Comparisons of Unicortical and Bicortical Lateral Mass Screws in the Cervical Spine:Safety vs Strength*
Choon-Keun Park, M.D., 1) Jang-Hoe Hwang, M.D., 2) Chul Ji, M.D., 1) Jae Un Lee, M.D., 1) Jae Hoon Sung, M.D., 1) Seung-Jin Choi, M.D., 1) Sang-Won Lee, M.D., 1) Eric Seybold, M.D., 3) Sung-Chan Park, M.D., 1) Kyung-Suok Cho, M.D., 1) Chun-Kun Park, M.D., 1) Joon-Ki Kang, M.D. 1) Department of Neurosurgery,
1)Medical College, The Catholic University of Korea, Suwon, Korea
Department of Neurosurgery,
2)Hallym University College of Medicine, Choonchun, Korea Department of Orthopedic Surgery,
3)State University of New York, New York, USA
= =
= = Abstract = = = =
경추부의 후관절 나사못 고정술에서 단피질삽입법과 양피질 삽입법 간의 특성에 관한 비교
가톨릭대학교 의과대학 성빈센트병원 신경외과학교실,
1)한림대학교 의과대학 신경외과학교실
2)Department of Orthopedic Surgery,
3)State University of New York, New York
박춘근1)
·황장회2)
·지 철1)
·이재언1)
·성재훈1)
·최승진1)
이상원
1)
·Eric Seybold3)
·박성찬1)
·조경석1)
·박춘근1)
·강준기1)
ntroduction:The purpose of this study was to analyze the safety, pullout strength and radiographic characteristics of unicortical and bicortical screws of cervical facet within cadaveric specimens and evaluate the influence of level of training on the positioning of these screws.
Methods:Twenty-one cadavers, mean 78.9 years of age, underwent bilateral placement of 3.5mm AO lateral mass screw from C3-C6(n=168) using a slight variation of the Magerl technique. Intraoperative imaging was not used. The right side(unicortical) utilized only 14mm screws(effective length of 11mm) while on the left side to determine the length of the screw after the ventral cortex had been drilled. Three spine surgeons(attending, fellow, chief resident) with varying levels of spine training performed the procedure on seven cadavers each. All spines were harvested and lateral radiographs were taken. Individual cervical vertebrae were carefully dissected and then axial radiographs were taken. The screws were evaluated clinically and radiographically for their safety. Screws were graded clinically for their safety with respect to the spinal cord, facet joint, nerve root and vertebral artery. The grades consisted of the following categories:“satisfactory”, “at risk” and “direct injury”. Each screw was also graded according to its zone placement. Screw position was quantified by measuring a sagittal angle from the lateral radio- graph and an axial angle from the axial radiograph. Pull-out force was determined for all screws using a material testing machine.
Results:Dissection revealed that fifteen screws on the left side actually had only unicortical and not bicortical purchase as intended. The majority of screws(92.8%) were satisfactory in terms of safety. There were no injuries to the spinal cord. On the right side(unicortical), 98.9% of the screws were “satisfactory” and on the left side(bicor- tical) 68.1% were “satisfactory”. There was a 5.8% incidence of direct arterial injury and a 17.4% incidence of direct nerve root injury with the bicortical screws. There were no “direct injuries” with the unicortical screws for the nerve root or vertebral artery. The unicortical screws had a 21.4% incidence of direct injury of the facet joint, while the bicortical screws had a 21.7% incidence. The majority of “direct injury” of bicortical screws were placed by the surgeon with the least experience. The performance of the resident surgeon was significantly different from the
IIII
*본 논문은 보건 복지부 00-CN-01-0003의 연구비와 가톨릭 중앙 의료원 연구비의 일부로 이루어졌음.
attending or fellow(p<0.05) in terms of safety of the nerve root and vertebral artery. The attending’s performance was significantly better than the resident or fellow(p<0.05) in terms of safety of the facet joint.
There was no relationship between the safety of a screw and its zone placement. The axial deviation angle mea- sured 23.5±6.6 degrees and 19.8±7.9 degrees for the unicortical and bicortical screws, respectively. The resident surgeon had a significantly lower angle than the attending or fellow(p<0.05). The sagittal angle measured 66.3±7.0 degrees and 62.3±7.9 degrees for the unicortical and bicortical screws, respectively. The attending had a significantly lower sagittal angle than the fellow or resident(p<0.05).
Thirty-three screws that entered the facet joint were tested for pull-out strength but excluded from the data because they were not lateral mass screws per-se and had deviated substantially from the intended final trajectory.
