Congenital absence of the portal vein (CAPV) is a rare malformation in which intestinal and splenic venous flow bypasses the liver and drains directly into the sys- temic circulation via a congenital portosystemic shunt.
Variable associated anomalies and clinical manifesta- tions caused by the disrupted enterohepatic circulation in CAPV have been reported, including congenital car- diac anomalies, skeletal and visceral anomalies, hepatic neoplasms, liver dysfunction, hemorrhoidal bleeding and portosystemic encephalopathy (1, 2). We describe two cases of CAPV presenting as pulmonary hyperten- sion, in which primary pulmonary hypertension was initially suspected. However, subsequent ultrasonogra-
phy and CT detected the absence of the portal vein and the presence of a portosystemic shunt. To the best of our knowledge, only three cases of pulmonary hypertension associated with CAPV have been reported since 1974 (3). Pulmonary hypertension is a recognized complica- tion of liver disease and portal hypertension. However, these two cases illustrate that CAPV may result in pul- monary hypertension without liver disease or portal hy- pertension and that CAPV can be diagnosed with nonin- vasive imaging techniques such as Doppler ultrasonog- raphy or CT angiography.
Case Report
Case 1
A 3-year-old girl presented with progressive dyspnea of several weeks duration. The medical history and physical examination were nonspecific. No hypoxemia was evident by arterial blood gas analysis (O2saturation:
Congenital Absence of the Portal Vein Presenting as Pulmonary Hypertension
1Suryoung Jun, M.D., Whal Lee, M.D., Ph.D., Jung-Eun Cheon, M.D., Ph.D., Woo-Sun Kim, M.D., Ph.D., In-One Kim, M.D., Ph.D., Kyung-Mo Yeon, M.D., Ph.D.
1Department of Radiology, Seoul National University Hospital Received July 18, 2007 ; Accepted September 21, 2007
Address reprint requests to : Whal Lee, M.D., Ph.D., Seoul National University College of Medicine, 28 Yongon-dong, Chongno-gu, Seoul 110- 744, Korea
Tel. 82-2-2072-0898 Fax. 82-2-743-6385 E-mail: [email protected]
Congenital absence of the portal vein (CAPV) is a rare malformation in which intesti- nal and splenic venous flow bypasses the liver and drains directly into the systemic circulation via a congenital portosystemic shunt. We describe two cases of CAPV pre- senting as pulmonary hypertension that were initially suspected as primary pul- monary hypertension. However, subsequent ultrasonography and CT detected the ab- sence of a portal vein and the presence of a portosystemic shunt. Pulmonary hyperten- sion is a recognized complication of liver disease and portal hypertension. However, these two cases illustrate that CAPV may result in pulmonary hypertension without liver disease or portal hypertension.
Index words :Portal vein
Portosystemic shunt Hypertension, pulmonary Angiography, CT
Liver
97.7%, PaO2: 79.9 mmHg, PaCO2: 39 mmHg, pH: 7.49).
The patient had anemia and thrombocytopenia (hemo- globin level: 10.8 g/dL, hematocrit: 34.9%, platelet count: 84×109/L), but biochemical parameters and the clotting profile were within normal ranges, except for a slightly elevated total serum bilirubin level (1.8 mg/dL).
Serological markers for hepatitis B and C viruses were negative. Chest radiography showed cardiomegaly and centroperipheral pulmonary vascular discrepancy sug- gestive of pulmonary hypertension (Fig. 1A).
Echocardiography revealed pulmonary hypertension with right ventricular enlargement and mild tricuspid regurgitation. Cardiac catheterization revealed a pul-
monary capillary wedge pressure of 9 mmHg, and pul- monary arterial pressure of 71/37 (mean 54) mmHg.
Pulmonary arteriography confirmed the absence of a pulmonary embolism, and no evidence of an intracar- diac or intrapulmonary shunt was seen by air-bubble contrast echocardiography or by cardiac catheterization.
Primary pulmonary hypertension was initially suspect- ed.
A C
B
Fig. 1. A 3-year-old girl presented with dyspnea.
A. Chest radiography showing cardiomegaly and centroperipheral pulmonary vascular discrepancy suggestive of pulmonary hy- pertension.
B. Arterial (a) and portal (b) phase axial images showing the absence of intrahepatic portal veins and a dilated hepatic artery (white arrow), and early inferior vena caval opacification (arrowhead) via a portosystemic shunt. Note the normal hepatic veins (yellow arrowheads).
