestinal protozoa often causing
self-limited watery diarrhea for several days in immunocom- petent persons. However, in immunocompromised individuals, including HIV-infected patients and transplant recipients, severe life-threatening illness can develop.(1) Older reports without the inclusion of HIV infected patients have documented oocysts in 1∼3% of specimens in the general population from industrialized countries of Europe and North America.(2) Most studies from developing countries have documented the prevalence of Cry- ptosporidium to be 5% to 10% of the general population.(2) In a review of 5,262 inhabitants of Korea, YU et al. reported the overall positive rate of human cryptosporidiosis was 3.3%
in several rural areas of Korea.(3) In transplant recipients, especially for small bowel transplants, diarrhea is a significant symptom commonly observed with rejection or infections caused by virus, bacteria and parasites. Thousands of solid organ transplants are performed annually in Korea; however, this is the first case report of cryptosporidiosis confirmed in a trans- plant recipient. We describe a case of cryptosporidial infection in a recipient of a small bowel transplant.
CASE REPORT
A 59-year-old female was admitted to Kangnam St. Mary’s hospital, a university-affiliated teaching hospital. The patient complained of profuse watery diarrhea and abdominal pain. She had undergone a small bowel transplantation for the short bowel syndrome after massive small bowel resection for the superior mesenteric artery syndrome, two years ago. There were no episodes of rejection. She was maintained on tacrolimus (2.5 mg per day) and deflazacort (6 mg per day). The vital signs were normal. The physical examination showed moderate dehydration and mild lower abdominal tenderness; it was otherwise unremarkable. There was no history of mucoid or bloody stool. The white blood cell count was 9,850/mm3, with 67.2% polymorphonuclear cells, 22.5% lymphocytes, 8.9%
monocytes, and 1.2% eosinophils. The hematocrit was 32.3%
Youn Jeong Kim, et al:Cryptosporidiosis in a Small Bowel Transplant Recipient 139
Fig. 1. Endoscopic biopsy. (A) H-E stain ×100. (B) AFB stain ×400. The endoscopic biopsy of the transplanted intestine showed only hyperemia without evidence of rejection.
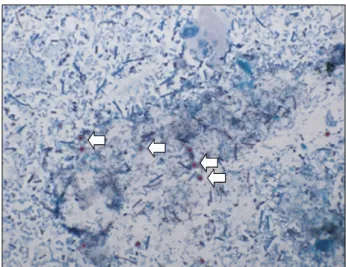
Fig. 2. Stool modified-AFB stain ×1,000. Repeated fresh stool smear though modified acid-fast stain revealed red-stained cryptosporidial oocysts.
and the platelet count was 237,000/mm3. Bacterial, fungal and mycobacterial blood cultures were negative. The routine stool culture for Salmonella, Shigella, Campylobacter, and Yersinia was also negative. In addition, the examination for ova and parasites was negative. Serum ELISA (Enzyme-linked immuno- sorbent assay) testing for paragonimiasis, cysticercosis, spar- ganosis, toxoplasmosis, and facioliasis was negative. CMV antigenemia and Rota virus antigen were negative. The tacrolimus level was 4.8 ng/mL, a level within normal range. The endo- scopy showed normal-appearing mucosa, and a biopsy of the transplanted intestine revealed no evidence of rejection (Fig. 1).
Fresh stool was obtained from the patient for microscopic examination and several cryptosporidial oocysts were found using a modified acid-fast stain (Fig. 2). The patient was treated with oral paromomycin (500 mg three times a day) for three weeks and the dose of tacrolimus was decreased to 2 mg per day and the deflazacort was decreased to 3 mg per day. After two weeks, the follow-up stool smear, including acid-fast staining, showed that the cryptosporidial oocysts were much decreased. The patient was discharged in good condition.
Recurrence of the cryptosporidium occurred six months and 1 year later without diarrhea. She did not receive any antimi- crobial agents, and is under continous observation.
DISCUSSION
Diarrhea is common in small bowel transplant recipients as a result of infection or rejection. It is important to determine the etiology because the treatments differ. For example, the
immunosuppressant agents would be increased or decreased depending on the diagnosis. Therefore, treatment decisions can be difficult in cases with no specific etiology identified for the diarrhea.