The mean pull-out force for all screws was 542.9±296.6N. There was no statistically significant difference between the pull-out force for unicortical(519.9±286.9N) and bicortical(565.2±306N) screws. There was no significant difference in pull-out strengths with respect to zone placement.
Conclusion:It is our belief that the risk associated with bicortical purchase mandates formal spine training if it is to be done safely and accurately. Unicortical screws are safer regardless of level of training. It is apparent that 14mm lateral mass screws placed in a supero-lateral trajectory in the adult cervical spine provide an equivalent strength with a much lower risk of injury than the longer bicortical screws placed in a similar orientation.
KEY WORDS:Unicortical・Bicortical・Lateral mass screw・Strength・Safety.
Introduction
Posterior cervical spine fusion has a long history of cli- nical utility in the treatment of traumatic and degenerative instability. The first spinous wiring was reported by Hadra in 1891. Rogers
20)popularized the use of spinous process wires and bone graft for the treatment of fracture disloca- tions. The triple-wire technique, as reported by McAfee, et al, has yielded good clinical results. Lateral mass plating, as first introduced by Roy-Camille, provides immediate fracture stability and rotational control
13)21)22). The safe pla- cement of the screws in this procedure remains a concern.
The stability of the cervical spine plating system is dependent on a number of factors, One of which is the interface strength between bone and screw. Heller, et al
11)have examined the pullout strength of unicortical versus bicortical purchase, and bicortical screw pullout force was twenty percent higher than unicortical screw pullout force.
Other investigators have analyzed the biomechanical and safety characteristics of different screw depths and trajecto- ries
1-4)8)9)11)13)15-17)19)23)24). These reports vary in the relative morbidity and technical difficulty of lateral mass plating.
The challenge to the surgeon is balancing what is safe versus what is biomechanically sound.
Recently, Wellman, et al
25)reported on the clinical outcome of forty-three patients treated with lateral mass plating and
found a zero incidence of screw related complication. There was “no attempt to achieve bicortical purchase” and the surgeons “sacrificed bicortical purchase rather than risk ex- tending the screw out of the far cortex.” Screw lengths of only 14-16mm were used. Graham, et al
9)found no incid- ence of cord or vertebral artery injury and a 1.8% per-screw risk of radiculopathy in a prospective study of twenty-one patients treated with lateral mass screw and plate fixation systems. All three radiculopathies that occurred were “a direct result of performing bicortical screw purchase”. They recommended that clinical studies of the “safety and efficacy of unicortical compared to bicortical screw purchase be done prior to any final recommendations being made about their clinical safety”.
The purpose of the current study was to analyze the safety, pullout strength, and radiographic characteristics of unicor- tical and bicortical screws placed in cadaveric spines and to evaluate the influence of level of training on the positioning of these screws.
Methods
Twenty-one formalin-preserved cadavers were used. El-
even male and ten female specimens were divided equally
among three spine surgeons with differing levels of experi-
ence. Group one consisted of seven cadavers in which the
procedure was performed by an attending physician who
had completed one year of spine fellowship training. Group two consisted of seven cadavers in which the procedure was allocated to the spine fellow in his 5th month of fellowship.
Group three consisted of seven cadavers in which the lateral mass screws were placed by a chief resident who had been instructed in the technique but who had never actually per- formed the procedure before this study:All surgeons were right-hand dominant.
The mean age of the specimens in the study was se- venty-eight years(range, fifty-seven to ninety-six years).
The mean specimen age in group one was eighty-one years, in group two, seventy-five years and in group three, eighty- two years. The cadaver age were not significantly different among the three groups.
Each cadaver was positioned prone, and the cervical spine was dissected as in posterior cervical spine surgery. Lateral mass screws(Synthes, Paoli, PA) were placed at C3, C4, C5, and C6 bilaterally. These were 3.5mm nonself-tapping cortical screws.
1. Screw placement
The technique chosen for screw trajectory was patterned as follows. The mid sagittal and mid axial apex of the lateral mass was identified. The drill bit was placed at this apex and then leaned against the spinous process of the vertebra below the level of drilling. This provided both lateral and superior angulation of the screw. Radiographic imaging was not used during placement of the screws.
On the right side, the drill guide was set to 14mm depth, and only 14mm screws were placed. No attempt was made at bicortical purchase. Screws placed on the right side were assumed to be unicortical. On the left side, the drill guide was not set, and a depth gauge was used to determine the length of the screw after the ventral cortex had been drilled.
The screws placed on the left side were assumed to be bicortical. All screw holes were tapped according to manu- facturer’s recommendations. All screws were then seated through the recessed screw hole in a precut lateral mass plate, to closely simulate the actual depth of the screw insertion in the clinical setting.
