분화갑상선암 환자에서 수술 후 재발 감시를 위한 경부 초음파검사
경북대학교 의과대학 외과학교실
정진향
Post-thyroidectomy Neck Ultrasonography for Surveillance in Patients with Differentiated Thyroid Cancer
Jin Hyang Jung
Department of Surgery, Kyungpook National University School of Medicine, Daegu, Korea
Received November 11, 2015 Revised November 11, 2015 Accepted November 12, 2015
Post-thyroidectomy neck ultrasound has become the modality of choice for detection of lo- co-regional recurrence of differentiated thyroid cancer, and it has been well documented in many journal articles and international guidelines. Neck ultrasound for surveillance is a highly sensitive and noninvasive tool but operator-dependent.
Keywords: Differentiated thyroid cancer, Thyroidectomy, Ultrasonography
Correspondence to:
Jin Hyang Jung
Department of Surgery, Kyungpook National University School of Medicine, 807 Hogukno, Buk-gu, Daegu 41404, Korea
Tel: +82-53-200-2166 Fax: +82-53-200-2704 E-mail: [email protected]
서 론
2014년 발표된 중앙암등록본부 자료에 의하면, 우리나 라 갑상선암 전체 발생 건수 가운데 유두암이 97.3%, 여포 암이 1.4%로 분화갑상선암이 대부분을 차지하고 있다.(1) 분화갑상선암은 비교적 서서히 자라며 예후가 양호한 것 으로 알려져 있으나 일차 치료 후 5-20%의 환자는 장기적 으로 재발을 경험하게 된다. 이러한 재발의 약 2/3는 치료 후 첫 10년 이내에 발생하며 60-75%가 경부림프절에, 20%는 갑상선 수술부위(thyroid bed)에 재발하고, 대개 의 재발은 원발암과 동측에 발생한다.(2-5) 분화갑상선
암의 재발이 장기 생존에 미치는 영향에 대해서는 아직 논 란이 있다. 일부 연구에서는 국소재발이 사망의 위험을 5 배까지 증가시킨다고 보고하고 있지만,(6) 국소재발의 유 형에 따라 생존에 다른 영향을 미친다는 보고도 있다.(7) 대부분의 국소재발은 외과적 절제를 포함한 치료에 반응 하는 경우가 많아 상당수가 단기추적관찰에서 무병 상태 를 유지하지만,(8) 결국 8% 정도의 환자는 국소재발로 인 한 사망을 경험하게 된다.(9)
수술 후 재발 감시를 위한 검사로는 혈청 갑상선글로블 린(thyroglobulin, Tg) 및 항갑상선글로블린항체 농도의 측정, 경부 초음파검사 및 방사성요오드 전신스캔 등을 시
REVIEW ARTICLE
J Surg Ultrasound 2015;2:74-80 JSUJournal of Surgical Ultrasound
Table 1. Ultrasound Guidelines for Cervical Node Level and Anatomic Landmark
Level Anatomic landmark Nodal group
IA Midline; Anterior to digastric muscle and superior to hyoid bone Submental
IB Lateral to zone IA, but medial or anterior to submandibular gland Submandibular
II From skull base to hyoid bone IIA / IIB subdivide by spinal accessory nerve Upper jugular
III From hyoid bone to cricoid cartilage lateral to CCA Mid-jugular
IV From cricoid cartilage to clavicle lateral to CCA Lower jugular
V From posterior border of SCM to anterior border of trapezius VA / VB subdivide by cricothyroid cartilage Posterior triangle VI Anterior/medial to CCA from level of hyoid to manubrium prelaryngeal (Delphian), pretracheal, paratracheal Central neck CCA = common carotid artery; SCM = sternocleidomastoid muscle.
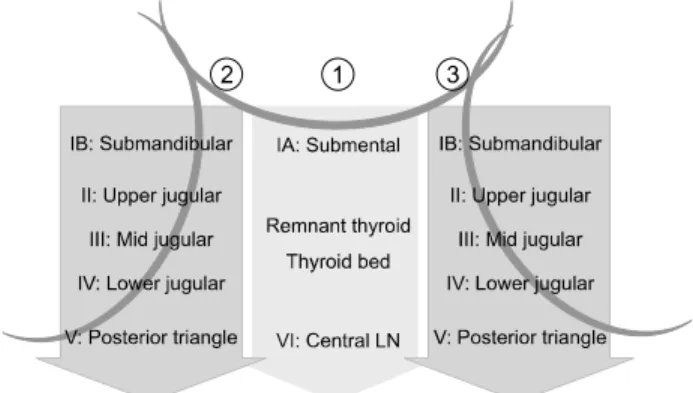
Fig. 1. Scanning techniques of post-thyroidectomy neck ultrasound.