C. A CT angiography volume rendered image showing the absence of a main portal vein. The superior mesenteric vein (SMV) and the splenic vein (SV) joined and drained through the inferior mesenteric vein (IMV) into the left internal iliac vein (yellow arrow- heads) and then into the inferior vena cava (asterisk).
a b
However, abdominal ultrasonography and CT angiog- raphy showed that the porta hepatis contained the com- mon bile duct and the common hepatic artery with no main portal vein. Intrahepatic portal veins were not seen, either. The common hepatic artery was found to be dilated (Fig. 1B). Furthermore, ultrasonography re- vealed a markedly enlarged mesenteric vein draining in- to the left internal iliac vein. There were no hepatic parenchymal lesions. Splenomegaly was also noted. CT angiography confirmed the absence of both intrahepatic and extrahepatic portal veins, and the superior mesen- teric vein and the splenic vein were found to be joined and to drain through the inferior mesenteric vein into the left internal iliac vein (Fig. 1C). These findings were compatible with CAPV, a type I-b portosystemic anom- aly as classified by Morgan et al. (4).
After a 19 month-follow-up under conservative man- agement, an approximately 3.5 cm sized hyperechoic hepatic mass was detected by ultrasonography. The mass appeared hyperintense on T2-weighted MR im- ages and mildly hyperintense on T1-weighted images.
Strong enhancement of the lesion was observed during the early arterial phase, but during the late portal and venous phases, the periphery of the lesion was slightly hypointense versus the liver parenchyma, whereas its center showed persistent enhancement, which was con- sidered to be due to a central scar (Fig. 1D). There was no evidence of chronic liver disease, and the level of al- pha-fetoprotein was not elevated (< 3ng/mL). Although not histologically confirmed, the hepatic mass was con- sidered a focal nodular hyperplasia, which is a relatively common complication of CAPV (2, 3).
The patient remains under conservative management.
Liver transplantation in this case is contraindicated due to the severe pulmonary hypertension (5, 6).
Case 2
A 20-year-old female presented with syncope, and complained of progressive dyspnea of several weeks du- ration. A physical examination showed no abnormali- ties, and arterial blood gas analysis indicated no hypox- emia (O2saturation: 98.9%, PaO2: 87.3 mmHg, PaCO2: D
Fig. 1. D. 19 months after a diagnosis of CAPV a 3.5 cm sized mass was detected in the right lobe of the liver. The mass was hyper- intense on T2-weighted MR images (a) and mildly hyperintense on T1-weighted images (b). Strong lesion enhancement was ob- served during the early arterial phase (c) and the lesion periphery was slightly hypointense versus the liver parenchyma during the venous phase (d). The lesion central portion which showed persistent enhancement (yellow arrow), was considered to be a central scar of a focal nodular hyperplasia.
a b
c d
33.6 mmHg, pH: 7.4). The patient had severe thrombo- cytopenia (platelet count: 5×109/L), the serum bilirubin level was elevated (total bilirubin: 5.6 mg/dL, direct bilirubin: 1.5 mg/dL), and the serum albumin level was slightly low (2.9 g/dL). Other biochemical parameters and the clotting profile were within normal ranges.
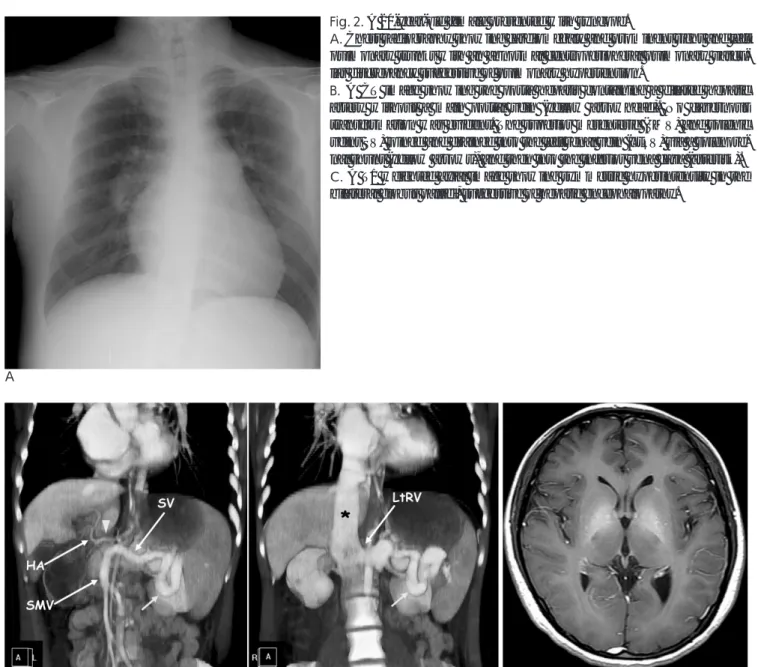
Chest radiography showed cardiomegaly and prominent right and left pulmonary trunks with an abnormal cen- troperipheral pulmonary vascular discrepancy sugges- tive of pulmonary hypertension (Fig. 2A). Echocardio- graphy revealed right ventricular enlargement and mild- ly reduced right ventricle contractility, accompanied by mild tricuspid regurgitation. The left ventricle was com- pressed by an enlarged right ventricle. Pulmonary arter- ial systolic pressure calculated from tricuspid regurgita-
tion velocity was 110 mmHg, and there was no evi- dence of an intracardiac or intrapulmonary shunt by air- bubble contrast echocardiography. There was no evi- dence of a pulmonary embolism on a lung ventilation/perfusion scan. Primary pulmonary hyper- tension was initially suspected.