In the Synthes screw, 14mm is the measurement from the tip of the screw head to the shaft. The length of the shaft of a 14-mm screw is 12mm. The thickness of the screw hole in the plate is 1mm. Therefore, a 14-mm screw was inserted to a depth of approximately 11mm. This was designated as the “effective length” of the screw.
Each of the three surgeons placed fifty-six screws, a total count of one hundred sixty-eight. Each specimen was identified by surgeon and whether it was the first or last specimen operated on by the surgeon. No radiographic feed- back was provided to the surgeon between the first and last specimens.
2. Safety evaluation
After screw placement, all spines were harvested and scored in a blinded fashion by the three surgeons and an attending neurosurgeon who was not involved in screw placement. All screws were reviewed by the entire group for a consensus rating. Screws placement was rated as
“satisfactory”, “at risk” or “direct injury”. A screw was considered satisfactory if it did not injure any of the afore- mentioned structures and was directed so that its trajectory posed no risk. A screw was considered at risk if it did not directly injure a structure, but if it had been longer(i.e. 2- 3mm), its trajectory would have caused direct injury to a surrounding structure(i.e., a unicortical or bicortical screw aimed at the transverse foramen). A screw was defined as
“direct injury” if it directly violated the aforementioned structures. Bicortical purchase was defined as protrusion of the tip of the screw far enough beyond the anterior cortex that the second cortex was fully engaged.
A lateral radiograph was taken of the specimens before disarticulation of the individual levels. The left sided(bi- cortical) screws were tagged with a radiopaque marker.
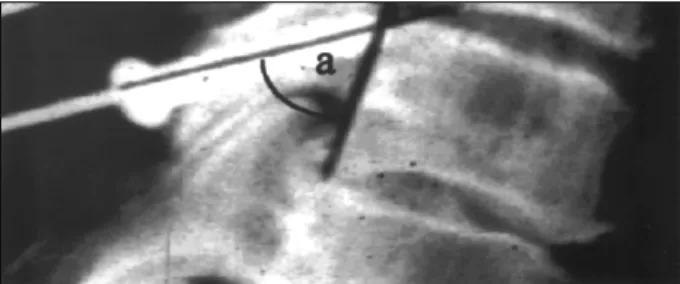
The sagittal angle and zone position of each screw was recorded. The sagittal angle was measured between a line parallel to the posterior vertebral body and a line parallel to the screw(Fig. 1). The zones for the tip of the screw are defined by Heller, et al as follows:Zone 1 is the superior margin of the superior articular process, Zone 2 includes the ventral portion of the lateral mass that forms the roof of the neuroforamen and the transverse process that protect
Fig. 1. A lateral radiograph of the specimen showing how the
saggittal angle (a) is measured. The higher the angle, the more
horizontal the screw.
the nerve root as it exits the neuroforamen, and Zone 3 extends from the inferior origin of the transverse process to the tip of the inferior articular process(Fig. 2).
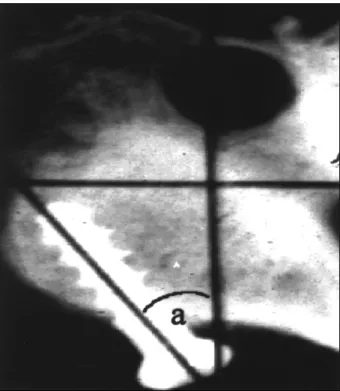
The nerve root, spinal cord, vertebral artery, facet joint, and depth of the screw(unicortical vs. bicortical) were assessed by all surgeons. Each specimen was disarticulated into four distinct cervical levels and then again reviewed by all surgeons for depth of penetration and nearness to surrounding structures, as before. A radiograph was taken of each cervical level in the axial fashion. The axial de- viation of the screw in each specimen was measured by 2
surgeons(ES, JB) in a technique shown in Fig. 3. The axial radiographs were reviewed to determine whether any screw posed a risk to the vertebral artery foramen was visible radiographically but was not seen on visual inspection of the specimen. All(12/12) screws that were radiographically at risk for the artery were previously assigned an at risk rating during the visual inspection of the specimen before the radiographic imaging. Interobserver reliability was ass- essed using ten axial angel measurements and 3 indepen- dent observers. Ninety percent of the measured angle were within 1 of another, and 100% were within 2 of another.
The interobserver measuring error for this study was 1.1.
3. Pull-out testing
A materials testing machine(Instron Canton, MA) was used to determine the pullout force of the lateral mass screws.