행할 수 있다. 대한갑상선학회 갑상선결절 및 암 진료 권 고안 개정안(10)과 2015년 미국갑상선학회 권고안(11)에 따르면, 갑상선 수술부위와 중앙 및 측경부림프절 구획을 평가하기 위해 경부 초음파검사를 수술 후 6-12개월에 시 행하며, 이 후 환자의 재발 위험성과 Tg 수준에 따라 정기 적으로 시행할 것을 권고하고 있다.
경부 초음파검사는 분화갑상선암 환자에서 경부 재발 및 전이를 발견하는데 매우 예민한 검사로, 빠르고 비침습 적이며 초음파 유도 하 세침흡인세포검사 또는 수술에 용 이하나 검사자에 상당히 의존적인 검사라는 한계를 가지 고 있어 좋은 결과를 위해서는 검사자의 노력이 필수적이 다. 다양한 경험뿐만 아니라 경부의 해부학적 구조와 림프 절 구획 및 감별 질환에 대한 풍부한 지식 또한 필요하다.
본 론
1. 갑상선 수술 후 경부 초음파검사 방법
경부 초음파검사는 고해상도 실시간 초음파 장비로 시 행해야 하며 일반적으로 7-12 MHz의 고주파수 선형 탐촉 자를 사용한다. 검사를 위한 환자의 자세는 누운 상태에서 목을 뒤로 젖힌 자세가 적절하다. 수술 후 재발 감시를 위 한 경부 초음파검사는 적어도 가로스캔과 세로스캔을 포 함하여 두 개 이상의 영상으로 일정한 순서에 따라 일엽절 제술 후 잔여 갑상선, 갑상선 수술부위와 경부림프절 level I-VI까지 빼놓지 않고 관찰하여야 한다(Table 1).(12,13)
검사는 먼저 가로스캔으로 목의 중심 상부 턱끝밑 (submental)의 림프절 level I부터 아래로 흉골 절흔 (sternal notch)까지 진행하며, 갑상선 수술부위와 림프 절 level VI의 중앙경부림프절의 재발 유무를 확인한다.
갑상선 수술부위 검사 시에는 가로스캔이 세로스캔보다 병변을 발견하는데 좀 더 유리하다. 다음으로 환자의 목을 좌측으로 돌리게 한 다음 우측 측경부를 검사한다. 우측 악하선(submandibular gland) 측후방부터 경정맥을 따 라 아래로 상부(level II), 중간(level III), 하부(level IV) 순서로 쇄골까지 검사한 후 세로스캔으로 한번 더 확인한 다. 흉쇄유돌근 후방의 level 5도 귀의 후하방에서 시작하 여 쇄골까지 가로 및 세로스캔을 시행한다. 좌측 측경부도 동일한 방법으로 검사한다(Fig. 1). 이상 소견이 발견되면 환자의 자세를 바꾸거나 탐촉자를 돌려가며 최대한 인공 음영(artifact)을 줄여 실제 병변인지 확인한다.
2. 갑상선 수술부위(thyroid bed)
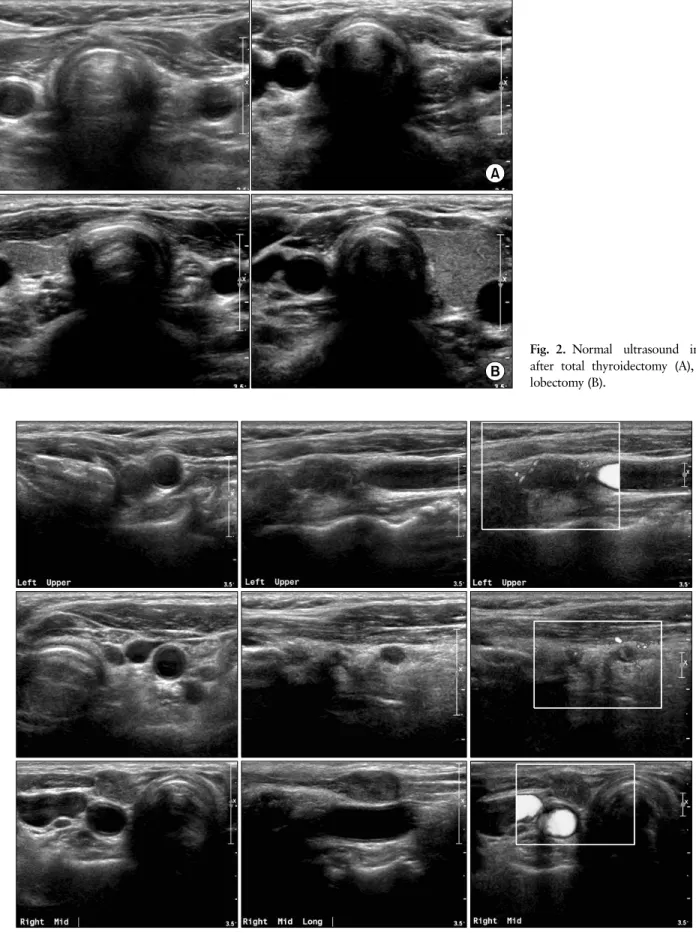