There are only a few published reports on diarrhea in small bowel transplant recipients. In 2005, Ziring D. reported that among 33 intestinal transplantation recipients, 13 (39%) deve- loped 20 episodes of infectious enteritis. More specificity, 14 viral, 3 bacterial and 3 protozoal infections. The infectious etiologies of the protozoa included one G.lambilia and two Cryptosporidium sp.(4) The parasitic enteritis occurred at a
140 대한이식학회지:제 22 권 제 1 호 2008
median of 183 (51∼298) days after the intestinal transplantation in this report.(4) In 2005, a report on three cases with Cryptosporidium and one with Microsporidium infection, in small bowel transplant recipients, showed that the timing of cryptosporidiosis varied from 6 days to 4 years.(5) Our patient was diagnosed with an enteritis due to Cryptosporidium two years after a small bowel transplant. High doses of immunosu- ppressant and immunological factors, involving the intestinal graft, may be related to the development of cryptosporidiosis in the intestinal transplant recipient.
Cryptosporidiosis is a mucosal infection caused by parasites of the genus Cryptosporidium. The infection causes diarrhea that is self-limited in immunocompetent human hosts. However, it can be severe in persons with AIDS and other forms of immunocompromise. In such patients, the severity and duration of clinical illness is strictly related to the level of immuno- suppression.(1,6)
Like most intestinal parasites, Cryptosporidium infection is usually diagnosed by microscopic examination of the stool.
However, trichrome staining used in routine parasitological in- vestigations is not useful for the diagnosis of Cryptosporidium infection. Demonstration of red-stained oocysts with special acid-fast staining over a blue background is diagnostic for Cryptosporidium infection.(7,8) The diagnosis of Cryptosporidium infection is difficult to establish. Therefore, frequently it is necessary to repeat the fresh stool examination in immunocom- promised patients with profuse diarrhea. More recently, immu- nofluorescent assays employing oocyst specific monoclonal antibodies are commonly used to test for cryptosporidiosis, which have been reported to be more sensitive than acid-fast staining.(9) Antigen-detection assays and PCR testing have also been used for Cryptosporidium detection.(10,11) We used only acid-fast staining in this case; the red stained oocysts, with the acid-fast staining, confirmed the Cryptosporidium.
As of 2000, there were 10 recognized species of Crypto- sporidium.(12) Most human isolates are thought to belong to a single species, Cryptosporidium parvum. Recent molecular biology studies have demonstrated that Cryptosporidium parvum includes a number of genotypes and occult species. In this case we did not evaluate the specimen for the species by molecular biology studies.
Paromomycin has been an effective drug for cryptos- poridiasis in some patients infected with HIV.(13) Nitazoxanide suspension, currently available in the Unites States, was appro- ved for treatment of cryptosporidiasis and giardiasis in children, in 2002. Because the treatment with single drugs have had limited effects, studies have investigated the effects of drug
combinations.(14) We treated our patient with paromomycin because nitazoxanide is not available in Korea. Azithromycin may interact with immunosuppressive agents and is generally avoided due to the risk of rejection. In addition, since it is important to restore the immune response for the treatment of cryptosporidiasis, in immune compromised patients, we modified the doses of the immunosuppressants. Our patient tolerated the treatment and had only moderate GI disturbance with the oral paromomycin therapy. Despite frequent reports of Cryptospo- ridium infection, there have been only three reports of human Cryptosporidium diarrhea in small bowel transplant patients worldwide to date.(4,5,15) We report a case of cryptosporidiosis in a small bowel transplant recipient who was diagnosed by modified acid-fast staining of a fecal smear.
REFERENCES
1) Farthing MJ. Clinical aspects of human cryptosporidiosis.
Contrb Microbio 2000;6:50-74.
2) Guerrant R. Cryptosporidiosis: an emerging, highly infectious threat. Emerg Infect Dis 1997;3:51-7.
3) Yu JR, Lee JK, Seo M, Kim SI, Sohn WM, Huh S, Choi HY, Kim TS. Prevalence of cryptosporidiosis among the villagers and domestic animals in several rural areas of Korea. Korean J Parasitol 2004;42:1-6.