Each vertebral body was embedded in potting material and held in a three-way vise. The long axis of the screw was aligned with the actuator of the materials testing machine.
The head of the screw was held with a surgical screw holder and was prevented from splaying with a cylin-drical washer. A tensile force was recorded using a constant rate of displacement of 2mm/min. Load and displacement data were collected by a computer. A sharp decline in the load- displacement curve signified peak pullout load. Statistical analysis was performed using commercial software(Stat- View;Abacus Concepts, Berkeley, CA). Tests were per- formed for safety and zone placement data, and analysis of variance was performed on pull-out data and radiograph angle measurements. Significance was deemed at the 95%
confidence limit(p<0.05).
Results
1. Safety
The majority(Table 1, 2) of the screws were placed in a safe position(92.8% rated satisfactory). All screws were satisfactory in proximity to the spinal cord. One the right side, where only 14-mm screws were placed and no attempt was made for bicortical purchase, 98.9%(83/84) of the screws were satisfactory. On the left side, where screws 14mm or greater were used for bicortical purchase, only 75%(61/84) were satisfactory. Excluding the fifteen screws that were not truly bicortical on the left side, only 68.1%(47/69) were truly satisfactory.
Fig. 2. The three zones of the lateral mass as defined by Heller et al.
Fig. 3. An axial radiograph indicating how the axial deviation angle (a) is measured.
Zone
1 2 3
1)))) Attempt at unicortical screws purchase
All eighty-four screws placed on the right side of the cadaveric spines were 14mm in length, regardless of the size of the specimen. This approximates an effective length of 11-12mm. Nine of these screws(10.7%) were actually bicortical. There was no incidence of direct injury to artery or nerve root. Only one screw(1/84) was considered to place the nerve root at risk(placed by the fellow) and none placed the vertebral artery at risk. The screw advancing on the nerve root was actually a bicortical screw that was intended to be unicortical. The incidence of facet joint violation was 21.4%. Facet joint penetration is important, at the most caudal end of the fusion, because inadvertent extension of the fusion may occur. Facet violation has little impact on the actual safety of a screw. Therefore, for future reference in this article, “unsafe” describes only those screws involving the artery or the nerve and not the facet joint.
2)))) Attempt at bicortical screws purchase
On the left side, 68.1% of the screws were satisfactory.
This was significantly different from the unicortical side
(p<0.05). Although they were all intended to be bicortical, dissection showed that fifteen(17.8%) of the eighty-four screws were actually unicortical. An almost equal number of these were placed by the resident and attending surgeon.
All the fellow’s screws were bicortical. Because the total number of screws with bicortical purchase decreased to sixty-nine, the actual incidence of unsafe bicortical screws increased to 31.9%. There were no injuries to the cord. The vertebral artery sustained a direct injury(compression of the artery) four times(4/69;5.8%). These were all placed by the resident surgeon. Eleven(16%) of the sixty-nine screws were considered to place the artery at risk. Here again, ten of the eleven at risk screws were placed by the least experienced surgeon and one by the fellow. The inci- dence of direct injury to the nerve root was 17.4%(12/69).
The majority of these(9/12) were placed by the resident, 3 by the fellow, and none by the attending surgeon. Ten of the screws were considered to place the nerve root at risk.
Here again, all but one was placed by the resident surgeon.
The performance of the resident surgeon was significantly different from that of the fellow or attending surgeons(p<
0.05). There was no significant difference between the performances of the fellow and attending surgeons. The incidence of facet joint injury(17.8%;15/84) was not sig- nificantly different from that of the right side. However, the attending surgeons performance in avoiding the facet joint was significantly better than of the resident or fellow(p<
0.05). No significant difference was found in safety score between the first and last specimens in Groups I, II, and III.
2. Radiographs
The mean axial deviation angle for the entire study was 21.6±7.5 degree. The right side measured 23.5±6.6 degree, and the left side measured 19.8±7.9 degree. All surgeons were right-hand dominant. The deviation angle was not significantly different by vertebral level. It was different, however, by surgical experience. The resident surgeon had a significantly lower axial deviation angle(17.5±8.9 deg- ree) than the other two surgeons(p<0.05). The unsafe screw in this study(direct injury or root or nerve at risk) had sig- nificantly lower axial deviation angles(13.6±8.5 degree and 16.6±5.4 degree, respectively) than the satisfactory screws (22.7±7.5 degree;p<0.05). There was no significant di- fference in axial deviation angle between screws that did and did not penetrate the facet joint.