However, abdominal ultrasonography showed the presence of no portal vein in the porta hepatis, and no intrahepatic portal vein. CT angiography confirmed these findings, and further revealed that the superior mesenteric and splenic veins joined and drained into the inferior vena cava via the left renal vein (Fig. 2B).
Marked splenomegaly was noted. The liver was not cir- rhotic as seen by ultrasonography and CT, and a brain MRI revealed symmetric T1 hyperintensity in the bilat-
B C
A
Fig. 2. A 20-year-old female presented with syncope.
A. Chest radiography showing cardiomegaly and prominent right and left pulmonary trunks with an abnormal centroperipheral pulmonary vascu- lar discrepancy suggestive of pulmonary hypertension.
B. A CT image showing the porta hepatis containing a dilated hepatic artery without a main portal vein (yellow arrowhead). No cavernous transformation was evident. The superior mesenteric (SMV) and splenic veins SV) joined and drained into the left renal vein (LtRV) via a splenore- nal shunt (yellow arrows), and then into the inferior vena cava (asterisk).
C. A T1 weighted axial image showing symmetric hyperintensity in the bilateral globus pallidi, suggestive of hepatic encephalopathy.
eral globus pallidi, suggestive of hepatic encephalopathy (Fig. 2C).
During conservative management of the severe pul- monary hypertension and thrombocytopenia, the pa- tient suddenly expired due to cardiac arrest on the fourth day of admission.
Discussion
During fetal development, abnormal involution of peri-intestinal vitelline venous loops can result in CAPV and extrahepatic portosystemic shunt formation (2, 4).
According to the case reports of liver biopsies in CAPV patients, histopathology displays portal tracts with nor- mal arteries and bile ducts but with severe loss of portal vein branches (1, 7). Since the intrahepatic branching of the developing portal vein is a prerequisite for the for- mation of intrahepatic bile ducts, it has been proposed that CAPV is not aplasia or agenesis of the portal vein, but it is caused by a secondary phenomenon such as the thrombotic occlusion of the extrahepatic portal vein dur- ing the prenatal period (1).
CAPV is classified into two types according to the ab- sence (type a) or presence (type b) of the confluent supe- rior mesenteric and splenic veins (4). Previously report- ed drainage sites of extrahepatic portosystemic shunts in CAPV vary, and have included the inferior vena cava (IVC), renal vein, iliac vein, inferior mesenteric vein, left hepatic vein, right atrium, and azygos vein (1-3).
Various anomalies including cardiac, skeletal, and vis- ceral anomalies have been reported in association with CAPV (1-3). Clinical presentations of CAPV are vari- ous, and CAPV can be entirely asymptomatic. Features suggestive of portosystemic shunt like hyperammone- mia, hypoalbuminemia, hypergalactosemia, mild liver function test abnormalities, and hepatic encephalopathy may exist, and patients can present with persistent jaun- dice and growth failure, mental retardation, and hemor- rhoidal bleeding (2, 3, 8).
CAPV is often associated with a benign or malignant hepatic neoplasm. Focal nodular hyperplasia is a rela- tively common complication of CAPV, and an adenoma, hepatoblastoma, or hepatocellular carcinoma may be present (2, 3, 8). These lesions might be caused by an ab- normal response of the liver cells to the lack of portal blood flow, increased arterial hepatic flow, and to the abnormal delivery of hepatotrophic factors (2, 3, 8).
In patients with liver disease and portal hypertension, the pulmonary vasculature is exposed to gut-derived
substances that bypass hepatic detoxification and enter the lungs through the portosystemic shunt (5). This is believed to provide the mechanism of two distinct pul- monary vasculopathies associated with liver disease and portal hypertension vasoconstriction and pulmonary ar- teriolar wall damage in portopulmonary hypertension and vasodilatation and arteriovenous shunting in he- patopulmonary syndrome (HPS) (5). In CAPV, enteric venous flow completely bypasses the liver and enters the pulmonary circulation without liver disease or por- tal hypertension (5, 7). Three cases of pulmonary hyper- tension and five cases of HPS in association with CAPV have been reported since 1997 (3, 7).