4) Ziring D, Tran R, Edelstein S, McDiarmid SV, Vargas J, Cortina G, Gajjar N, Ching N, Cherry J, Krogstad P, Renz JF, Fondevila C, Busuttil RW, Farmer DG. Infectious enteritis After intestinal transplantation: incidence, timing, and outcome.
Transplantation 2005;79:702-9.
5) Delis SG, Tector J, Kato T, Mittal N, Weppler D, Levi D, Ruiz P, Nishida S, Nery JR, Tzakis AG. Diagnosis and treatment of cryptosporidium infection in intestinal transplant recipients. Transplant Proc 2002;34:951-2.
6) Gerber DA, Green M, Jaffe R, Greenberg D, Mazariegos G, Reyes J. Cryptosporidial infections after solid organ transplan- tation in children. Pediatr Transplant 2000;4:50-5.
7) Robin G. Fraser D, Orr N, Sela T, Slepon R, Ambar R, Dagan R, Le Blancq S, Deckelbaum RJ, Cohen D. Cryptosporidium infection in Bedouin infants assessed by prospective evaluation of anticryptosporidial antibodies and stool examination. Am J Epidemiol 2001;153:194-201.
8) Cryptosporidiosis. http://www.dpd.cdc.gov/dpdx/HTML/Crypto- sporidiosis. htm. 2008; March 10
9) Johnston SP, Ballard MM, Beach MJ, Causer L, Wilkins PP.
Evaluation of three commercial assays for detection of Giardia and Cryptosporidium in fecal specimens. J Clin Microbio 2003;41:623-6.
10) Garcia LS, Shimizu RY, Bernard CN. Detection of Giardia lamblia, Entamoeba histolytica/Entamoeba dispar, and Crypto-
Youn Jeong Kim, et al:Cryptosporidiosis in a Small Bowel Transplant Recipient 141
sporidium parvum antigens in human fecal specimens using the triage parasite panel enzyme immunoassay. J Clin Microbiol 2000;38:3337-40.
11) McLauchlin J, Amar CF, Pedraza-Diaz S, Mieli-Vergani G, Hadzic N, Davies EG. Polymerase chain reaction-based diag- nosis of infection with Cryptosporidium in children with primary immunodeficiencies. Pediatr Infect Dis J 2003;22:
329-35.
12) Fayer R, Morgan U, Upton SJ. Epidemiology of Cryptos- poridium: transmission, detection and identification. Int J
parasitol 2000;30:1305-22.
13) Gerald LM, John EB, Raphael DM. Mandell, Douglas, and Bennett’s principles and practice of infectious disease. 6th ed.
Philadelphia, Elsevier; 2005;vol 2, p.3215-28.
14) Smith NH, Cron S, Valdez LM, Chappell CL, White AC Jr.
Combination drug therapy for cryptosporidiosis in AIDS. J Infect Dis 1998;178:900-3.
15) Pozio E, Rivasi F, Caccio SM. Infection with Cryptosporidium hominis and reinfection with Cryptosporidium parvum in a transplanted ileum. APMIS 2004;112:309-13.
Abstract
Episodes of diarrhea are common in transplant recipients; these episodes have a variety of etiologies. Infectious illnesses such as Clostridium difficile and cytomegalovirus (CMV), and the side effects of immunosuppressive medications are the most common causes of diarrhea. However, it is difficult to diagnose most cases.
Cryptosporidium is a coccidian protozoan parasite that affects the epithelial cells of the human gastrointestinal,
biliary and respiratory tracts. It can cause a self-limiting diarrhea in immunecompetent persons. However, it can cause life-threatening illness in immunocompromised patients such as human immunodeficiency virus (HIV) infected patients or in transplant recipients. Here we report the first case, in Korea, of cryptosporidiosis diagnosed by a fecal smear with modified acid-fast staining in a small bowel transplant recipient. The patient was successfully treated with paromomycin. (J Korean Soc Transplant 2008;22:138-141)
Key Words: Small bowel transplant, Cryptosporidium, Diarrhea