The sagittal angle was also analyzed. A higher sagittal
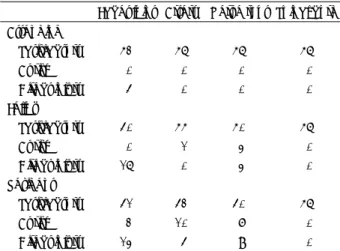
Table 1. Safety vs. side Facet
joint Artery Nerve root
Spinal cord Left side(bicortical)
Satisfactory 68 69 61 84
At risk 1 11 11 0
Direct injury 15 4 12 0 Right side(unicortical)
Satisfactory 65 84 83 84 At risk 1 0 1 0 Direct injury 18 0 0 0
Table 2. Safety vs. surgeon
Facet joint Artery Nerve root Spinal cord
Attending
Satisfactory 52 56 56 56 At risk 0 0 0 0 Direct injury 4 0 0 0 Fellow
Satisfactory 40 55 50 56 At risk 0 1 3 0 Direct injury 16 0 3 0
Resident
Satisfactory 41 42 40 56
At risk 2 10 7 0
Direct injury 13 4 9 0
angle was correlates to a screw inserted in a more caudad direction and a lower sagittal angle was equates to a screw inserted in a more cephalad direction. The mean sagittal angle was 64.3±7.6 degree for the entire study. There was no significant difference between left and right sides or different vertebral levels. There was a significant differ- ence among surgeons in mean sagittal angles. The screws inserted by attending surgeon had the lowest angle(61.3±
7.1 degree) and were thus the closest to the vertical plane, whereas those inserted by the resident surgeon had the highest angle(67.2±9.1 degree) and were thus the closest to the horizontal plane(p<0.05). The screws that injured the roots were directed more cephalad(60.±6.9 degree) than the safe screws(64.8±7.4 degree). The screws that injured the artery were directed more caudad(72.5±13.7 degree) than the satisfactory screws(p<0.05). There was no significant difference for screws at risk. Screws that entered the facet joint were directed more caudad(68.9±
7.6 degree) than screws that did not enter the facet joint (63.1±7.3 degree, p<0.05).
Zone placement for the tip of the screw was analyzed. The most frequent zone placement occurred in zone 3(51.8%), followed by zone 2(33.9%) and Zone 1(14.3%). There was no significant difference found between satisfactory and unsafe screws and their respective zone placements.
Most facet penetrations occurred in zone 3. This was not significantly different, however. There was also no differ- ence in zone predilection among the different vertebral le- vels, between the left or right side, or according to surgical experience.
3. Pullout data
All thirty-three screws that entered the facet joint were tested for pullout strength but were excluded in the data calculation because they were not lateral mass screws per se and had deviated substantially from the intended final trajectory. The mean pullout force for all screws was 542.9
±296.6N. The maximum recorded was 1277.7N(non facet screw) and the minimum was 16.7N. Although the mean pullout force was higher for the bicortical screws, there was no statistically significant difference between the right (unicortical) side(519.9±286.9N) and the left(bicortical) side(565.2±306N)(p=0.378). Because some screws on the left were not truly bicortical and some screws on the right were, pullout strength was analyzed regardless of side and whether they were unicortical or bicortical. Interest-
ingly, the unicortical values were higher(560.6±277.5N vs. 522.9±317N), but the differences were not statistically significant.
The pullout values as a whole were higher for C3 and C4(580.6±283.4N) compared with C5 and C6(496.3±
388.2N). This was not significant. The mean pullout str- ength for all screws placed by the fellow surgeon was the highest(628.5±286N) for and those placed by the attending surgeon were lowest(445.9±233.6N). The difference was not significant, however. There was no statistically signifi- cant difference in pullout strengths between the different zones, even though zone 1 screws on the right(210±
180.9N) were markedly weaker than zone 3 screws on the right(600.3±277.8). The actual number of screws in Zone 1 was too small for statistical power. The overall pullout strengths for the female specimens was 503.4±263.2N and that for the males was 572.9±318N(p=0.18, not significant).
A separate analysis of variance linear regression was cal- culated for pullout strength versus age. The R2 value was 0.133, indicating no correlation between age and pullout strength.