갑상선 절제수술 후 경동맥과 경정맥은 갑상선이 차지 하고 있던 공간으로 이동하게 되어 우측 경동맥은 기도 바 로 옆에 위치하게 되고 좌측은 식도와 인접하여 위치하게 된다(Fig. 2). 이러한 특징으로 수술 후 초음파검사에서 기도와 경동맥 사이에 공간점유병변(space occupying lesion)이 보이면 재발을 의심해봐야 한다. 갑상선 수술부
Fig. 2. Normal ultrasound image after total thyroidectomy (A), and lobectomy (B).
Fig. 3. Ultrasound image of the thyroid bed recurrence.
Fig. 4. Ultrasound image of the recurrence in central lymph node.
Fig. 5. Ultrasound image of normal or benign node in lateral neck.
위의 재발은 실제 수술부위의 재발뿐만 아니라 중앙경부 림프절의 재발일 경우도 있다. 초음파에서 두 재발 병변을 구분하기는 쉽지 않으며, 세침흡인세포검사에서 암세포 주위의 림프조직을 확인함으로써 감별진단이 가능하 다.(14)
갑상선 수술부위 재발암의 초음파 소견은 일반적으로 저에코의 둥근 모양으로, 잘 구분되어지는 경계(well-de- fined margin)를 가진 경우가 많으며, 일부에서 미세석회 화나 낭성 변화를 보이기도 한다(Fig. 3, 4).(14) 그러나 Rondeau 등(15)은 재발 감시를 위한 갑상선 수술부위에 대한 초음파검사는 80%의 민감도와 52%의 특이도를 나 타내어 측경부림프절 전이의 진단에 비해 정확도가 떨어
진다고 보고하였으며 대부분 비특이적 소견으로 아직까 지 명확한 진단 기준은 없는 상태이다.
갑상선 수술부위의 재발암으로 오인할 수 있는 병변으 로는 수술로 인해 생긴 국소적인 조직의 왜곡, 잔여 갑상 선 조직, 봉합육아종(suture granuloma), 부갑상선종, 양성 림프절이 있으며 이 외에도 띠근육(strap muscle), 기도 연골, 추체엽(pyramidal lobe), 및 수술 후 섬유화, 낭종, 지방 괴사 등도 종종 재발암으로 오인할 수 있 다.(14,16) 봉합육아종은 수술 중 사용하는 봉합사 주변으 로 육아종이 발생하는 것으로 내부에 석회화와 유사한 고 에코의 점(spot)을 가진 저에코의 결절 형태로 나타나며, 재발암의 초음파 소견과 잘 구분이 되지 않는다. 봉합육아
Fig. 6. Ultrasound image of malignant lymph node.