In a recent study on liver transplantation in CAPV pa- tients, it was suggested that prophylactic liver transplan- tation be conducted in CAPV patients before fatal pul- monary hypertension or HPS develops, as this might complicate or preclude liver transplantation (6). Thus, it is important to first detect the absence of the portal vein and the presence of a portosystemic shunt by imaging studies, regardless of the clinical presentation.
We have described two cases of CAPV that presented as pulmonary hypertension without severe liver dys- function or portal hypertension. Both cases were initial- ly diagnosed as having primary pulmonary hyperten- sion, but abdominal ultrasonography and CT angiogra- phy lead to the identification of pulmonary hyperten- sion, and a diagnosis of CAPV. Anatomical loss of the portal vein accompanied by abnormal venous drainage of the supramesenteric and splenic veins is required for a definite diagnosis of CAPV (9). CT angiography and MR angiography have been proven as reliable and non- invasive diagnostic techniques for imaging the portal system, as in our cases (2, 8, 9). These two cases may be differentiated from acquired portal vein thrombosis by the absence of cavernous transformation of the peripor- tal collateral veins or the absence of other secondary signs of portal hypertension, such as varices and ascites (3).
We conclude that it is important to investigate the pos- sibility of a portosystemic shunt in cases considered as primary pulmonary hypertension, even in the absence of symptoms and signs suggesting liver disease or portal hypertension. Although clinical presentations of CAPV are various, the imaging characteristics of CAPV, i.e., the absence of a portal vein and the presence of a por- tosystemic shunt can be detected precisely by ultra- sonography, CT angiography, or MR angiography re- gardless of clinical presentation. The resulting early non-
invasive diagnosis allows appropriate treatment to be initiated before the development of fatal pulmonary hy- pertension or HPS, which might complicate or preclude liver transplantation.
References
1. Appel H, Loddenkemper C, Schirmacher P, Dienes HP, Sieper J, Rudwaleit M, et al. Congenital absence of the portal vein with splenomegaly and hypersplenism in a young woman. Digestion 2003;67:105-110
2. Niwa T, Aida N, Tachibana K, Shinkai M, Ohhama Y, Fujita K, et al. Congenital absence of the portal vein: clinical and radiologic findings. J Comput Assist Tomogr 2002;26:681-686
3. De Gaetano AM, Gui B, Macis G, Manfredi R, Di Stasi C.
Congenital absence of the portal vein associated with focal nodular hyperplasia in the liver in an adult woman: imaging and review of
the literature. Abdom Imaging 2004;29:455-459
4. Morgan G, Superina R. Congenital absence of the portal vein: two cases and a proposed classification system for portasystemic vas- cular anomalies. J Pediatr Surg 1994;29:1239-1241
5. Halank M, Ewert R, Seyfarth HJ, Hoeffken G. Portopulmonary hypertension. J Gastroenterol 2006;41:837-847
6. Soejima Y, Taguchi T, Ogita K, Taketomi A, Yoshizumi T, Uchiyama H, et al. Auxiliary partial orthotopic living donor liver transplantation for a child with congenital absence of the portal vein. Liver Transpl 2006;12:845-849
7. Cheung KM, Lee CY, Wong CT, Chan AK. Congenital absence of portal vein presenting as hepatopulmonary syndrome. J Paediatr Child Health 2005;41:72-75
8. Turkbey B, Karcaaltincaba M, Demir H, Akcoren Z, Yuce A, Haliloglu M. Multiple hyperplastic nodules in the liver with con- genital absence of portal vein: MRI findings. Pediatr Radiol 2006;36:445-448
9. Takagaki K, Kodaira M, Kuriyama S, Isogai Y, Nogaki A, Ichikawa N, et al. Congenital absence of the portal vein complicating hepatic tumors. Intern Med 2004;43:194-198
대한영상의학회지 2007;57:423-428
폐동맥 고혈압으로 발현한 선천성 간문맥 형성부전의 증례 보고1
1서울대학교병원 영상의학과
전수령・이 활・천정은・김우선・김인원・연경모
선천성 간문맥형성부전은 문맥혈류가 간을 우회하여 문맥-체정맥 단락을통해 대정맥으로 직접 배출되는 드문 기 형이다. 저자들은 일차성 폐동맥고혈압으로 진단되었다가 초음파 및 전산화단층촬영을 통해 문맥의 형성부전 및 선 천성 문맥-체정맥 단락을 비침습적으로 발견해 냄으로써, 이로 인한 이차성 폐동맥 고혈압이 발생하였음을 밝힐 수 있었던 증례를 2예 보고하고자 한다.