Discussion
A decade has passed since some of the first reports of examination of biomechanical and clinical experiences with cervical lateral mass plating systems
1-4)8)9)11)13)15-17)19)23)24). Montesano, et al
16)and Errico, et al compared the failure properties of lateral mass plating using the Magerl and Roy-Camille screw trajectories. They found the Magerl technique to be biomechanically superior. In Montesano, et al the failure load for the Magerl technique was 585N and that for the Roy-Camille technique was only 152N. In Er- rico, et al the mean screw pullout force for 3.5mm screws placed by the Magerl technique was also significantly higher than those placed by the Roy-Camille technique (607121N vs. 471108N). Both groups emphasized the sa- fety of the Magerl technique, because screws are directed away from the neurovascular structures, there is a lower likelihood of injuring facets, especially at the caudal aspect of the fusion. In a comprehensive study comparing the Magerl and Roy-Camille techniques for screw placement, Heller concluded that the Magerl technique had a higher risk of nerve root injury(7.3% vs. 0.8%) but a lower risk of facet violation than the Roy-Camille method(2.4% vs.
22.5%).
The original technique described by Magerl and Seemann recommended drilling at an angle of 25 laterally and 40- 60 superiorly to parallel the facet joint
26). Using a cadaveric model, An, et al
2)determined that a less lateral and more cephalad screw trajectory had greater risk of nerve root injury. They recommended a screw trajectory of 15-18 in the superior direction and 30-33 in the lateral direction.
In a retrospective report of 30 consecutive patients with cervical spine injuries treated with lateral mass fixation, Anderson, et al reported no major complications and a 100% fusion rate using the lateral mass plating technique.
Heller, et al
10)concluded that the actual risk of screw inser- tion was much less than that predicted in vitro. They found a 0.6% incidence of nerve root injury and zero incidence of artery injury. Fehlings and Cooper
8)reported on forty-four patients who undergoing lateral mass plating and found that only three required revision surgery for screw-plate failure. Most recently, Martin, et al
14)reported on 191 pati- ents with lateral mass plating and showed a 0.1% incidence of nerve root injury and a 100% fusion rate.
In the current study issues of safety and efficacy, which have been raised by some surgeons, were examined with unicortical and bicortical screw purchase
9)25). Heller, et al
11)determined that bicortical purchase increased pullout resis- tance from a load to failure of 272N to a load of 350N.
They suggest that it “remained to be determined whether this amount of enhanced purchase justifies the theoretical risk of morbidity associated with penetration of the second cortex”. The results of the current study included several important points. No statistically significant difference in pullout strength was found between unicortical and bicor- tical screws. There were no injuries with either unicortical or bicortical 14-mm screws, even when their paths inadver- tently deviated from the planned trajectory.
Theoretically bicortical screw should have higher pullout strength. However in our study no statistically significant difference in pullout strength was found between unicor- tical and bicortical screws. This difference was thought to be caused by both inconsistent placement of screws and smallness of the facet size. This means correct placement of screws is clinically more important than bicortical pla- cement.
Approximately 10% of our screws were incorrectly placed according to the number of cortices they were supposed to penetrate. This occurred at all levels of training and indi- cates that it is not always possible to accurately feel with
the drill bit or depth gauge the far cortex of the lateral mass.
This can have profound clinical consequences when choo- sing between a 16 or 18mm screw if bicortical purchase is sought and indicates that measuring screw depth has inaccuracies that may be an inherent part of this procedure.
An attempt should be made to minimize this risk by choos- ing a screw length(i.e. 14mm) that is both safe and effective.
The results of this study also indicate that the level of spine training plays a direct role in determining the clinical safety of placing lateral mass screws through both cortices.
There is a direct correlation between the level of training and the incidence of injury. All of these injuries were from screws more than 14mm in length. It is the authors belief that the risk associated with bicortical purchase mandates formal spine training if it is to be performed safely and accurately. Unicortical screws are safer, regardless of level of training.
The effective length of the screw in the bone varies among fixation system. For instance, anterior oblique system, a 14-mm screw has a shaft length of 12mm and once inserted through the plate, the effective length in the bone was reduced to 11mm. Jonsson and Rausching
12)studied several lateral mass plating systems to determine the effective length of specifically designated screw lengths in cadaveric spines.
They found that a 20mm anterior oblique screw has an effective length of 16-17mm. They also found that no screw of 11mm effective length introduced perpendicular to the plate comes close to the segmental nerve. This corresponds to a 14-mm screw. One half of the screws with effective length of 13mm(16mm screw) “penetrated the anterior cor- tex of the articular pillar and encroached on the nerve and ganglion”.
They also thought it “unnecessary to transgress the an- terolateral cortex” when using the Magerl technique. Ebra- heim et al. measured the distance between the lateral mass and the vertebral foramen and found that as the surgeon moves caudad from C3 to C6, the distance from the post- erior border of the vertebral artery foramen to the posterior border of the lateral mass gradual increased. Distances ran- ged from 12.3mm at C3 to 133.6mm at C6. It is apparent that a 14mm screw with an effective length of 11mm should usually be safe, regardless of the slight variations with desired trajectory.