종을 좀 더 시사하는 소견은 내부의 고에코가 결절의 중심 에 위치하며 1 mm 보다 크고 거칠며 가상의 선을 따라 여 러 개가 보인다는 것이다. 또한 시간이 지나면서 줄어들거 나 없어지는 경우도 있다. 초음파로 구분이 어렵다면 세침 흡인세포검사를 통해 육아조직이나 거대세포 반응(giant
cell reaction), 이물 육아종 등을 확인하면 감별이 가능하 다.(17-19)
3. 경부 림프절(cervical lymph node)
경부에 존재하는 정상 림프절은 나이가 들수록 초음파
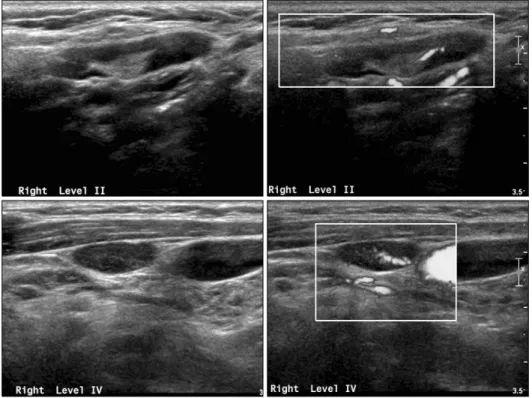
에서 보이는 숫자가 늘어난다.(12) 크기는 3-25 mm로 다 양하며 특히 턱밑과 상부 경정맥 주위의 림프절들이 크기 가 크다.(12,20) 정상 또는 양성 림프절의 초음파 소견은 타원형의 저에코 피질(cortex) 중심부에 고에코의 지방문 (echogenic hilum)이 존재하며 도플러 검사에서 지방문 을 따라 혈류 패턴을 확인할 수 있다. 고에코 지방문은 양 성 림프절의 강력한 예측인자이나 크기가 작은 림프절의 경우 고에코 지방문이나 혈류를 확인하기 어려운 경우도 있다. 그러므로 하나의 진단 기준이 아닌 여러 초음파 소 견들을 고려하여야 한다(Fig. 5).(14,21)
경부림프절 재발을 의심할 수 있는 초음파 소견으로는 둥근 모양 또는 불규칙한 모양, 지방문의 소실, 도플러 검 사에서 주변부 또는 불규칙한 혈류 소견, 미세석회화, 낭 성 변화 등이 있다.(14,22) 갑상선 유두암의 림프절 전이 의 경우에는 림프절 내 갑상선글로블린으로 인해 내부 에 코가 증강(hyperechoic)되어 보일 수도 있다(Fig. 6).(12)
분화갑상선암에서 경부 림프절 전이에 대한 초음파 진 단 기준들의 정확도는 림프절 단위 분석으로 초음파 소견 과 병리소견을 비교 분석한 연구들에 의하면 림프절의 높 은 에코, 석회화, 낭성 변화, 이상 혈류 소견은 각각 예민 도가 86%, 12-50%, 11-21%, 86%였으며, 특이도는 96%, 100%, 100%, 82%로, 석회화와 낭성 변화는 100% 특이도 를 보이는 악성 림프절의 특징적인 소견이나 예민도가 낮 은 단점을 보였다. 림프절 모양이나 크기, 고에코 지방문 의 소실 소견들은 다양한 진단율이 보고되고 있으며, 상대 적으로 진단적 정확도와 특이도가 낮았다.(23,24)
4. 초음파 해석 및 보고서
갑상선 수술 후 초음파검사에서 확인된 병변에 대해서 는 세침흡인세포검사 시행 여부 결정과 이후 추적검사에 서 변화 유무를 확인하기 위해 자세한 판독 소견과 각각의 병변에 대한 해석을 기록해 두어야 한다. 림프절의 위치는 림프절 level (Table 1)에 따라 기록하고 크기는 장경, 단 경, 높이의 세 단면에서 측정한다. 각각의 초음파 소견을 따로 기록하고 도플러 검사에서 림프절의 혈류 패턴은 지 방문(hilar), 주변부(peripheral), 혼합형(mixed), 무혈 류(absence)로 분류하여 기록한다. 결절이나 림프절의 위 치, 크기, 초음파 및 도플러 검사 소견 등을 종합하여 양성 (benign), 불확정(indeterminate), 의심(suspicious) 병 변으로 분류한다.(14)
5. 초음파 유도 하 세침흡인세포검사
초음파에서 국소재발이 의심되는 경우에 다른 질환과 의 감별진단을 위해서는 초음파 유도 하 세침흡인세포검 사가 도움이 된다. 또한, 흡인물의 갑상선글로블린의 측 정이 진단의 민감도를 향상시킬 수 있다.
결 론
경부 초음파검사는 분화갑상선암 환자에서 국소 재발 및 전이를 발견하는데 매우 예민한 검사 방법이며 국소 재 발의 세포학적 진단뿐만 아니라 치료 과정에도 유용하게 활용할 수 있다. 그러나 초음파검사는 검사자 의존도가 높 은 한계를 가지고 있어 좋은 결과를 위해서는 검사자의 노 력이 필수적이다.
REFERENCES
1. National Cancer Information Center. 2012 Annual da- ta report [Internet]. Available from: http://www.
cancer.go.kr.
2. Mazzaferri EL, Kloos RT. Clinical review 128: Current approaches to primary therapy for papillary and fol- licular thyroid cancer. J Clin Endocrinol Metab 2001;
86:1447-63.
3. Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med 1998;338:297-306.
4. Sherman SI. Thyroid carcinoma. Lancet 2003;361:
501-11.
5. Frasoldati A, Pesenti M, Gallo M, Caroggio A, Salvo D, Valcavi R. Diagnosis of neck recurrences in pa- tients with differentiated thyroid carcinoma. Cancer 2003;97:90-6.
6. Lundgren CI, Hall P, Dickman PW, Zedenius J.
Influence of surgical and postoperative treatment on survival in differentiated thyroid cancer. Br J Surg 2007;94:571-7.
7. Stojadinovic A, Shoup M, Nissan A, Ghossein RA, Shah JP, Brennan MF, et al. Recurrent differentiated thyroid carcinoma: biological implications of age, method of detection, and site and extent of recurrence.
Ann Surg Oncol 2002;9:789-98.
8. Kloos RT, Mazzaferri EL. A single recombinant hu- man thyrotropin-stimulated serum thyroglobulin measurement predicts differentiated thyroid carcino- ma metastases three to five years later. J Clin En- docrinol Metab 2005;90:5047-57.
9. Mazzaferri EL, Jhiang SM. Long-term impact of ini-
tial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med 1994;97:418-28.
10. Yi KH, Park YJ, Koong SS, Kim JH, Na DG, Ryu JS, et al. Revised Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Thyroid Cancer. Korean J Otorhinolaryngol-Head Neck Surg 2011;54:8-36.
11. Haugen BR Md, Alexander EK, Bible KC, Doherty G, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid, 2015 (in press).
12. Bieker TM. Scanning the post-thyroidectomy neck:
appearance and technique. JDMS 2009;26:215-23.
13. Stack BC Jr, Ferris RL, Goldenberg D, Haymart M, Shaha A, Sheth S, et al; American Thyroid Association Surgical Affairs Committee. American Thyroid Asso- ciation consensus review and statement regarding the anatomy, terminology, and rationale for lateral neck dissection in differentiated thyroid cancer. Thyroid 2012;22:501-8.
14. Frates MC. Ultrasound in recurrent thyroid disease.
Otolaryngol Clin North Am 2008;41:1107-16.
15. Rondeau G, Fish S, Hann LE, Fagin JA, Tuttle RM.
Ultrasonographically detected small thyroid bed nod- ules identified after total thyroidectomy for differ- entiated thyroid cancer seldom show clinically sig- nificant structural progression. Thyroid 2011;21:845- 53.
16. Shin JH, Han BK, Ko EY, Kang SS. Sonographic findings in the surgical bed after thyroidectomy:
comparison of recurrent tumors and nonrecurrent lesions. J Ultrasound Med 2007;26:1359-66.
17. Kim JH, Lee JH, Shong YK, Hong SJ, Ko MS, Lee DH, et al. Ultrasound features of suture granulomas in the thyroid bed after thyroidectomy for papillary thyroid carcinoma with an emphasis on their differentiation from locally recurrent thyroid carcinomas. Ultrasound Med Biol 2009;35:1452-7.
18. Coquia SF, Chu LC, Hamper UM. The role of sonog- raphy in thyroid cancer. Radiol Clin North Am 2014;52:1283-94.
19. Kwak JY. Postoperative Surveillance of Thyroid Cancer: in View of US. J Korean Thyroid Assoc 2012;
5:15-9.
20. Ying M, Ahuja A. Sonography of neck lymph nodes.
Part I: normal lymph nodes. Clin Radiol 2003;58:351-8.
21. Kuna SK, Bracic I, Tesic V, Kuna K, Herceg GH, Dodig D. Ultrasonographic differentiation of benign from malignant neck lymphadenopathy in thyroid cancer. J Ultrasound Med 2006;25:1531-7.
22. Wunderbaldinger P, Harisinghani MG, Hahn PF, Da- niels GH, Turetschek K, Simeone J, et al. Cystic lymph node metastases in papillary thyroid carcinoma.
AJR Am J Roentgenol 2002;178:693-7.
23. Leboulleux S, Girard E, Rose M, Travagli JP, Sabbah N, Caillou B, et al. Ultrasound criteria of malignancy for cervical lymph nodes in patients followed up for differentiated thyroid cancer. J Clin Endocrinol Metab 2007;92:3590-4.
24. Rosário PW, de Faria S, Bicalho L, Alves MF, Borges MA, Purisch S, et al. Ultrasonographic differentiation between metastatic and benign lymph nodes in pa- tients with papillary thyroid carcinoma. J Ultrasound Med 2005;24:1385-9.