Most screws placed in the current study were in the lower
zone and pedicle zone(Zone 2 and Zone 3). Regardless of
the number of cortices penetrated, these lower-zone screws
were not found to be at increased risk of causing nerve injury compared with the screws in Zone 1. In fact, the screws that injured the nerve roots were placed in a more cephalad direction. This is in contradistinction to the work by Ebraheim, et al
5)6)and Xu, et al
27)who found that the upper zone(Zone 1) was the safest zone.
Ebraheim, et al
7)also determined that an average lateral deviation of more than six degrees should be safe enough to avoid the lateral limit of the vertebral artery foramen.
Their data indicates that there is no risk of damaging the vertebral artery if a screw is directed ten degrees lateral to the sagittal plane. The current investigators have also exa- mined these angels and determined that there is a clear association between unsafe screws and absence of lateral deviation. Lateral angulation is perhaps more important than the sagittal angel(Zone placement). Unfortunately, lateral angulation cannot be accurately assessed during or after surgery without an axial computed tomography scan. The routine use of intraoperative or postoperative lateral radio- graphs to assess screw safety is of marginal value.
The issue of fresh frozen versus embalmed bone should be addressed in connection with the pullout testing. Various factors affect the pull-out strength of screws in bone
26). Pelker, et al has shown that the compressive properties of freeze-dried vertebrae do not differ significantly from that frozen vertebrae. The next question, therefore, is to what extent the embalming process adversely affect the mecha- nical properties of bone and thus the pullout strength of the screws. There is little in the literature regarding this topic.
McElhaney, et al have shown that the embalming process tends to decrease the compressive strength of bone, but not the tensile strength. Additionally, specimens in the current study, on average, had screw pullout values equivalent to, or higher than, previously published values
11)16). The current specimens were not wet at the time of screw pullout testing.
It is unknown whether the drying process that occurred during the dissection and radiographic measurement played a role in returning the stiffness of the bone to its pre- embalmed level. Further investigation is needed comparing results obtained with wet embalmed specimens with those obtained with dried em-balmed specimens before further conclusions can be drawn.
Conclusion
Several questions posed by investigators during the past
few years were addressed in the current study. Although pedicle screws placed in the cervical spine provide greater stability than lateral mass screws, the inherent neurova- scular risk associated with pedicle screw placement is quite high. In the authors opinion, lateral mass screws with an effective length of 11mm, placed in a superolateral-lateral trajectory in the adult cervical spine, provide an equivalent pull-out strength with a much lower risk of injury than the longer bicortical screws placed in a similar orientation.
Additionally, when intraoperative imaging is not used, the accurate and safe placement of these screws is significantly improved with experience and focused educational training in the technique.
•
논문접수일:2001년 7월 2일•
심사완료일:2001년 8월 27일•
책임저자:이 상 원442-060 경기도 수원시 팔달구 지동 93
가톨릭대학교 의과대학 성빈센트병원 신경외과학교실 전화:031) 249-7193, 전송:031) 245-5208 E-mail:[email protected]
References
1) Abumi K, Itoh H, Tanejchi H, Kaneda K:Transpedicular
screw fixation for traumatic lesions of the middle and lower cervical spine : Description of the techniques and preliminary report. J Spinal Disorders 7 : 19-28, 1994
2) An H, Gordin R, Renner K:Anatomic considerations for
plate-Screw fixation of the cervical spine. Spine 16 ( Suppl ):
S548-51, 1991
3) Choueka J, Spivak J, Kummer F, Stegr T:Flexion failure of
posterior lateral mass screws. Spine 21 : 462-468, 1996
4) Cooper PR, Cohen A, Rosiello A, Koslow M:Posterior sta-bilization of cervical spine fractures and subluxations using plates and screws. Neurosurgery 23 : 300-306, 1988
5) Ebrahim N, Tremain M, Xu R, Yeasting R:Lateral radiologic
evaluation of lateral mass screw placement in the cervical spine.
Spine 23 : 458-462, 1998
6) Ebraheim N, Xu R, Challgren E, Yeasting R:Quantitative
anatomy of the cervical facet and the posterior projection of its inferior facet. J Spinal Disord 10 : 308-316, 1997
7) Ebraheim N, Xu R, Yeasting R:The location of the vertebralartery foramen and its relation to posterior lateral mass screw fixation. Spine 21 : 1291-1295, 1996
8) Fehlings MG, Cooper PR:Posterior plates in the manage-
ment of cervical instability : Long-term results in 44 patients.
J Neurosurg 81 : 341-349, 1994
9) Graham A, Swank M, Kinard R, Lowrey G, Dials B:Poste-
rior cervical arthrodesis and stabilization with a lateral mass
plate. Spine 21 : 323-329, 1996
10) Heller J, Silcox H, Sutterlin C:Complications of Posterior
Cervical Plating. Spine 20 : 2442-2448, 1995
11) Heller J, Estes B, Zaouli M, Flier R, Diop A:Biomechanical
study of screws in the lateral masses : variables affecting pu- llout resistance. J Bone Joint Surg[Am] 78 : 1315-1321, 1999
12) Jonsson H, Raushning W:Anatomical and morphometric st-udies in posterior cervical spinal screw-plate systems. J Spinal Disord 5 : 429-438, 1994
13) Levine A, Mazel C, Roy-Camille R:Management of fracture
separation of the articular masses using posterior cervical plating. Spine 17 ( Suppl ): S447-454, 1992
14) Martin GJ Jr, Haid RW, Rodts GF, Woodard EJ, Alexander J:Posterior plating in the cervical and thoracic spine, prese-
nted at the 25th annual meeting of the Cervical Spine Research Society, Rancho Mirage, California, December, 1997, pp4-6
15) Miller R, Ebraheim N, Xu R, Yeasting R:Anatomic conside-ration of transpedicular screw placement in the cervical spine.
Spine 21 : 2317-2322, 1996
16) Montesano P, Juach E, Anderson P, Benson D, Hanson P:
Biomechanics of cervical spine internal fixation. Spine 16 ( Su- ppl ): S10-16, 1991
17) Pait G, McAllister P, Kaufman H:Quadrant anatomy of the
articular pillars of the cervical spine. J Neurosurgery 82 : 1011-1014, 1995
18) Panjabi M, Durnceau J, Goel V, Oxland T, Tadata K:Cervical
Human Vertebrae : Quantitative three-dimensional anatomy of the middle and lower regions. Spine 16 : 861-869, 1991
19) Perin N, Cooper P:Posterior stabilization of the cervicalspine using plates and screw. In : Garfin SA, Northrup BE,
eds. Surgery for Spinal Cord Injuries. New York : Raven press, 1993, pp113-122
20) Rogers W:Fractures and dislocations of the cervical spine.
J Bong Joint Surg[Am] 39 ; 341-376, 1957
21) Roy-Camile R, Gaillant G, Berteaux D:Early management
of spinal injuries. In : McKibben B, ed. Recent Advances in Or- thopedics. Edinburgh : Churchill-Livungstone, 1979, pp57-87
22) Roy-Camille R, Mazel C, Sailant G, Benazet J:Rational andtechniques of internal fixation in the trauma of the cervical spine. In : Sherk HH, Dun HJ, Eismont FJ. Eds. The Cervical spine. Philadelphia : JB Lipincott, 1989, pp163-189
23) Suterlin C, McAfee P, warden K, Rey R, Farey I:A biomech-
anical evaluation of the cervical spinal stabilization methods in a bovine model. Spine 13 : 795-802, 1988
24) Ulrich C, Woersdoerfer O, Kalff R, Claes L, Wilke HJ:Bio-
mechanics of fixation systems to the cervical spine. Spine 16 : S4-9, 1991
25) Wellman B, Follett K, Traynelis V:Complication of posterior
articular mass plate fixation of the subaxial cervical spine in 43 consecutive patients. Spine 23 : 183-200, 1998
26) Wittenberg R, Shea M, Swartz D, Lee K, White A, Hayes W:Importance of bone mineral density in instrumented spine
fusion. Spine 16 : 647-652, 1991
27) Xu R, Robke J, Ebraheim N, Yeasting R:Evaluation of cer-
vical posterior lateral mass screw placement by oblique ra- diographs. Spine 21 : 696-701, 1996
28) Zdeblick T, Zou D, Warden K, Meng R, Kunz D:Vanderby
R. Cervical stability after foramenotomy. J Bone Joint Surg
[Am] 74-A : 22-27, 1992
경추부의 후관절 나사못 고정술에서 단피질삽입법과 양피질 삽입법 간의 특성에 관한 비교
가톨릭대학교 의과대학 성빈센트병원 신경외과학교실,
1)한림대학교 의과대학 신경외과학교실
2)Department of Orthopedic Surgery,
3)State University of New York, New York
박춘근1)
·황장회2)
·지 철1)
·이재언1)
·성재훈1)
·최승진1)
이상원